Diffusion-Weighted Magnetic Resonance Imaging in the Diagnosis of Cerebral Venous Thrombosis : A Meta-Analysis
Article information

Abstract
Objective
A role of diffusion-weighted imaging (DWI) in the diagnosis of cerebral venous thrombosis (CVT) is not wellunderstood. This study evaluates the effectiveness of DWI in the diagnosis of CVT.
Methods
Literature search was conducted in electronic databases for the identification of studies which reported the outcomes of patients subjected to DWI for CVT diagnosis. Random-effects meta-analyses were performed to achieve overall estimates of important diagnostic efficiency indices including hyperintense signal rate, the sensitivity and specificity of DWI in diagnosing CVT, and the apparent diffusion coefficient (ADC) of DWI signal areas and surrounding tissue.
Results
Nineteen studies (443 patients with 856 CVTs; age 40 years [95% confidence interval (CI), 33 to 43]; 28% males [95% CI, 18 to 38]; symptom onset to DWI time 4.6 days [95% CI, 2.3 to 6.9]) were included. Hyperintense signals on DWI were detected in 40% (95% CI, 26 to 55) of the cases. The sensitivity of DWI for detecting CVT was 22% (95% CI, 11 to 34) but specificity was 98% (95% CI, 95 to 100). ADC values were quite heterogenous in DWI signal areas. However, generally the ADC values were lower in DWI signal areas than in surrounding normal areas (mean difference−0.33×10-3 mm2/s [95% CI, −0.44 to −0.23]; p<0.00001).
Conclusion
DWI has a low sensitivity in detecting CVT and thus has a high risk of missing many CVT cases. However, because of its high specificity, it may have supporting and exploratory roles in CVT diagnosis.
INTRODUCTION
Cerebral venous thrombosis (CVT) is a distinct cerebrovascular disease which accounts for approximately 1–2% of all adult stroke cases [19]. It has an annual incidence of 3–4 cases per million in adults and up to seven cases per million in children [30]. CVT mostly affects individuals aged 20–50 years and less than 10% victims are over 65 years of age. Females have a 3-fold greater risk of developing CVT [29]. Among the risk factors for CVT incidence, heridetary thrombophilia, inflammatory disorders and cancer, pregnancy, diabetes, and oral contraceptive use are more important [4]. The presentation is usually subacute as symptoms evolve over days to weeks. Commonly associated symptoms include headache, focal neurologic deficits, seizures, altered consciousness, obscuration of vision, nausea, vomiting, papilledema, cranial nerve palsies and coma [27].
Diagnosis of CVT is difficult because clinical manifestations are often nonspecific and relies mainly on neuroimaging findings which may also provide information about flow dynamics of affected area [32]. Because a thrombus develops with time and can be associated with recanalization such as the chronic partially recanalized dural sinus thrombosis, neuroimaging methods can have a compromised output [17]. In general, a diagnosis based on T2-weighted imaging (T2WI) in combination with magnetic resonance venography (MRV) is recommended as the first line modality [12,35]. Besides leaving a hyperintense signal on T2WI, a thrombus in cerebral vein or sinus may also produce a hyperintense signal on diffusionweighted imaging (DWI) [34]. DWI is a method of magnetic resonance imaging (MRI) technology which quantifies Brownian motion of water and is highly sensitive in detecting acute arterial strokes and distinguishing cytotoxic and vasogenic edema.
The efficiency of DWI for the diagnosis of CVT is evaluated by several authors of retrospective studies [19-23]. However, the outcomes are considerably heterogenous which necessitates a systematic review of this area. The aim of the present study was to undertake a literature survey for the identifications of relevant studies and to perform a meta-analysis of important indices which can provide a refined evidence of the efficiency of DWI in diagnosing CVT.
MATERIALS AND METHODS
All analyses were based on previously published studies; therefore, no ethical approval or patient consent were required.
Inclusion criteria
The inclusion criteria were: the study — 1) evaluated the efficiency of DWI in the diagnosis of CVT; and 2) reported one or more relevant endpoint/s including the rate of hyperintense signal detection by DWI, area under receiver operator curve (AUROC) parameters for DWI utility in diagnosis CVT, and apparent diffusion coefficient (ADC) values of areas with and without DWI signal in patients with CVT.
Literature search
Electronic databases (EMBASE, Google Scholar, Ovid SP, and PubMed) were searched for the acquisition of research articles reporting the outcomes of diagnostic performance/utility of DWI for CVT. Literature search was carried out by using important keywords in logical combinations. These included cerebral venous thrombosis, CVT, vein, sinus, clot, stroke, hemorrhage, edema, occlusion, magnetic resonance imaging, MRI, diffusion-weighted imaging, DWI, apparent diffusion coefficient, ADC, hyperintense signal, area under operator receiver curve (AUROC), specificity, sensitivity, diagnosis, and diagnostic accuracy. Database software suggested articles and cross references of important literary sources were also examined.
Data extraction, synthesis, and statistical analysis
Relevant data (demographic, clinical, and pathological characteristics of the patients, study design and dates, technical details of the procedures, outcome measures and outcomes) were extracted from published research articles of respective studies and were organized in specialized datasheets. For achieving the pooled estimates of percent DWI hyperintense signals and AUROC parameters, the meta-analysis of proportions with Freeman-Tukey double arcsine transformation were performed with Stata software (version 12; Stata Corporation, College Station, TX, USA). For the evaluation of the significance of difference between DWI measured ADC of thrombosed sites and normal brain areas, a meta-analysis of mean differences was performed with RevMan software (version 5.3; Cochrane, Copenhagen, Denmark) under random effects model. Between-study inconsistency was tested with I2 index. Publication bias assessment was performed with Egger’s regression asymmetry test and trim and fill method was used to estimate the number of possible missing studies.
RESULTS
Nineteen studies were included (Fig. 1). The literature search identified 872 abstracts but vast majority (n=840) had to be excluded based on irrelevancy of title/abstract. Thirty-two research articles were found to have relevant text/data and were downloaded from databases. After the observance of eligibility criteria, 19 research articles were found useful for the current study. Studies that used DWI for other purposes such as characterizing cytotoxic or vasogenic edema; studies that used DWI and other diagnostic modalities but did not report results for each method separately; studies published in a non-English language; and review articles were excluded.
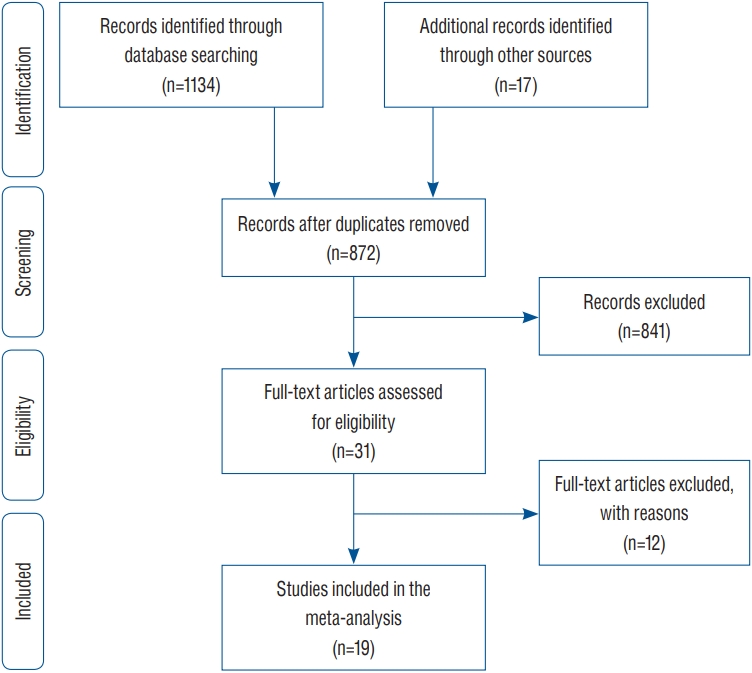
A flowchart of study screening and selection process.
Among the included studies, 16 were retrospective in desig ns [2,3,6,8,10,11,13,18,20-23,25,26,36,37] and three were the case reports [7,15,33]. In all, 443 patients with CVT were subjected to DWI examinations in these studies. Total number of CVTs studied was 856. Important characteristics of the included studies are presented in Table 1. Study of a funnel plot corresponding to the meta-analysis of pooled incidence of hyperintense signal on DWI indicated the possibility of some missing studies (Fig. 2). Egger’s regression asymmetry test also showed significant publication bias (coefficient : 4.46 [95% confidence interval (CI), 2.31 to 6.60]; p=0.001).
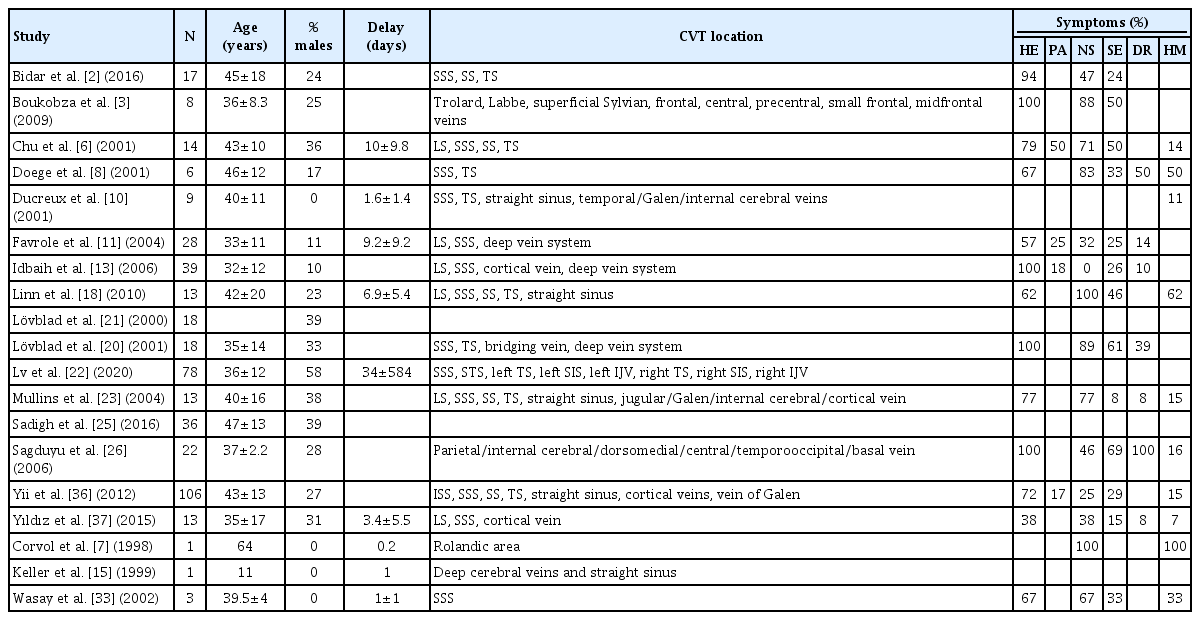
Important characteristics of the included studies
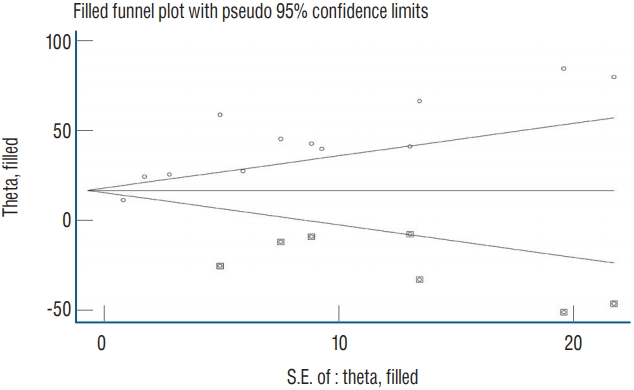
A funnel plot corresponding to the meta-analysis of diffusion-weighted imaging hyperintense signal rate showing the outcomes of trim and fill method of publication bias assessment. Circles show studies included in the meta-analysis whereas circles within squares show possible missing studies. S.E. : standard error.
Age of these patients was 40.1 years (95% CI, 33.1 to 43.1) and 28% (95% CI, 18 to 38) of these patients were male. Delay time from onset of symptoms to DWI was 4.61 days (95% CI, 2.3 to 6.9). Major symptoms in these patients were: headache 76.4% (95% CI, 62.6 to 90.3), neurological deficits 71.6% (95% CI, 56.0 to 87.2), seizures (33.6% [95% CI, 24.7 to 42.5]), hemiparesis 32.3% (95% CI, 25.2 to 39.3), papilledema 27.2% (95% CI, 19.3 to 35.1), and drowsiness (21.0% [95% CI, 13.8 to 28.3]).
Eighty-two percent of cerebral thromboses were found in sinuses and 18% in veins. Among the sinuses, the incidence of thrombosis was 28% in superior sagittal sinus, 37% in lateral/transverse sinus, 13% in sigmoid sinus, 4% in straight sinus, and 0.74% in inferior sagittal sinus. Among the cortical veins, the incidence of thrombosis was 0.55% in frontal vein, 0.37% in Trolard vein, 0.37% in Labbe vein, and 0.2% in superficial Sylvian vein. Within the deep cerebral veins, the incidence of thrombus was 1% in vein of Galen and 0.56% in internal cerebral vein. Moreover, the thrombus incidence was 0.37% in jugular vein, 0.2% in central vein and 0.2% in precentral vein.
Hyperintense signals on DWI were detected in 40% (95% CI, 26 to 55) of the patients with CVT (Fig. 3). However, any signal of clinical interest on DWI was found in 79% (95% CI, 46 to 99) of the patients. The sensitivity of DWI in the diagnosis of CVT was 22% (95% CI, 11 to 34). However, the specificity of DWI for detecting CVT was 98% (95% CI, 95 to 100) (Fig. 4).
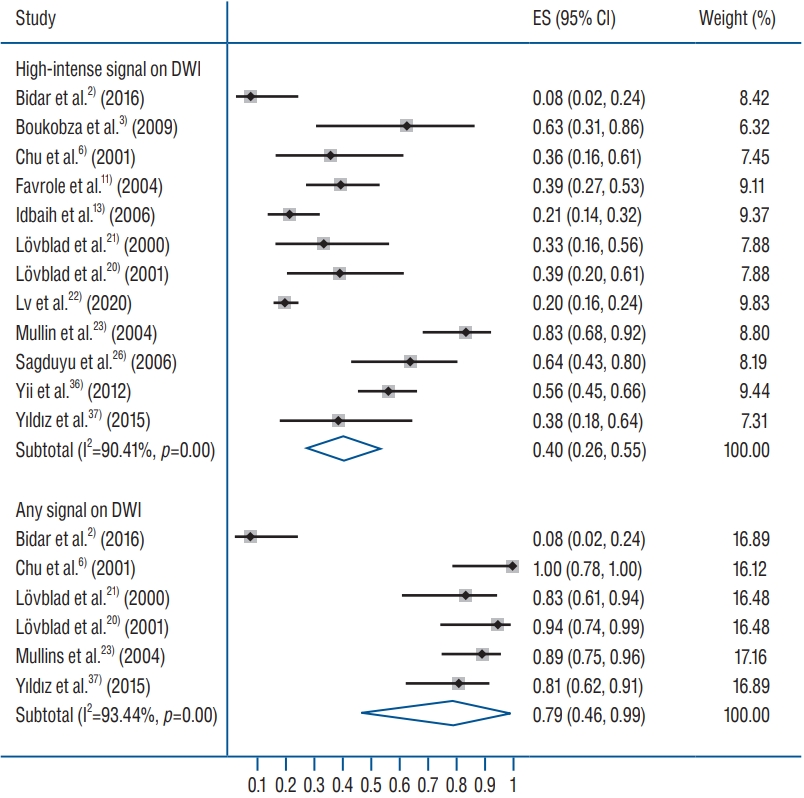
A forest plot showing the overall effect size of percent rate of hyperintense signal on DWI in cerebral venous thrombosis cases. In study identities, in case of Linn et al.[18]fi, first values are for cortical vein, and second for superior sagittal sinus. In case of Sadigh et al.[25], fifirst and second values denote investigator 1 and 2. ES : effect size, CI : confidence interval, DWI : diffusion-weighted imaging.
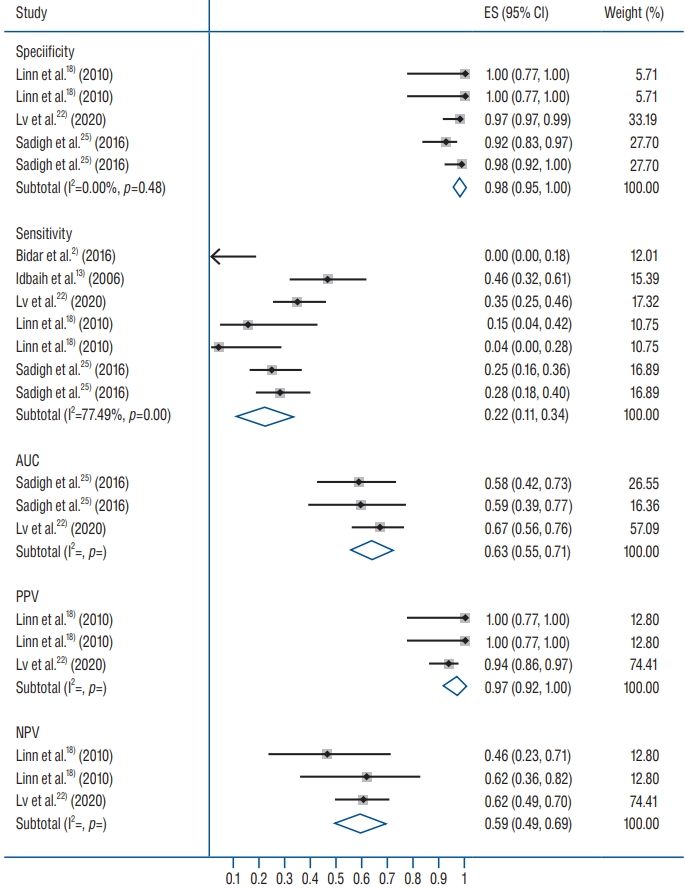
A forest plot showing the pooled sensitivity and specificity values in diagnosing cerebral venous thrombosis by diffusion-weighted imaging. ES : effect size, CI : confidence interval, AUC : area under curve, PPV : positive predictive value, NPV : negative predictive value.
ADC findings of the including studies were much heterogeneous. The range of ADC (×10-3 mm2/s) values in the DWI signal areas noted by the individual studies were 0.25–1.2 [23], 0.32–0.86 [6], 0.33–1.74 [10], 0.49±0.15 (standard deviation) [11], 0.65–0.79 [20], and 0.81–1.3 [8]. In general, the ADC values were lower in DWI signal areas than in surrounding non-CVT areas (mean difference−0.33×10-3 mm2/s [95% CI, −0.44 to −0.23]; p<0.00001; Fig. 5).

A forest plot showing the mean difference between ADC values in thrombosed areas and surrounding areas of patients with cerebral venous thrombosis. DWI : diffusion-weighted imaging, ADC : apparent diffusion coefficient, SD : standard deviation, CI : confidence interval.
DISCUSSION
In a sample population of patients with CVT who underwent DWI studies, we have found that the proportion of patients with CVT in whom hyperintense signals were detected on DWI was approximately 40%. Only a few studies reported the AUROC data, based on which the sensitivity of DWI in detecting a CVT was only 22% whereas the specificity was 98% [2,13,18,22,25]. There was a wider range of ADC values for DWI signal areas but generally it was lower in thrombosed areas than in surrounding tissues.
Currently, the MRI is routinely used in patients suspected for the presence of CVT by using different MRI sequences. Although, we have observed that hyperintense signal on DWI is associated with low sensitivity to detect CVT, however, the hyperintense signal on DWI had high specificity for CVT. It is suggested that DWI can provide an additional clue for the diagnosis of CVT which could be important in clinically unsuspected patients [37]. By using DWI, Favrole et al. [11] detected 20 occluded veins or sinuses in 12 patients (41%) with recent CVT and suggested that the presence of hyperintense signal on DWI in occluded veins at the time of diagnosis might be predictive of a low rate of vessel recanalization 2 or 3 months later. They also suggested that the movements of water molecules are restricted within the venous clot according to the stage of CVT formation [11]. Using diffusion-tensor imaging for 77 CVTs in 33 children, Wagner et al. [31] found restricted diffusion patterns in 38% of thromboses.
We have found that the proportion of patients with CVT for whom DWI hyperintense signals were detected was approximately 40%. The range was from 8% to 83% in the individual studies which contributed to a high statistical heterogeneity in this pooled analysis. Signal intensity on DWI mainly depends on restricted rates of diffusion. Compared with the normal white matter, stable but reduced diffusion has been observed in hyperacute, acute, and early subacute hematomas containing hemoglobin within intact red blood cells [1,14,28]. A thrombus in the vein can be differentiated from an intracerebral hematoma by the absence of extracellular f luid due to which thrombus exhibits highly restricted diffusion that can result in more intense signal on DWI [22].
The MRI intensity of venous thrombus varies according to time of imaging from the onset of thrombus formation. This may also affect the results of DWI to show high signal intensity with low ADC due to restricted diffusion. Especially if symptoms are subtle and the progression of thrombus is not uniform, the onset of thrombus formation cannot be detected accurately always which may lead to a low sensitivity of this method. Diagnosis of a thrombus in the cerebral veins can also be influenced by the paramagnetic effect of deoxyhemoglobin in blood [16]. The latest AHA/ASA scientific statement recommends that gradient echo T2 susceptibility-weighted imaging with MRI should be used to improve the accuracy of CVT diagnosis [27].
Use of DWI can be more valuable in discriminating the types of edema, in the assessment of tissue viability, in the detection of subclinical abnormalities, and in facilitation of basic imaging research related to the pathophysiology of CVT [6]. It has also been suggested that DWI may provide an additional clue to CVT diagnosis in clinically unsuspected patients after standard MRI scans but without sensitive MRI sequences such as contrast enhanced MRV or T2-weighted gradient recalled echo. Careful examination of cortical surface on diffusion MRI for clot signal or clot susceptibility signal can give additional information when CVT is not suspected on routine T1 or T2 or fluid-attenuated inversion recovery sequence [37]. The presence of hyperintense signal on DWI has also been found to be predictive of clinical deterioration during hospital stay [31].
ADC values were quite heterogenous in DWI signal areas among the included studies and less data were available to study ADC patterns comparatively. Generally, the ADC values were lower in DWI signal areas in comparison with surrounding areas. Lower ADC values are usually associated with pathological conditions including cerebrovascular events [5,9,24]. Moreover, ADC values change with time. In atypical ischemic event in brain, the ADC start decreasing from first hour of event to reach minimal levels at 24 hours after the onset of event and then start rising to become higher than surrounding normal tissue after 3 days of onset [2]. In cerebral hemorrhage patients too, a correlation is found between the signal intensity ratio on DWI with that of T2WI, but there existed no correlation between signal intensity and ADC [28].
CONCLUSION
This meta-analytical review suggests that DWI has low diagnostic efficiency and thus has a high risk of missing many CVT cases but may have supporting and exploratory roles. Although, hyperintense signals can be found at sites of thrombosis on DWI in at least some patients with CVT, the DWI may be more useful in differentiating CVT from intravenous non-thrombotic tissue as well as subclinical abnormalities. However, more data will be required to precisely evaluate DWI performance for CVT detection in general or for a subgroup of patients.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
INFORMED CONSENT
This type of study does not require informed consent.
AUTHOR CONTRIBUTIONS
Conceptualization : CT
Data curation : FJ
Formal analysis : BL, FJ
Funding acquisition : JW
Methodology : JL
Project administration : SY
Visualization : XC
Writing - original draft : XL
Writing - review & editing : BL