Real-Time Visualization of Thrombus during Suction Thrombectomy : Contrast-in-Stasis Technique
Article information

Abstract
This report introduces a simple method to visualize the captured thrombus in real-time during suction thrombectomy using “contrast-in-stasis technique”. It enables visualization of the thrombus captured by a suction catheter as it is being retrieved through the tortuous course of the carotid artery eventually into the guiding catheter. It also offers visual identification of important findings such as fragmentation of thrombus into pieces or loss of thrombus during retrieval, and, therefore, helps clinicians to make further critical decisions during the procedure.
INTRODUCTION
Technical innovations within the last few decades have made a major breakthrough in the field of endovascular surgery for the treatment of acute ischemic stroke. Both recanalization rate and procedure time for the recent techniques are incomparable to ones for classic techniques decades ago. Currently, suction thrombectomy is one of the fastest and simplest methods to achieve recanalization [1,3]. Using the negative pressure from a syringe passed through a suction catheter, a whole block of thrombus can be captured or aspirated at once. However, the thrombus can be broken into pieces and only one fragment may be captured, or even lost during the retrieval through the tortuous course of the carotid artery. If the remaining thrombus luckily stays on the arterial wall, it may be captured by additional maneuvers. If not, fragmented thrombi may migrate distally into smaller branches resulting in a more difficult situation to deal with. The clinicians tend to rely on the subjective sensation of their hands as well as the status of negative pressure in the syringe to tell whether the thrombus stays still on the tip of a suction catheter or it is lost during the retrieval. Real-time visual identification of the thrombus, if possible, enables clinicians to evidence that the thrombus captured by a suction catheter is being retrieved stably through the tortuous course eventually into the guiding catheter. This report introduces a simple method for the real-time visualization of the captured thrombus during suction thrombectomy using “contrast-in-stasis technique”.
TECHNICAL PROCEDURES
This study was approved by the Institutional Review Board of Daegu Fatima Hospital (IRB 2023-07-006).
A balloon-mounted guiding catheter is mandatory for this technique, and 9 French Optimo (Tokai, Aichi, Japan) is mostly used in our institute. It is located stably at the proximal internal cerebral artery (ICA). Then, a suction catheter is prepared. React 68 (Medtronic, Minneapolis, MN, USA) and Penumbra ACE 68 (Penumbra Inc., Alameda, CA, USA) are frequently used in our institute, but any other large bored catheters, including intermediate guiding catheters, can be utilized. A tortuous carotid siphon and a prominent origin of arterial branches such as the ophthalmic artery and posterior communicating artery can be obstacles that interfere with smooth advancement of a suction catheter. Creating a curve at the tip of a suction catheter by steam-shaping is highly recommended to overcome these obstacles and, therefore, to enhance its distal accessibility. A coaxial microcatheter, as well as a microwire, can be also used if necessary. Temporary balloon inflation of a balloon-mounted guiding catheter enhances the supporting power by holding the tip of the guiding catheter tightly in place at the proximal ICA, thereby making the distal access easy as well. In most cases of the ICA occlusion and some cases of the middle cerebral artery (MCA) occlusion with hypoplastic proximal branches, the artery tends to be stagnated without an antegrade blood flow, and the occlusion point often cannot be visualized by a subtraction angiography with guiding catheter injection (Fig. 1). To confirm the exact occlusion points in these specific situations, contrast can be injected continuously and gently via a suction catheter while it is being advanced distally (Fig. 2). However, in the majority of cases, proximal branches and perforators exist allowing antegrade flow nearly up to the occlusion point, and subtraction angiography clearly shows the lesion. Before reaching the occlusion point, the balloon on the guiding catheter is inflated to arrest the blood flow and contrast media is infused gently via the guiding catheter to fill up the ICA. Contrast is also injected gently via the suction catheter, and the proximal margin of thrombus is identified. As soon as the tip of suction catheter reaches the lesion and is wedged to the thrombus, a strong negative pressure is generated using a 50 mL syringe (Fig. 3). The suction pressure is transmitted solely on the thrombus, and the contrast stays still in the artery proximal to the occlusion point. Some of the contrast may wash away at the portion nearby the patent branches proximal to the occlusion point. Additional contrast can be infused anytime via the balloon-mounted guiding catheter to enhance the visuality. While the suction catheter is gently being retrieved, captured thrombus is visualized in real-time until it is pulled down fully into the guiding catheter (Fig. 4). When the whole block of thrombus is captured and occluded artery is recanalized, some of the stagnated contrast in the distal portion may instantly wash away as the thrombus is being pulled down. Since there are no prominent branches throughout the course of the ICA from the proximal balloon to the ophthalmic artery, that segment usually remains fully filled up with contrast and, therefore, the thrombus captured on the tip is visualized well. When the suction catheter is retrieved without any thrombus captured, no thrombus on the tip is visualized on the fluoroscope and, at the same time, the stagnated contrast rapidly disappears being aspirated by the suction catheter (Fig. 5). Thrombus in atypical shape or with huge burden can also be identified in real-time (Figs. 6 and 7). It enables visual confirmation of important findings such as fragmentation of thrombus into pieces, loss of thrombus during retrieval, or the captured thrombus being aspirated through the suction catheter. If retrieval of the thrombus is not evidenced, the balloon on the guiding catheter should not be deflated until the completion of additional thrombectomy in order to prevent distal migrations. For every single maneuver of thrombectomy, the guiding catheter must be cleared up thoroughly and maintained free from the possible remnant of thrombus debris prior to the acquisition of the following angiogram. This eliminates the risk of inadvertent migration of the thrombus which may remain in the guiding catheter. Supplementary Video 1 demonstrates some examples of procedures using contrast-in-stasis technique which include confirmation of the occlusion point and real-time visualization of the captured thrombus in various situations, as well as a table of example cases with the clinical information.

Anterior-posterior (A) and lateral (B) views of carotid angiogram of a patient with the left internal carotid artery terminal occlusion show stagnation of contrast without an antegrade blood flow. Note that the occlusion point cannot be visualized by a subtraction angiography with guiding catheter injection.
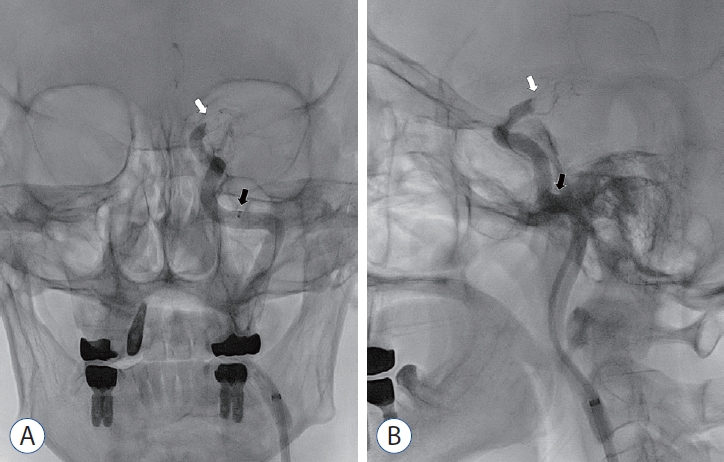
Anterior-posterior (A) and lateral (B) views of non-subtraction carotid angiogram show the exact occlusion point (white arrows) at the left internal carotid artery terminum. Contrast is injected continuously and gently via a suction catheter (black arrows) while it is being advanced.

A 50 mL syringe is set up with its plunger fixed by a 20 mL syringe to generate a strong negative pressure.

Serial images (A-C) of non-subtraction angiogram using “contrast-in-stasis technique” for a patient with the distal internal carotid artery occlusion show the captured thrombus (black arrowheads) in realtime as it is being retrieved through the tortuous course of the carotid artery into the guiding catheter.
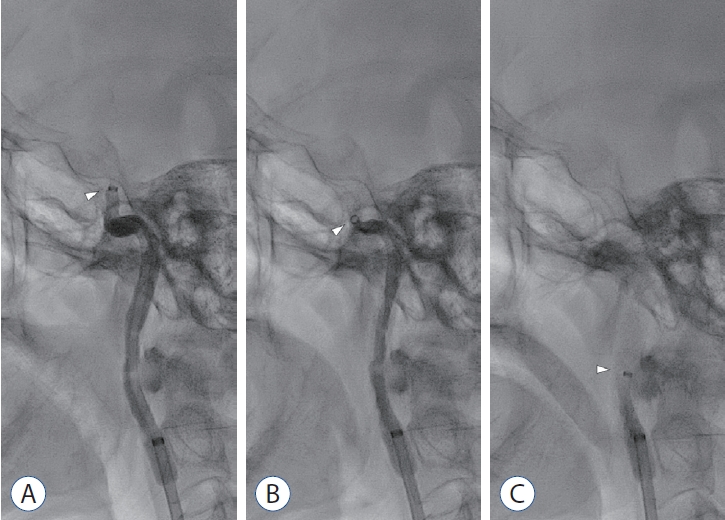
Serial images (A-C) of non-subtraction angiogram using “contrast-in-stasis technique” show that, when the suction catheter is retrieved without any thrombus captured, no thrombus is visualized on the tip of the suction catheter (white arrowheads) and, at the same time, the stagnated contrast rapidly disappears being aspirated by the suction catheter.

Serial images (A-D) of non-subtraction angiogram using “contrast-in-stasis technique” for a case of the cervical internal carotid artery occlusion show that the whole block of thrombus in a complex shape (black arrowheads) is being retrieved stably into the guiding catheter. The photograph (E) shows the retrieved thrombus.
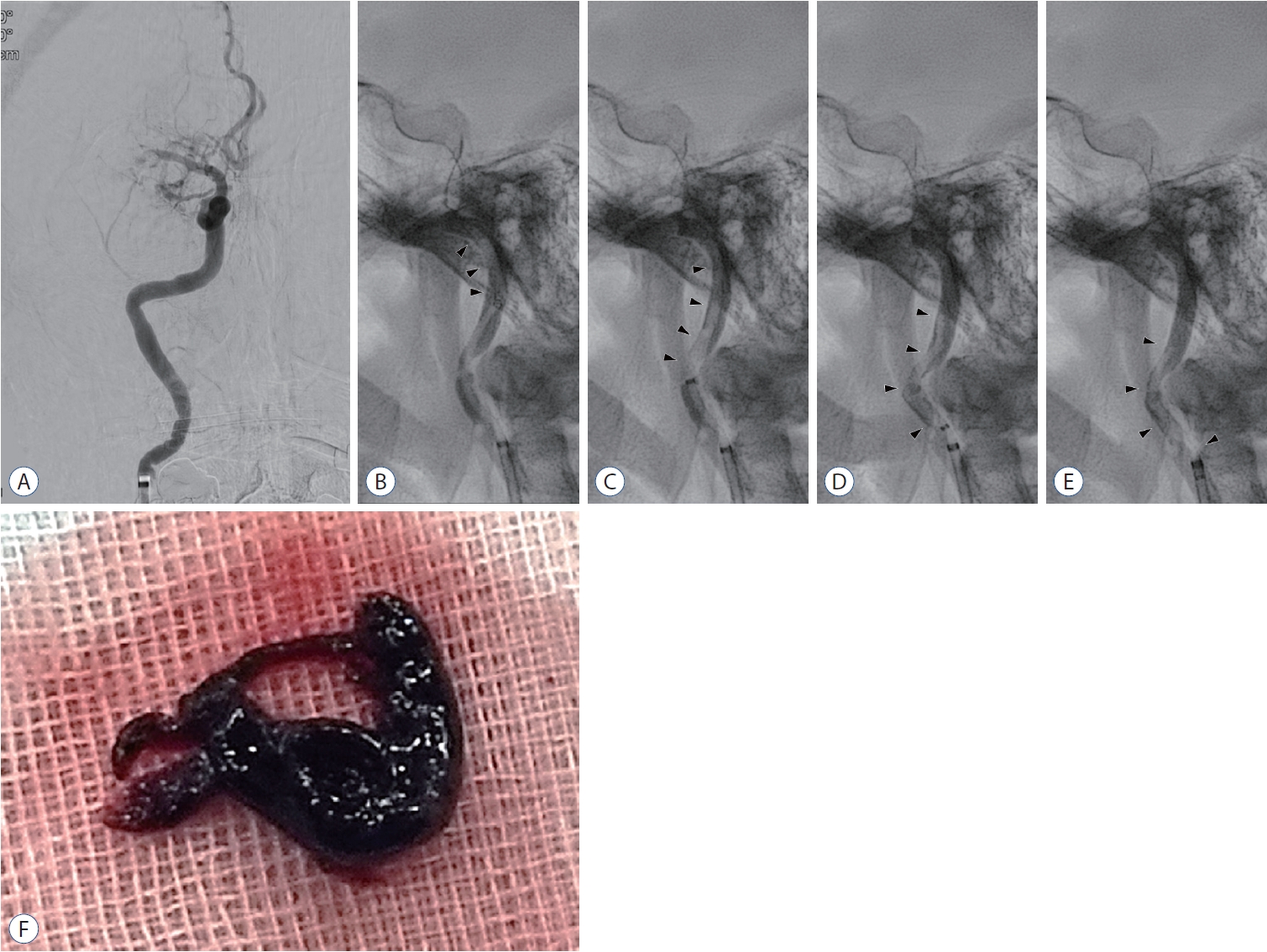
Right carotid angiogram (A) of a patient with a typical middle cerebral artery infarction shows an occlusion of the middle cerebral artery. However, serial images (B-E) of non-subtraction angiogram using “contrast-in-stasis technique” show that an extremely long thrombus with huge burden (black arrowheads) is being retrieved stably into the guiding catheter. The photograph (F) shows the retrieved thrombus.
DISCUSSION
Due to low recanalization rates as well as significant hemorrhagic risks of classical old-fashioned thrombolysis techniques using microwire, so-called mechanical thrombolysis in the past was indicated only for those with proven penumbra zone after detailed but time-consuming evaluation on perfusion status prior to the initiation of an endovascular procedure. Introduction of suction thrombectomy, stent retrieval, and combination of these two techniques has brought major impact on changes of treatment paradigm for hyperacute ischemic stroke caused by large vessel occlusion. Their high recanalization rates have naturally influenced recent trends to shorten the pre-procedural time by omitting detailed imaging studies if the patients meet the adequate indication at early time-window [2]. On the other hand, pre-procedural information on the size or extent of thrombus is not acquired sufficiently. Clinicians do not actually know how heavy the thrombus burden is and whether the whole thrombus is captured and it is being retrieved stably without being lost until it is completely pulled out. Moreover, since the clinical outcome of thrombectomy is strictly time-dependent, many clinicians prefer a local anesthesia instead of general. Acutely ill patients are often irritable even in sedative states and their continuous movements make it difficult to acquire subtraction images, thus requiring repeated trials with additional radiations. Roadmap images also may not be not utilizable under conditions with severe motion artifacts. “Contrast-in-stasis technique” introduced in this report requires neither subtraction nor roadmap images, and it offers real-time visualization of both the captured thrombus and artery overcoming the continuous motion of patients during suction thrombectomy. It may also reduce the amount of contrast used and radiation exposure by preventing repeated trials, and, as a result, shorten the overall procedural time. This technique is also applicable to cases using combined suction thrombectomy and stent retrieval if the suction catheter is adequately wedged to the thrombus captured by the stent. Currently, balloon-mounted guiding catheters are commonly used in thrombectomy since they are related with not only prevention of distal migrations of the thrombus but also higher successful recanalization rate and first-pass recanalization rate4). For utilization of “contrast-in-stasis technique”, no additional endovascular devices or instruments are required, but a commonly used balloon-mounted guiding catheter and contrast are the only requisites.
However, there exist some limitations for this technique. With recent trends using a large bored suction catheter that nearly fits into the diameter of the MCA, visualization of thrombus in the MCA often cannot be possible once the suction catheter is advanced into the MCA and wedged to the thrombus. If branches proximal to the occlusion point are prominent, stagnated contrast tends to wash away at the portion nearby the patent branches, and additional contrast should be infused via the balloon-mounted guiding catheter to enhance the visuality. Nevertheless, the ICA from the proximal balloon to the ophthalmic artery usually remains fully filled up with contrast since there are no prominent branches, and the status of the thrombus can be visualized clearly in real-time. This segment has the most tortuous course and captured thrombus can be frequently lost when the catheter tip shakes and bumps against the arterial wall during the retrieval. Therefore, this technique can be especially useful for cases of the ICA occlusion in which the artery already tends to be stagnated without an antegrade blood flow due to a thrombus in complex shape or with huge burden.
CONCLUSION
“Contrast-in-stasis technique” offers real-time visualization of a captured thrombus during suction thrombectomy overcoming the continuous motion of patients. Based on the realtime visualized information acquired by this technique, clinicians can make critical decisions such as when to deflate the balloon on the guiding catheter or whether additional maneuver of thrombectomy is required.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Informed consent
This type of study does not require informed consent.
Author contributions
Conceptualization : YSL; Data curation : YSL; Formal analysis : YSL; Methodology : YSL; Project administration : YSL; Visualization : YSL; Writing - original draft : YSL; Writing - review & editing : YSL
Data sharing
None
Preprint
None
Supplementary materials
The online-only data supplement is available with this article at https://doi.org/10.3340/jkns.2023.0158.
This video demonstrates some examples of procedures using contrast-in-stasis technique which include confirmation of the occlusion point and real-time visualization of the captured thrombus in various situations, as well as a table of example cases with the clinical information. Since the procedures are carried out rapidly, each video clip loops three times.