The Surgical and Cognitive Outcomes of Focal Cortical Dysplasia
Article information
Abstract
Focal cortical dysplasia (FCD) is the major cause of intractable focal epilepsy in childhood leading to epilepsy surgery. The overall seizure freedom after surgery ranges between 50–75% at 2 years after surgery and the long-term seizure freedom remain relatively stable. Seizure outcome after surgery depends on a various factors such as pathologic etiologies, extent of lesion, and types of surgery. Therefore, seizure outcome after surgery for FCD should be analyzed carefully considering cohorts’ characteristics. Studies of pediatric epilepsy surgery emphasize the early surgical intervention for a better cognition. Early surgical intervention and cessation of seizure activity are important for children with intractable epilepsy. However, there are limited data on the cognitive outcome after surgery in pediatric FCD, requiring further investigation. This paper reviews the seizure and cognitive outcomes of epilepsy surgery for FCD in children. Several prognostic factors influencing seizure outcome after surgery will be discussed in detail.
INTRODUCTION
Focal cortical dysplasia (FCD) is a subgroup of malformations of cortical development characterized by abnormal cortical lamination, neuronal migration, and differentiation. It was first reported from pathological specimens obtained in ten patients with drug resistant epilepsy [50]. Over the past decade, several classifications of FCD have been proposed [2,39]. In 2011, the International League Against Epilepsy Task Force proposed a new consensus classification based on histopathological features to yield consistent interobserver and intraobserver reliability [5].
FCD has a high epileptogenic potential, and is often associated with drug-resistant epilepsy. It is the most common cause of intractable focal epilepsy in children undergoing epilepsy surgery [20,32]. The primary goal of epilepsy surgery for intractable epilepsy is to achieve seizure freedom and eliminate adverse consequences of continuing antiepileptic drug (AED) treatment. When children achieve seizure freedom after successful epilepsy surgery, withdrawal of AEDs is generally considered. After assessing the benefits of AED discontinuation and the risk of seizure recurrence after withdrawal, clinicians decide whether and when to stop the AEDs. For young children, additional objective is to optimize neuropsychological development and improve the quality of life after surgery [13].
In this article, we focused on the seizure and cognitive outcomes of epilepsy surgery in pediatric FCD series. Moreover, we reviewed the prognostic factors for favorable outcome after epilepsy surgery.
SEIZURE OUTCOME
Seizure outcomes after epilepsy surgery has been improved over time with the advancement of preoperative diagnostic methods and surgical techniques [47,54]. The overall seizure-free outcome after surgery ranges from 50 to 75% [7,9,12,29]. Details of the selected surgical series are shown in Table 1. Seizure outcomes after surgery are dependent on a number of factors including pathologic etiologies, extent of lesion, and types of surgery. Series that analyzed mostly short term follow-up after surgery presented better seizure outcome [35,52]. These surgical series are associated with a decrease in seizure-freedom with postoperative time [28,34]. Some studies reported that seizure outcome at least 2 years after surgery remained stable as long-term outcome [15,19,45]. Therefore, it can be considered that a 2-year postoperative outcome may reflect the long-term seizure outcome.
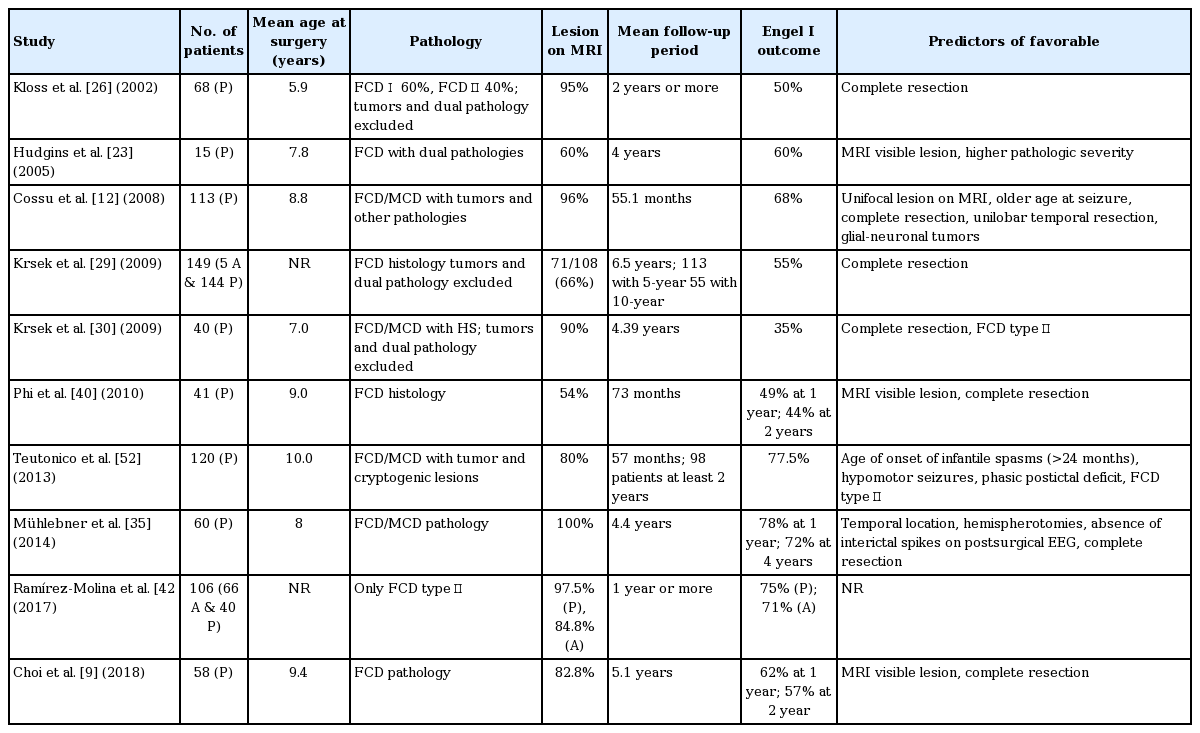
Cohort characteristics and outcomes after epilepsy surgery in children with focal cortical dysplasia/malformation of cortical development
Seizure outcomes of the two large pediatric surgical series are further discussed here. One of the largest pediatric series analyzed the outcome of 113 children who underwent surgery between 1996 and 2004 [12]. The mean age at surgery was 8.8 years. Pathologic etiologies include not only FCD, but also dual pathologies such as glio-neuronal tumors or mesial temporal sclerosis. The majority (96%) had abnormal brain magnetic resonance imaging (MRI). At 55 months after the mean postoperative follow-up, 68% were categorized as Engel’s class I, with 60% being seizure free (Engel’s classes Ia and Ic). They reported that focal lesion on MRI, older age at seizure onset, complete resection, unilobar temporal resection, and a glioneuronal tumor had better surgical outcome.
Another series studied the surgical outcome of 149 patients (144 patients were <20 years and five adult patients) with a mild malformation of cortical development (mMCD) or FCD [29]. Surgery was performed between 1986 and 2006. Of these 149 patients, 29 patients had mMCD, 58 patients were classified as FCD type I, and 52 patients as FCD types II. At 2 years follow-up, 55% were classified as Engel’s class I. With regard to long-term seizure outcome, 113 patients were followed-up for at least 5 years after surgery, and 75% of them remained stable seizure status after the second postoperative year. This study mainly included children with histologically proven mMCD/FCD, and demonstrated that complete resection is the most important predictive prognostic factor for surgical outcome.
PROGNOSTIC FACTORS OF FAVORABLE OUTCOME
Several prognostic factors related to surgical outcome have been proposed. It is crucial to select the best surgical candidates based on predictors of favorable surgical outcome. In a meta-analysis of FCD surgical series, complete resection, severe type of histopathology, detection of MRI lesion, and temporal location of the surgery were found to be important prognostic factors [8,44]. However, the heterogeneity of patient populations, types of surgery, and pathologic etiologies between studies may account for the inconsistency in the proposed prognostic factors across various studies.
Complete resection is widely accepted to be the most important prognostic factor for seizure freedom after surgery [9,10,12,15,18,19,25,26,29,35]. Complete resection is generally defined as complete removal of the lesion on neuroimaging or the interictal and ictal onset zones on intracranial electrode recording. Patients with complete resection achieved 60–70% chance of becoming seizure free, while those with incomplete resection only achieved 14–22% [9,26,29]. Complete resection of the visible lesions (lesional zone) and the epileptogenic zone would increase the likelihood of successful surgical outcomes. It is difficult to assert that resection of the visible lesion is sufficiently includes the epileptogenic zone. Indeed, the epileptogenic zone may be organized as the focal lesional site or as a more complex network extending beyond the lesion [36,46]. To delineate epileptogenic zone, patients with normal MRI or poorly localizing electroencephalography undergo intracranial electrode monitoring, electrocorticography, or stereo-electroencephalography. In addition, a resection of the seizure onset zone, which were determined by high-frequency oscillations or lowvoltage fast activities, resulted in a favorable seizure outcome in pediatric FCD [1,17,31]. The leading cause of incomplete resection was the overlap between the epileptogenic zone and the eloquent cortex [18,21,30,33]. When the epileptogenic zone overlaps with eloquent cortex, multiple subpial transections (MST) can be considered; however, the efficacy of MST in epilepsy surgery has not yet been fully elucidated [3].
Both pediatric and adults surgical series demonstrated that severe dysplasia usually yields a more favorable outcomes compared with mild cortical dysplasia [23,25,27,49,52,55]. In a series of 40 pediatric FCD (24 FCD type I and 16 FCD type II), seizure freedom was achieved in 75% of FCD type II patients, whereas only 21% of FCD type I patients [30]. Conversely, some studies failed to identify any significant differences between the seizure outcome and severity of histopathology [15,35,57]. Compared with FCD, glio-neuronal tumors are known to have greater favorable outcomes [12,14,37,52]. Furthermore, glioneuronal tumors associated with FCDs (FCD IIIa) showed excellent outcome compared with FCD type I, which was comparable to solitary tumors [11].
Cohort studies evaluating predictors of surgical outcome reported better outcomes in patients with demonstrated MRI lesions than in those without relevant MRI abnormalities [9,12,23,40]. A meta-analysis in various surgical groups of patients showed that patients with lesions on MRI had a 2.5 times higher chance of seizure freedom after surgery (odds ratio, 2.5; 95% confidence interval, 2.1–3.0; p<0.001) [51]. The same observation has been reported in patients with FCD [44]. Constellation of MRI findings is diagnostic for FCD in patients with intractable epilepsy. However, MRI findings can often be subtle and difficult to detect, especially for patients with FCD type I. In a previous study, about 20% of patients with FCD had normal MRI scans [32]. A structural lesion on MRI is likely to be co-located with the epileptogenic cortex. Furthermore, a discrete lesion on MRI may provide substantial information to localize the epileptogenic zone and serve as a marker of the resection area allowing a more effective resection. However, even in the absence of MRI lesion, it may be worthwhile to consider epilepsy surgery in patients with intractable focal epilepsy. Multimodal integrative presurgical evaluation may lead to a good outcome in patients with intractable focal epilepsy, even without demonstrable lesion on MRI [24].
In both pediatric and adult FCD series, the seizure outcome of temporal lobe resection was better than that of extratemporal resection [8,12,22,35,44]. Better localization of the epileptogenic zone and chances of combined dual pathology, such as hippocampal sclerosis, might contribute to improve seizure outcome in temporal lobe resection. Moreover, in temporal lobe resection, there is no need to consider sparing the eloquent areas.
The need for intracranial monitoring was associated with poor outcome [6]. Generally intracranial monitoring is performed when there is uncertainty in the location and extent of the epileptogenic zone. Therefore, poor localization of the epileptogenic zone could be a reason for intracranial monitoring which ultimately results in poor surgical outcome.
COGNITIVE OUTCOME
Children with FCD frequently have combined developmental and cognitive dysfunction [30,32,49,55]. Another important aim of epilepsy surgery in children is to improve the overall cognitive outcome. In a study of infants treated surgically for catastrophic epilepsy, Wyllie observed a marked catch-up development in those with at least 50% reduction in seizures [56]. In a series of 42 children who underwent temporal resection for intractable epilepsy caused by hippocampal sclerosis or dysembryoplastic neuroepithelial tumors, a statistically significant improvement of the full scale intelligence quotients was observed [48]. However, the improvement of cognitive function is not guaranteed after surgery in all patients. A study evaluating the cognitive outcome after epilepsy surgery in preschool children showed that only a few patients gained cognitive improvement after surgery [16]. They reported that patients who achieved seizure-free, shorter duration of epilepsy, and a low preoperative developmental level showed cognitive improvement following surgery. However, to the best of our knowledge, studies evaluating the cognitive outcome after epilepsy surgery for FCD are limited (Table 2). A study of 40 children with FCD type II reported that 37.5% of children showed an improvement after surgery [42]. However, in other pediatric series, a stabilization of cognitive function, rather than a marked improvement, after successful surgery was demonstrated [41,43]. Therefore, cognitive improvement is not guaranteed in all patients after effective epilepsy surgery. Nonetheless, cognitive improvement, at least stabilized cognitive function, is possible after surgery.

Cognitive outcome after epilepsy surgery in children with focal cortical dysplasia/malformation of cortical development
The fact that early onset and long duration of epilepsy may be followed by cognitive deterioration suggests a window of vulnerability for irreversible decline of cognition [4,38,53]. Some pediatric FCD series demonstrated the better cognitive outcomes after surgery in patients with shorter epilepsy duration [7,41]. In contrast, other study opposed that epilepsy duration did not appear to inf luence cognitive outcome after surgery [42]. Nevertheless, to minimize the detrimental effects of uncontrolled seizure, early surgical intervention and cessation of seizure activity are important for children with intractable epilepsy.
CONCLUSION
Focal cortical dysplasia is a major cause of focal intractable epilepsy and epilepsy surgery in childhood. The efficacy of epilepsy surgery is dependent on the ability to precisely localize and resect the epileptogenic zone. Among the several prognostic factors, complete resection of the epileptogenic zone is the most powerful predictor for favorable seizure outcome. We observed cognitive improvement or stabilization after surgery in children with FCD. However, more studies to support early surgical intervention for a better cognitive outcome will be required.
Notes
No potential conflict of interest relevant to this article was reported.
INFORMED CONSENT
This type of study does not require informed consent.