INTRODUCTION
Oblique lateral interbody fusion (OLIF) was first described by Michael Mayer in 1997 [15,16] and involves minimally invasive spine access to the disc space via a corridor between the peritoneum and psoas muscle [4]. Compared to direct lateral interbody fusion (DLIF), OLIF has fewer complications related to lumbar sympathetic plexus injuries, such as anterior thigh pain, paresthesia over the thigh and groin region, and hip flexor weakness [19]. Unlike DLIF, which confirms true lateral configuration and the cage is inserted straight, during OLIF, the cage is often observed in the disc space in an oblique form.
Some studies report that it is common to see cases of cage obliquity on postoperative computed tomography (CT) or magnetic resonance imaging (MRI) with cage insertion after OLIF [3,11], In addition, in one study, the average cage obliquity was 13.0°±5.9°, and a representative moderate case was reported to be 19.1°±5.2° [3]. In particular, it was reported that the cage obliquity is greater at the L4-L5 level than at other levels [20]. As such, incorrect placement of the lateral cage resulted in : 1) impingement of the retroperitoneal vessels or nerves; 2) spillage of high concentrations of bone morphogenic protein, which is often placed into the cage to enhance fusion; 3) coronal malalignment of the segment; and 4) increased gap between the cage and vertebral endplate, which can also result in problems such as pseudoarthrosis [3,21]. Therefore, to account for instrumentation shifting, an orthogonal maneuver is required to change the cage from an oblique trajectory to a direct lateral trajectory [6].
The purpose of this study was to investigate the factors that affect cage obliquity angle despite orthogonal maneuvers and determine the relationship between cage insertion angle and radiological outcomes occurring after surgery.
MATERIALS AND METHODS
After approval from the Institutional Review Board of Armed Force Capital Hospital (No. AFCH 2022-10-004-001) was obtained, we retrospectively reviewed the medical records of patients. Informed consent was waived. We retrospectively reviewed the medical records of patients who underwent OLIF at L4-L5 from January 2019 to December 2021.
Patient enrollment
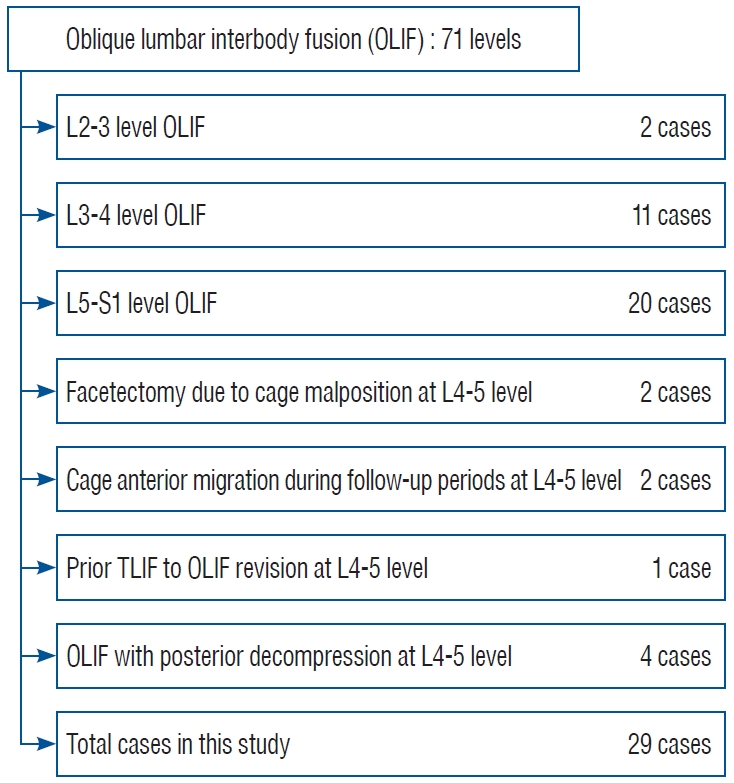
We performed a retrospective data survey of 59 patients who underwent OLIF for degenerative stenosis with or without spondylolisthesis. To minimize the influence of biomechanical differences in the lumbar vertebral site, we only included patients who underwent surgery at L4-L5. Patients with facetectomy due to cage malposition, cage anterior migration during the follow-up period, prior transforaminal lumbar interbody fusion (TLIF) to OLIF revision, and OLIF with posterior decompression, were excluded.
The indications for OLIF were as follows : 1) central stenosis with instability; 2) degenerative spondylolisthesis; 3) degenerative scoliosis; and 4) neural foraminal stenosis, confirmed by spine radiographs, CT, and MRI.
Ultimately, we enrolled 29 patients who underwent OLIF at L4-L5 (Fig. 1). These patients underwent whole spine radiographs, dynamic radiographs, lumbar spine CT, and MRI preoperatively, and at 6 months and 12 months postoperatively.
Surgical procedure and postoperative management
All operations were performed by one neurosurgeon (S.H.H.). The patients were positioned in the right local decubitus position, and then positioned using a bean bag after general anesthesia. After draping, the surgical site was confirmed with a C-arm, and an oblique skin incision of two fingers was performed in the front of the abdomen in the vertebral anterior body line. External, internal, and transverse abdominis muscles were sequentially split, and then retroperitoneal fat was observed downwards. The psoas muscle was palpated with a finger and bluntly dissected. The peritoneum was pushed forward, and by exposing the psoas muscle, the iliac blood vessels and the origin of the psoas muscle were confirmed, and blunt dissection at the origin of the psoas muscle was performed. The tubular retractor was inserted under C-arm guidance. The tubular retractor was fixed to the L4 ventral body with a fixing pin and opened to check the disc space. Annulotomy was performed based on the origin of the psoas muscle. Moreover, annulotomy was mostly conducted at the anterior third of the disc space. The intervertebral disc was removed using a shaver, endplate preparation was performed, and then cage insertion was performed. At this time, the cage was properly inserted using the orthogonal maneuver which was performed by inserting the cage at an angle first and entering the anterior one-third of the way, and then the assistant pushed the patient’s back forward and at the same time erected the cage vertically. The trapezoid-shaped polyether ether ketone cage (Clydesdale; Medtronic, Minneapolis, MN, USA) was filled with the demineralized bone matrix (Accell Connexus®; Seaspine, Carlsbad, CA, USA), allobone chip (Maxxeus, Kettering, OH, USA), and bone morphogenetic proteins (Novosis; CGBio, Seoul, Korea). After changing the patient to the prone position, using the spine table to create sufficient lumbar lordosis (LL), and confirming with the C-arm, posterior fixation was performed using the percutaneous pedicle screw system (Longitude system; Medtronic).
All patients were encouraged to ambulate from the day of surgery and were discharged 14 days after surgery. The patients were instructed to wear a lumbar-sacral orthosis for 6 months for instrumented fusion.
Clinical evaluation
To investigate changes in clinical outcomes before and after surgery, we used the immediate preoperative and 12-month postoperative visual analog scale (VAS) scores and Oswestry Disability Index (ODI) values.
Radiologic evaluation
All patients were evaluated using whole spine radiographs, preoperative static and dynamic lumbar radiographs, CT, and MRI. For follow-up, whole spine radiographs, static and dynamic lumbar radiographs, and CT were obtained 6 and 12 months postoperatively.
On whole spine radiographs, pelvic incidence, sagittal vertical axis (SVA), lumbar coronal and sagittal Cobb angles were measured preoperatively and at 6 months and 12 months postoperatively. The segmental lumbar lordotic angle (SLA), segmental lumbar coronal Cobb angle (SCA), disc anterior height (DAH), and iliac crest height were examined with standing neutral lateral radiograph imaging at L4-L5. The iliac crest height was marked with + if it invaded the disc space, and the distance between the L5 upper endplate and the furthest point where the vertical line meets the iliac crest was marked. On the other hand, cases where the iliac crest was lower than the L4-L5 disc space was marked as -, and the distance between the L5 upper endplate and the portion where the line drawn perpendicular to the iliac crest first met was measured. If the left and right heights were different in the image, and the surgical site was the left, the left pelvic height was measured in the lateral X-ray view with reference to the standing AP X-ray. The highest point of the iliac crest was chosen as the measurement site because the surgery was performed in a lateral position without bending, and the highest point was deemed to be highly reproducible during OLIF surgery at the L4-L5 level. The sagittal range of motion (lumbar flexibility) was measured using standing lateral extension and flexion radiograph imaging at L4-L5. Lumbar flexibility was calculated as the difference between the LL angle during flexion and extension in lumbar spine dynamic radiographs. Moreover, cage location ratio was measured by comparing the center of the cage and the upper endplate of the caudal vertebral body [21] (Fig. 2).
Cage obliquity angle, foraminal height (FH), fusion grade, and subsidence rate were measured using CT images. The cage obliquity angle was measured based on a line perpendicular to the line from the spinous process to the center of the intervertebral disc and a line formed by the cage metallic marker. FH was measured in sagittal view from the pedicle interior margin of the gastric vertebral body to the upper margin of the pedicle of the lower vertebral body, and the fusion grade was measured using the Bridwell fusion grade [2] (Supplementary Table 1).
On MRI, the area of the psoas major muscle of the corresponding surgical level, the total psoas muscle area index (TPAI), the distance from the iliac artery to the origin of the psoas muscle (DIAPM), and the angle between the origin of the psoas muscle and the center of the vertebral disc (APCVD) were measured. The psoas muscle area was measured using the axial cross-section of the left psoas major muscle approached during surgery on MRI at T2, and the TPAI was measured using the left and right psoas major muscle area of L3-L4 divided by the height [8,17]. The DIAPM was measured as the straight distance from the iliac artery to the point where the psoas muscle was attached to the vertebral disc [22]. The APCVD was measured as the angle between the transverse line of the intervertebral disc to the point where the psoas muscle was attached to the vertebral disc (Fig. 2).
Statistical analysis
Linear regression analysis was performed with several independent variables to determine if the measured data were related to cage obliquity. In addition, independent variables thought to affect cage obliquity were analyzed using a multiple linear regression model, and a p-value <0.05 was considered statistically significant. Estimated regression expression statistics of the cage obliquity angle were calculated with significant values from the multiple linear regression analysis.
In addition, demographic data and pre- and postoperative radiographic parameters in the two groups (a group with an obliquity angle greater than 15° and a group with an obliquity angle less than 15°) were compared. Data obtained via the radiological analysis were analyzed for statistical significance using the Student t-test. Descriptive variables were analyzed with the chi-square test or Fisher exact test. The results are presented as mean±standard deviation. Variables with p<0.1 in the univariate analysis were used in the multivariate analysis. Moreover, we used receiver-operating characteristic (ROC) curves to assess the predictability cutoff values.
Statistical analysis was performed using IBM SPSS statistics for Windows version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The cage obliquity angle in patients who underwent OLIF surgery at L4-L5 during March 2019 to December 2021 was 15.1°±5.7° (range, 5.8°-27.5°). All patients included in the study were male and the mean age was 44.8±8.9 years (range, 19-58). The average body mass index (BMI) of the patients was 26.9±3.4 (range, 21.1-33.2), the psoas muscle volume encountered at surgical approach was 20.8±3.5 (range, 13.0-26.5), and the TPAI, an approximate indicator of skeletal muscle mass, was 10.2±1.8 (range, 7.6-13.5). The DIAPM was 14.8±5.2 mm (range, 4.9-25.3) and the APCVD was 22.7°±7.3° (range, 9.3°-43.4°). In standing neutral lateral radiograph imaging at L4-L5, the iliac crest height was -1.3±9.4 mm (range, -12.5 to 15.7), and in standing dynamic radiograph imaging, L4-L5 flexibility (flexion-extension angle) was 13.4°±6.6° (range, 1.8°-28.6°). The cage angles used were 6º and 12º, and the cage heights used were 10, 12, 14, and 16 mm (Table 1).
Radiological measurements
The cage obliquity angle measured at 12 months postoperatively was 15.1±5.7 (range, 5.8-27.5). The SLA, SCA, DAH, and FH changes were increased by 1.8°±4.2°, -0.47°±1.8°, 4.2±2.7 mm, and 5.4±3.3 mm on average, respectively. The changing pattern of SLA compared to the cage angle used (postoperative index level SLA - used cage angle) and the changing pattern of disc height compared to the cage height used (postoperative index level DAH - used cage height) were -0.4°±3.5° and -0.1°±1.9°, respectively, and the average fusion grade was 1.7±0.5 (Table 2).
There was no statistically significant difference in LL (L1-S1) and SVA preoperatively versus 12 months postoperatively, and SLA did not change statistically but tended to increase. However, DAH (8.4±3.6 vs. 12.8±2.2 mm, p<0.05) and FH (17.8±2.8 vs. 23.2±3.1 mm, p<0.05) showed statistically significant increases preoperatively versus 12 months postoperatively (Table 3).
Single and multiple regression analysis
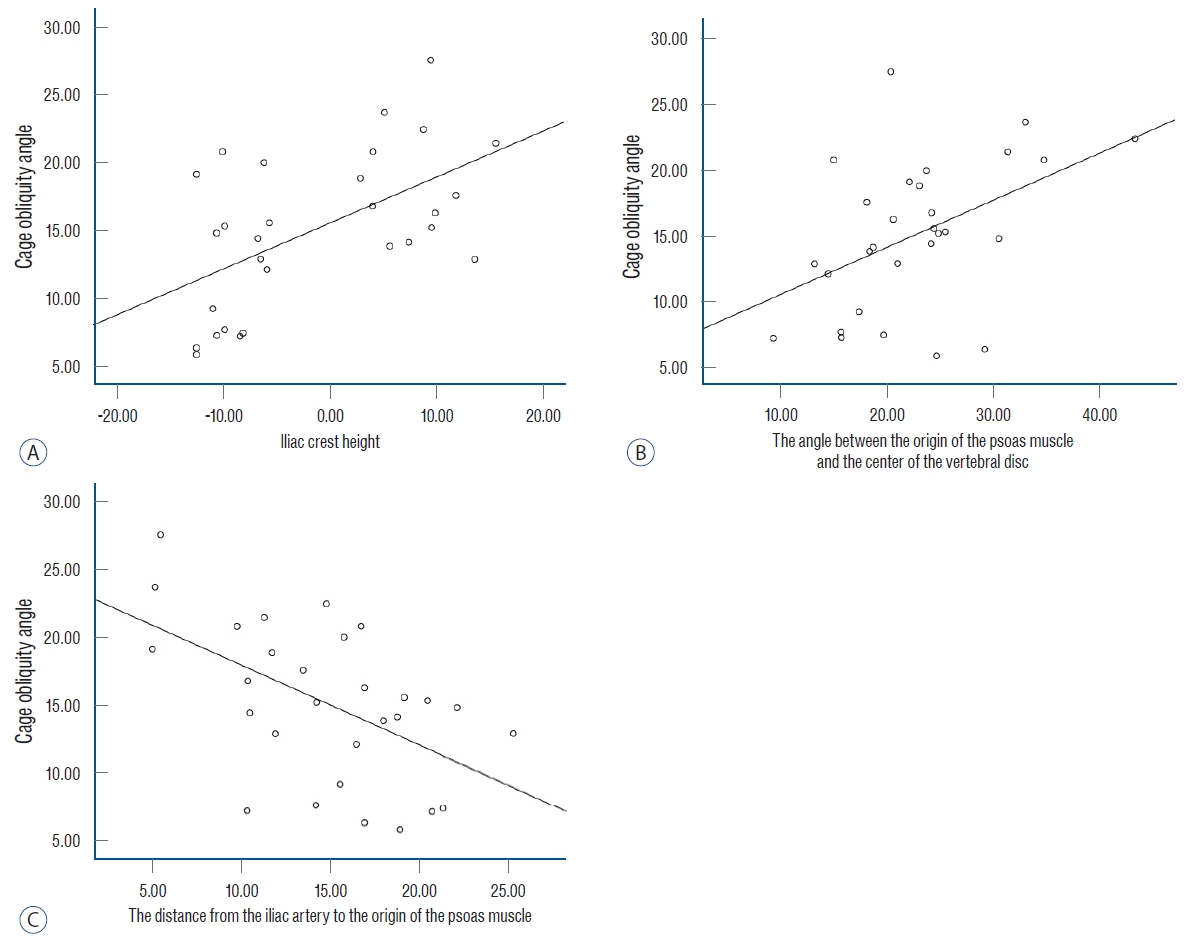
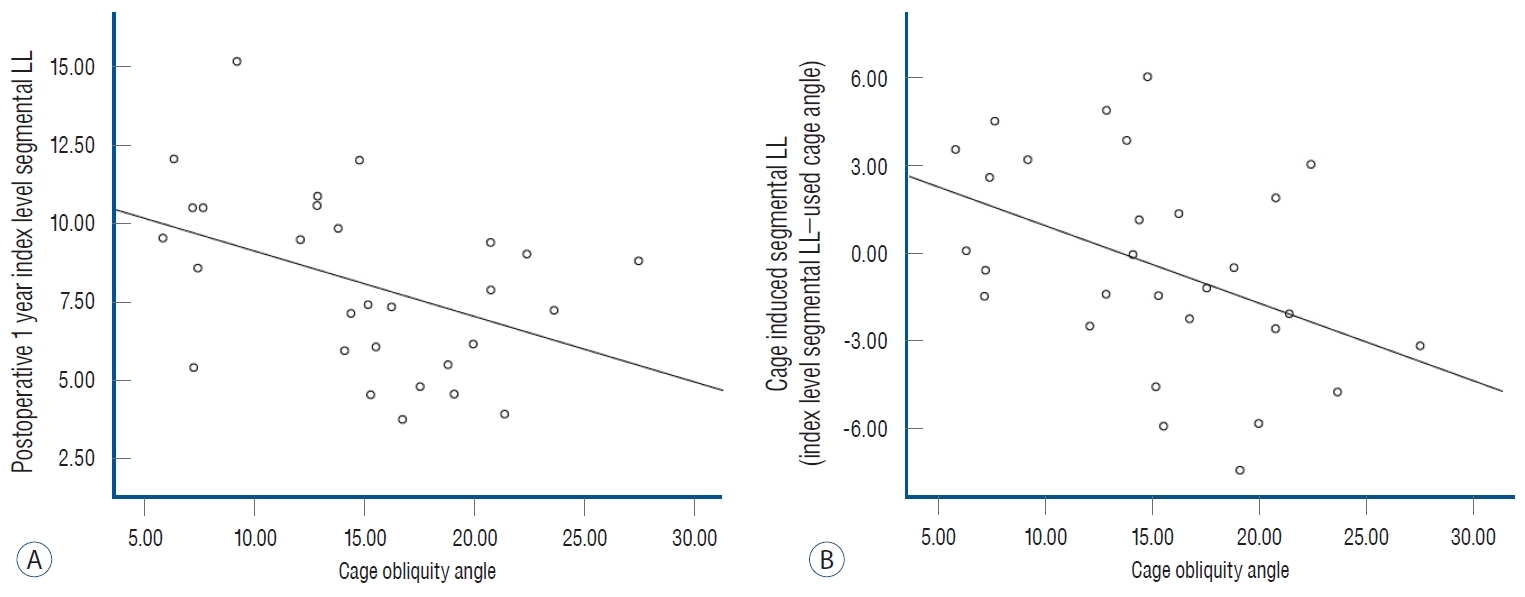
A single linear regression analysis was performed for each of the factors thought to affect cage obliquity angle, revealing that DIAPM, APCVD, and iliac crest height were three factors that were significantly correlated with cage obliquity angle (R2=0.28 and p=0.003, R2=0.21 and p=0.012, and R2=0.31 and p=0.002, respectively) (Fig. 3). Moreover, the 12 month-postoperative index level SLA and cage-induced segmental LL were significantly affected by cage obliquity angle (R2=0.18 and p=0.02 and R2=0.19 and p=0.02, respectively) (Table 4 and Fig. 4).
As a result of multiple linear regression analysis of factors thought to affect cage obliquity angle, these three factors were also statistically significant : DIAPM, APCVD, and iliac crest height. The variance factor (the Durbin-Watson factor) was 2.418 and the adjusted R2, indicating explanatory power, was 0.551. Based on this, the equation to predict the preoperative cage obliquity angle was calculated as : cage obliquity angle = 13.062-0.318×DIAPM+0.325×APCVD+0.174×iliac crest height (Table 5). The correlation analysis between DIAPM, APCVD, and iliac crest height, which appear to affect cage obliquity, was not statistically significant (Table 6).
Statistical comparison by artificially dividing participants into two groups
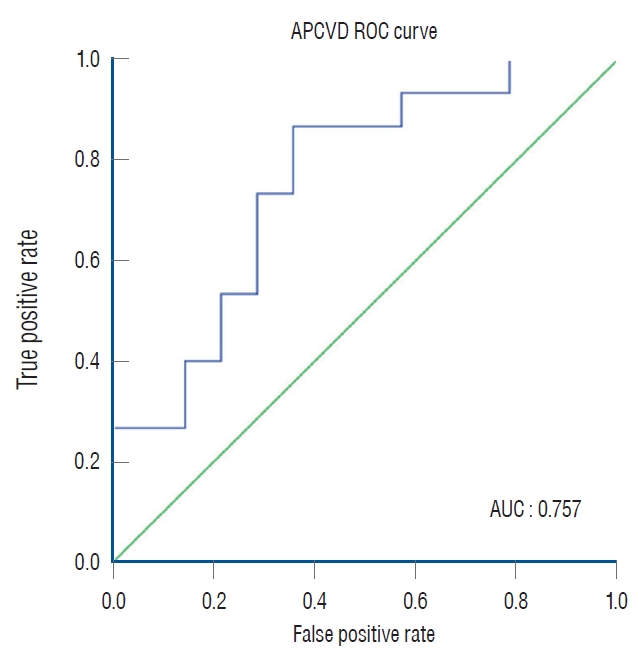
The study divided the participants into two groups based on the mean cage obliquity angle of 15° : the small cage obliquity angle group (n=14) and the large cage obliquity angle group (n=15). The cage obliquity angle in each group was 10.4°±3.4° and 19.4°±3.5°, respectively (p<0.05). There were statistically significant differences in preoperative DIAPM, APCVD, and iliac crest height between the two groups. Additionally, postoperative 1-year index level SLA and cage-induced segmental LL demonstrated significant differences of 9.8°±2.6° versus 6.4°±1.9° and 1.7°±2.7° versus -2.4°±3.0°, respectively (Table 7). In univariate analysis, all three variables, DIAPM, APCVD, and iliac crest height, showed statistically significant differences. However, in multivariate analysis, only APCVD demonstrated a significant value (Table 8). The area under the ROC curve of the APCVD was 0.757, When the cutoff value of the APCVD was calculated at 21.58°, and the sensitivity and specificity were 73.3% and 71.4%, respectively (Fig. 5).
Clinical outcomes
At 12 months postoperatively, back and leg VAS and ODI values showed improvement (Supplementary Table 2). However, none of these values were related to the cage obliquity angle (Table 6).
Intra-rater and inter-rater reliabilities
For all radiological parameters, the intra-rater correlation coefficient was greater than 0.88 and the inter-rater correlation coefficient was greater than 0.82, and therefore, the mean values of the four measurements were used for the present study (e.g., intraclass correlation coefficient of the iliac crest height [2,2], 0.907; 95% confidence interval, 0.827-0.949; p<0.001).
DISCUSSION
It is widely known that OLIF fusion surgery is a surgical method that can further minimize lumbar plexus injury compared to DLIF [1]. In OLIF, unlike DLIF, the cage is inserted diagonally into the disc space, usually based on fluoroscopic imaging of the C-arm during surgery. In this procedure, an orthogonal maneuver is performed to enable the cage to be inserted in a vertical direction similar to DLIF, without generating cage obliquity at the disc space. However, it is uncommon for the cage obliquity angle to converge to 0° with OLIF. In some studies, the reported cage obliquity angle reached 13.0°±5.9° [3,19], and one more advanced study reported it as 11.3°±6.9° and that cage obliquity angle was greater at the L4- L5 level than at other levels (13.4°±6.4°) [20]. In this study, the average cage obliquity angle was measured at 15.1°±5.7° (range, 5.8°-27.5°) at L4-L5 level in lumbar spine CT images performed after surgery.
Cage obliquity can cause several problems. Radiculopathy may be caused by a large cage and incorrect position due to cage obliquity [11]. In addition, concerns such as spillage of high concentrations of bone morphogenic protein, which is often placed in cages to enhance fusion, coronal malalignment of the segment, and pseudoarthrosis due to an increased gap between the cage and vertebral endplate may arise, and research on this is still lacking [3,14,21]. However, in some studies, it has been shown that cage obliquity has no effect on indicators such as postoperative bone union rate, differing degrees of foraminal decompression between right and left side neural foramen, and VAS and ODI score improvement [3,9,14]. These results are consistent with that of our study, and patient clinical outcomes and fusion grades were not correlated with cage obliquity (Tables 4 and 6).
Although there have been studies on the factors affecting cage obliquity, previous studies on the effects of orthogonal maneuvers are scarce. In this study, we considered whether factors influencing cage obliquity would be affected by the cage insertion entry point, cage insertion trajectory, and interfering factors during orthogonal maneuvers. In terms of studies on cage insertion entry points, there has been one study on surgical corridors in OLIF. According to this study, the position of the psoas major muscle and iliac artery or aorta in humans may be sufficiently different. In this study, the positions of the iliac artery and psoas muscle were categorized into six vertical zones (A, I, II, III, IV, P) and four horizontal zones (R, a, b, c, L), resulting in a total of 14 types. Our patients were classified as type Aa, Ab, Ac, Ib, and Ic, and their distribution is illustrated in Fig. 6 [22]. The results of this study align with the fact that the distance between the psoas major muscle where it is attached to the disc and the major blood vessel is an important factor. At this time, even though the psoas major muscle is dissected from the intervertebral disc, the orthogonal maneuver cannot be properly performed because excessive movement in a narrow space of the surgical corridor is unlikely to damage blood vessels or damage anterior longitudinal ligaments and cause cage malposition.
In addition, the APCVD was taken into account considering the fact that the cage insertion trajectory enters toward the disc space midline during cage insertion before the orthogonal maneuver. This was a factor influencing cage obliquity and was significantly correlated. When divided according to a mean cage obliquity angle of 15°, APCVD stood out as the only significant risk factor, indicating that it potentially exerts the highest impact among the three factors (DIAPM, APCVD, iliac crest height) investigated in this study.
Interfering factors during orthogonal maneuvers included psoas muscle volume at the index level, TPAI reflecting approximate skeletal muscle, BMI reflecting obesity, disc height reflecting preoperative disc space collapse, and lumbar flexibility at the index level which reflects the leverage effect and that cage vertical movement can occur more easily during cage insertion [7,8]. However, none of these were statistically correlated with cage obliquity. This study was limited to the L4- L5 level only, and unlike other levels of L2-L4, the iliac crest acts as an interfering factor during orthogonal maneuvers [10]. In several studies, surgery may be difficult due to the relationship between the location of the iliac crest and L4-L5 level, and in some cases, a surgical method for removing some of the iliac crest is also suggested [5,18]. In this study, the effect on the iliac crest and the possibility of a failed orthogonal maneuver due to the iliac crest was considered. As shown in Tables 4 and 5, the cage obliquity was affected by the iliac crest.
In addition, in this study, the induced cage obliquity angle was found to be a significant result among the values found to be influenced by cage obliquity. This is evaluated as the difference between the originally used cage angle and the segmental LL angle we obtained after surgery, and this value decreased as the cage obliquity increased. This means that as the cage obliquity increases, the SLA that we can obtain after surgery is small compared to the cage angle used. Similarly, other studies have shown that the SLA increases when the cage angle is horizontal rather than oblique during TLIF [12-14]. This implies that as the cage approaches a horizontal position, the contact area between the vertebral body and the endplate increases in the horizontal direction, allowing the original cage angle to be achieved and promoting the creation of LL.
Therefore, by dissecting slightly further from the psoas muscle origin point and placing the entry point more inward, along with a reduced trajectory angle, cage obliquity can be minimized. Additionally, considering the individual iliac crest height of each patient before surgery, surgeons can anticipate and strive to achieve the desired segmental LL angle, thus minimizing cage obliquity.
Limitations
The present study has several limitations. First, this was a retrospective study involving a small number of patients, which may have affected the strength of the results of the statistical analysis. Second, this study included only male patients who were soldiers and officers on active military duty under the age of 60 years (range, 19-58), and the design of the present study meant that there was a chance of selection bias. In the future, large-scale studies including the elderly and women are needed to overcome the limitations of this study which focused only on men. Nevertheless, the present study makes a significant contribution in that it identified factors that influence cage obliquity and factors that are affected by cage obliquity in OLIF at the L4-L5 level.
CONCLUSION
In OLIF at the L4-L5 level, cage obliquity was not correlated with the patient’s skeletal muscle mass or psoas muscle volume, but was correlated with DIAPM and APCVD, indicating a correlation with cage entry point and trajectory. Moreover, the iliac crest height was affected during orthogonal maneuvers. There was no correlation with changes in clinical outcome, fusion grade, and foramen height changes according to the degree of cage obliquity. However, the more severe the cage obliquity, the less segmental LL was produced at the index level, and less segmental LL was produced than the intended cage angle used by the surgeon. To prevent these issues, it is recommended that the three mentioned factors (DIAPM, APCVD, and iliac crest height) are considered and that orthogonal maneuvers are performed during surgery. A longterm follow-up study with a large number of patients is necessary to provide further evidence of the effectiveness of cage obliquity in OLIF.