Mysterious Foreign Body in Transverse Sinus
Article information
Abstract
This case report describes a patient who had a foreign body in transverse sinus. A 35-year-old Korean-Chinese man visited the emergency room with lacerated wound in left eyelid and a foreign body which was stumbled upon in the skull. On examination, there was right side hemianopsia in his left eye. He did not complain any headache or show any abnormal neurological signs, but there was a foreign body at left transverse sinus in computed tomography which was taken at another hospital. There was no intracranial abnormality except the foreign body in computed tomography. Because of the financial problem, additional evaluations were not possible. We herein report a strange case in which the pathway of a foreign body to locate in transverse sinus was ambiguous, and suggest that the foreign body located in transverse sinus might have been the penetrated along the anterior fontanelle and passed through the superior sagittal sinus.
INTRODUCTION
Undesired accidents may frequently occur, and many unusual cases have been reported. Among these, a foreign body is relatively common source. A foreign body can be located anywhere in body, for example, appendix, bronchus, ear, eye, nose, oral, sinus, skin, skull base, throat, rectum, urethral, and others1,3,5,6,9,12,14,15,18). Most of the foreign bodies can be traced their origins and the pathways. Here, we report a mysterious foreign body with its origin and pathway ambiguous.
CASE REPORT
A 35-year-old Korean-Chinese man visited the emergency room because of the accident during a construction work. He had a small lacerated wound in left eyelid which was superficial and not severe. His right eye was artificial because of motorcycle accident which was happen in China when he was child. He said that the artificial eye was replaced in China after the accident, because of the visual activity loss and the warning of a folk remedy about progression of visual loss in both eyes. We checked visual acuity of left eye and found right side hemianopsia. He did not complain any headache or neurologically abnormal sign, but a foreign body was seen in the computed tomography of the brain which was taken at another hospital. There was a bullet-like foreign body, about 1.9 cm in length and 0.8 cm in diameter with medial projection of the apex, in the left transverse sinus. The left transverse sinus was not engorged and not injured by the foreign body. Except the foreign body, there were no definite intracranial abnormalities such as hemorrhage, skull fracture, brain parenchymal disease, and even more healed skull fracture line. The skull radiographs and computed tomography were shown in Fig. 1. After revealing the presence of the foreign body, we carefully reexamined to find the insertional wound of such foreign body. But there was no scar in whole scalp and neck.
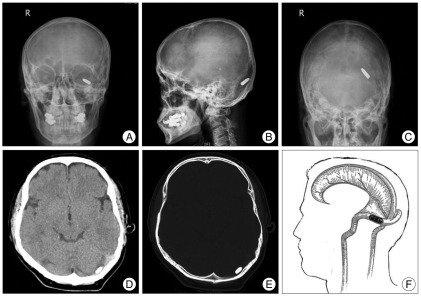
The skull radiographs and computed tomography of the patient with a foreign body in left transverse sinus. A, B and C : The skull radiographs with a foreign body located in left transverse sinus area. D and E : The computed tomography with a foreign body which is not associated with the brain parenchymal injury or the skull fracture. F : The schematic figure of the sinuses and the foreign body.
We recommended additional evaluations to be done, but he refused because of poor economic status. He was discharged after wound care.
DISCUSSION
Our patient has lost his visual acuity due to the motorcycle accident when he was young. He had been living without the insight of right side hemianopsia, and the foreign body in skull might have been found by chance. But, there was no evidence of route which the foreign body could penetrate into the skull.
Because right artificial eye was replaced after the accident, the authors have guessed that the foreign body came from the motorcycle accident. The foreign body was located in left transverse sinus near the primary visual cortex. The left homonymous hemianopia is a visual field defect caused by lesions of the retrochiasmal visual pathways, such as primary visual cortex10,13). Although it is mere guesswork, the folk remedy who replaced artificial eye perhaps misconcepted that the visual loss occurred because of the eyeball problem, not the visual pathways problem.
The possible pathways that the foreign body could penetrate into the skull were simply classable by direct or indirect invasion into the skull, but, direct invasion was less possible because of the absence of the skull fracture, although it might have been healed. Therefore, the possibility of indirect invasion seems more plausible explanation. However, the possible route of indirect invasion should be satisfied the following criteria; invisible or easily healable small skin wound, no accompanying with a cranial fracture, and proper size which the foreign body could be migrated. The answer could be the fontanelles and the superior sagittal sinus.
Fontanelles are soft spots on a baby's head which enable the bony plates of the skull to flex, allowing the child's head to pass through the birth canal. There are the anterior and posterior fontanelles. The small posterior fontanelle usually closes during the first several months of an infant's life. The much larger, diamond-shaped anterior fontanelle generally closes completely until two year-old2,11). Often it is late in closing or may never close in cleidocranial dysostosis, a hereditary congenital disorder due to the haploinsufficiency7). Unusually persistence of an open anterior fontanel has been reported also in a 4-year-old girl without neurological impairment17). So there is a possibility of the penetration of foreign body through the anterior fontanelle which was not closured at childhood period, and the penetrating wound may have been healed with intramembranous ossification, which the mesenchymal connective tissue turned into bone tissue.
The superior sagittal sinus is a dural venous sinus in the sagittal groove, beginning at the foramen caecum and terminating at the confluence of sinuses where it merges with the straight sinus and corresponding transverse sinus8,16). It is triangular in section, narrow in front, and gradually increases in size as it passes backward. Its inner surface presents the openings of the superior cerebral veins, and their orifices being concealed by fibrous folds, numerous fibrous bands, extend transversely across the inferior angle of the sinus. At birth, the superior sagittal sinus is nearly matured and increased in size with aging16). It is composed with soft fibrous tissues, so the foreign body, even though it was large one, could pass through the lumen.
Nevertheless, the report of blood flow and velocity in the superior sagittal sinus disappointed our expectation4). The results showed that mean flow in the superior sagittal sinus was 443±124 mL/min and mean velocity 152±30 mm/second in healthy adult, and the values were markedly decreased in the situation of flow obstruction. These values would be lower in children age, and it would not be helpful condition to push the foreign body from the superior sagittal sinus to transverse sinus. But, we thought the proper passage to transverse sinus was only superior sagittal sinus because the foreign body was lied along the transverse sinus tract, and could not move against to the gravity, although the passive force for moving of foreign body was not clear.
CONCLUSION
We suggest the hypothesis that the foreign body located in transverse sinus in this patient may have had its penetration along the anterior fontanelle and passing through the superior sagittal sinus.