INTRODUCTION
Reopening occluded vessels through endovascular thrombectomy (EVT) has improved clinical outcomes in acute ischemic stroke (AIS) by facilitating reperfusion and salvaging brain tissue at risk. The history of EVT for AIS can be described as a history of conquest and pioneers. It began with the initial exploration of intravenous thrombolysis (IVT) territory for patients with AIS caused by anterior large vessel occlusion (LVO). The subsequent territorial expansion began with widening the time window for treatment and has since continued to progress. However, despite these advancements, a vast and largely uncharted domain remains waiting to be reclaimed by further advancements in EVT.
HISTORY
IVT has been the primary treatment for AIS patients presenting within 3-4.5 hours of symptom onset since the NINDS (National Institute of Neurological Disorders and Stroke) trial in 1995 and the ECASS III (European Cooperative Acute Stroke Study) trial in 2008 [32,70]. However, low recanalization rates were prominent with IVT, particularly in cases of LVO, when compared to AIS without LVO [11,60].
Seven pivotal randomized controlled trials (RCTs) published between 2015 and 2016 confirmed that EVT is considered a standard treatment for patients with LVO in the anterior circulation when performed within 6 hours of symptom onset [10,14,15,27,36,63,90]. The time interval since symptom onset was identified as the most crucial factor for determining the optimal management of stroke patients. The HERMES (Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke) study, a meta-analysis of five RCTs, similarly concluded that performing EVT after 7.3 hours did not confer any additional clinical benefit [91]. In the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) study, every hour of delay in reperfusion resulted in a 7.7% decreased probability of achieving functional independence [67]. Likewise, in the REVASCAT (Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting Within Eight Hours of Symptom Onset) study, every 30-minute delay in reperfusion resulted in a 26% decrease in the likelihood of a favorable outcome [79]. Consequently, streamlining workflow to reduce time delays has become the cornerstone of stroke systems for both intravenous and intraarterial therapies.
The concept of penumbra, consisting of cells incapacitated due to lack of oxygen, has led to efforts to identify ischemic penumbra. In 2011, a multicenter study of 237 patients with anterior circulation LVO, treated beyond 8 hours of symptom onset based on perfusion imaging, showed good outcomes with comparable complication rates to those observed in early time window studies [38]. The DEFUSE (Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution) 2 study in 2012 demonstrated comparable good outcomes after EVT in patients presenting within and beyond 6 hours when a target mismatch was noticed on perfusion imaging [48]. Efforts to identify patients with salvageable brain tissue even in the late time window beyond 6 hours led to the design of the DAWN (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) and DEFUSE 3 trials, which resulted in a paradigm shift from “time is brain” to “imaging is brain” [76]. The DAWN trial selected patients presenting between 6 and 24 hours based on severe clinical deficits (high National Institutes of Health stroke scale [NIHSS]) with a small established infarction (small core). This clinical-core mismatch successfully identified patients who would benefit from EVT in the late time window, and the trial was halted after a pre-specified interim analysis. The rate of functional independence at 90 days was 49% in the EVT group compared to 13% in the control group [72]. The DEFUSE 3 trial enrolled patients in the late time window (6-16 hours) with evidence of salvageable tissue on perfusion imaging. Following the presentation of the DAWN trial results in May 2017, the DEFUSE 3 trial was stopped due to lack of equipoise, and an early interim analysis confirmed the benefit of EVT over medical therapy in patients selected based on a tissue paradigm. Good outcomes in the treatment arm were 45%, compared to 17% in the medical arm [3].
CURRENT ISSUES OF EVT
Current advancements have been made in two key area : first, determining the expandability of EVT to benefit a larger number of eligible AIS, and second, improving the execution of EVT techniques for better clinical outcome.
Expanding eligibility for endovascular therapy
A significant number of patients are not receiving the potential benefits of this highly effective treatment, as less than 20% of patients with AIS currently undergo EVT. However, with the expansion of treatment eligibility criteria, this percentage could potentially increase to 43.1% [31]. The current guidelines, which are based on high-evidence level studies, employ restrictive eligibility criteria to optimize the chances of demonstrating the efficacy of EVT. Meanwhile, these criteria also exclude a substantial proportion of potentially eligible patients, thereby limiting the broader application of endovascular treatment. Although there are ongoing RCTs aimed at expanding the eligibility criteria for EVT, it remains challenging to address various aspects of eligibility in clinical trials due to financial issues, challenges in patient enrollment, and the difficulty of verifying statistical differences. However, there has been a growing number of observational studies supporting the off-label application of EVT, which further emphasizes the need to consider a broader population for this treatment.
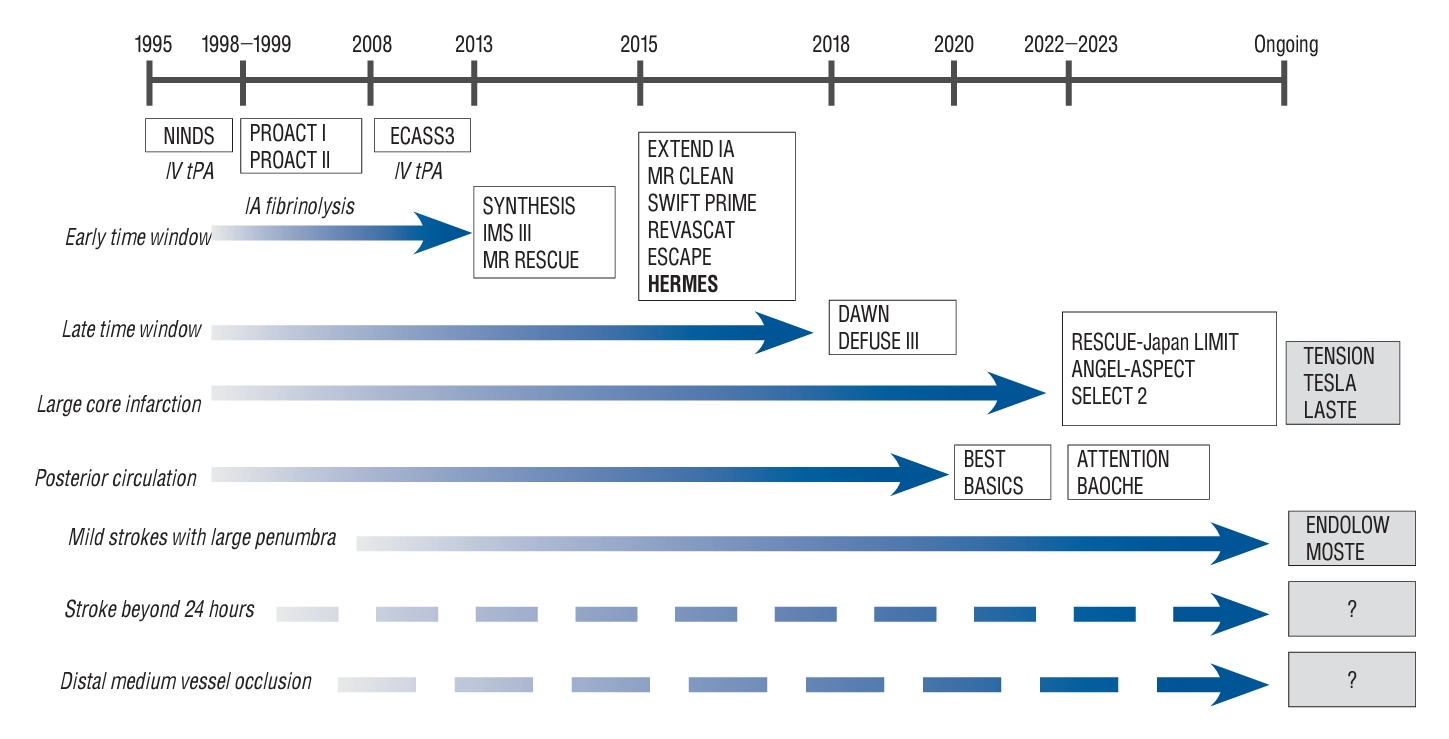
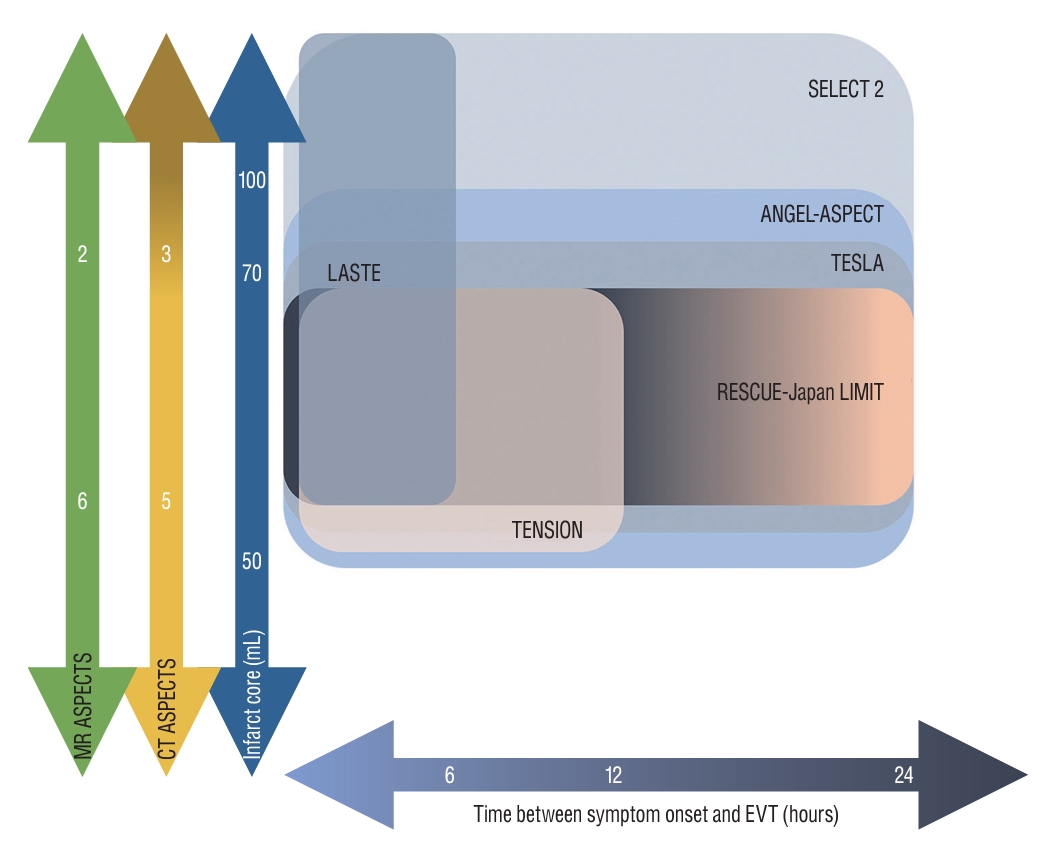
Fig. 1 shows the timetable of RCTs regarding expanding the eligibility of EVT in AIS patients. Based on the number needed to treat (NNT) for achieving 90-day functional independence in severe RCTs, the population with expanded indications also demonstrated a meaningful response to EVT. Narrowing patient selection with precise criteria tends to improve treatment effectiveness (Fig. 2).
EVT for large core infarction (LCI)
LCI is a common exclusion criterion in 21% of ineligible LVO patients [23]. Majority of early time window trials set a threshold for LCI, typically defined as an infarct volume of 50-70 mL or an Alberta Stroke Program Early CT Score (ASPECTS) of 6 [14,83,106]. The in-hospital metric for triaging patients with AIS is designed to exclude patients with a LCI, as they are considered at a higher risk of complications, including reperfusion injury following recanalization and an increased incidence of post-thrombectomy symptomatic intracerebral hemorrhage (sICH).
Recent studies have suggested that an ASPECTS below 2 may result in futility, indicating limited potential benefit from EVT [33,110]. Additionally, other studies have demonstrated a lack of benefit when the computed tomography perfusion (CTP)-determined core volume exceeds 100-150 mL [16,85]. Meanwhile, multiple studies have suggested that performing EVT on a relatively large core profile, even in patients with baseline ASPECTS scores of 3-5 which were previously considered indicative of treatment futility, can offer meaningful treatment benefits and reduce disability and mortality [24,81,105].
There are issues regarding the precise measurement of the extent of ischemic change, particularly due to the absence of an available gold standard for ischemic core imaging. Predicting the core infarct using computed tomography (CT) or magnetic resonance imaging (MRI) is not completely correlated with tissue death [56]. Different cells, including neurons, are destined to be affected by ischemia in varying ways. The analysis of pooled individual patient data from the HERMES collaboration found that patients who underwent reperfusion had significantly better functional outcomes compared to those who did not undergo reperfusion, even when controlling for follow-up infarct volume [12]. Moreover, seemingly irreversible changes in MRI diffusion-weighted imaging (DWI) and non-contrast CT can potentially reverse after the restoration of blood flow [45].
As the time window increases, there is a noticeable decrease in the mismatch ratio, which correlates with a reduced benefit from EVT [95]. However, patients with a LCI who present in the early time window, often referred to as fast progressors, may still experience benefits from EVT through reperfusion of the salvageable mismatch area [24,105]. Nonetheless, identifying the progressively decreasing mismatch profile in the early time window is challenging due to the limited time window and the poor predictive value of perfusion imaging in hyperacute window [16].
Recently, starting from 2022, three RCTs including RESCUE-Japan LIMIT (Recovery by Endovascular Salvage for Cerebral Ultra-acute Embolism-Japan Large Ischemic Core trial), ANGEL-ASPECT (Endovascular therapy in acute anterior circulation large vessel occlusive patients with a large infarct core), and SELECT 2 (Randomized Controlled Trial to Optimize Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke), have been published sequentially [35,84,100]. These trials have shown the potential for expanding the inclusion criteria for EVT to include patients with LCI (Fig. 3). The first published RESCUE-Japan LIMIT study randomly assigned 203 patients with LCI, meeting the inclusion criteria of CT or DWI ASPECTS of 3-5 within 6 hours after the last known well or within 24 hours in the absence of early changes on fluid-attenuated inversion recovery (FLAIR) images. The study demonstrated improved functional outcomes, with a lower modified Rankin scale (mRS) score of 0 to 3 at 90 days in the EVT group compared to the medical care group (31.0% vs. 12.7%, relative risk 2.43; 95% confidence interval [CI], 1.35 to 4.37; p=0.002) [100]. The ANGEL-ASPECT study, conducted in China, randomly assigned 456 patients with LCI who met the inclusion criteria of ASPECTS of 3-5 or infarct core volume of 70-100 mL within 24 hours after the last known well. The study demonstrated a shift in the distribution of functional outcome at 90 days, with a generalized odds ratio of 1.37 (95% CI, 1.11 to 1.69; p=0.004), indicating a favorable treatment effect in the EVT group. However, it is important to note that the EVT group had a higher incidence of intracranial hemorrhage, with 6.1% experiencing sICH compared to 2.7% in the control group, and 49.1% experiencing any intracranial hemorrhage compared to 17.3% in the control group [35]. The SELECT 2 study randomly assigned 352 patients with similar inclusion criteria as the ANGEL-ASPECT study, except it included an infarct core volume of 50-70 mL. It demonstrated a better functional outcome with a generalized odds ratio of 1.51 (95% CI, 1.20 to 1.89; p<0.001). Interestingly, cerebral hemorrhage was infrequent in both groups [84].
Still ongoing RCTs, including the TENSION (Efficacy and Safety of Thrombectomy in Stroke With Extended Lesion and Extended Time Window; NCT03094715), TESLA (Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke; NCT03805308), and LASTE (Large Stroke Therapy Evaluation; NCT03811769) trials, have varying inclusion criteria based on different definitions of large core volume infarct, imaging modalities, time windows, and the use of perfusion imaging (Fig. 3). As the results of RCTs on LCI continue to emerge, it will be possible that we may witness not only an expansion of eligibility criteria for patients with LCI but also a fundamental change in the metrics used for patient selection.
EVT for strokes beyond 24 hours
Recent studies have primarily focused on a time window limited to 24 hours, and conducting prospective studies for AIS beyond 24 hours, including RCTs, poses challenges due to the small fraction of the AIS population. Patients with good collateral circulation may still exhibit a viable ischemic penumbra even in the later stages of stroke [19,87]. Among these slow progressors, some fortunate individuals never experience further infarction progression, while the majority of non-reperfused patients typically encounter infarct progression within 3 days [47,102].
About 20% of patients with LVO who present beyond 24 hours show persistent mismatch profile [22]. It appears that patients presenting beyond 24 hours, who otherwise meet DAWN or DEFUSE 3 criteria, may be safely treated with comparable clinical outcomes to those treated within 24 hours [1,17,19,22]. In the propensity score-matched analyses using retrospective data of 150 patients with anterior circulation LVO with moderate to severe neurologic deficits persisting beyond 16 hours, about one-third of LVO patients met the inclusion criteria of either DAWN, DEFUSE 3, or ESCAPE (Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke) trials with identified salvageable tissues. EVT was performed in 16% of patients and showed better odds of good functional outcomes with 11.08-fold higher odds ratio [41]. In the SELECT LATE study, retrospective observational cohort study, 81% of patients who underwent EVT beyond 24 hours demonstrated the presence of a mismatch. These patients were more likely to achieve functional independence and had lower mortality rates. However, it should be noted that as time progressed, there was an increased tendency for hemorrhage to occur [86].
EVT for mild strokes with large penumbra
Clinical trials typically exclude patients with mild clinical stroke severity, defined as NIHSS scores ≤5, who are considered “too good to treat”. A population-based study of AIS indicates that approximately 7% of patients with LVO were not treated due to their mild symptoms [31]. Interestingly, some reports have found that 27-35% of AIS patients with low NIHSS scores still experience poor clinical outcomes despite receiving optimal medical management [9,25,39,96]. Moreover, conservative management in 14.6% to 34.6% of patients with mild disability and LVO AIS can lead to frequent early neurologic deterioration (END) [42,51,78,82]. In such cases, anticipative thrombectomy has been associated with improved clinical outcomes, while patients who undergo rescue thrombectomy after experiencing END have shown worse outcomes compared to those who receive either optimal medical management alone or immediate EVT alone (54.5% rescue EVT, 71.7% optimal medical management alone, 85% immediate EVT; p=0.007) [69]. However, another study argues that the potential risk associated with neurologic deterioration or hemorrhagic event after EVT might outweigh the risk of END after optimal medical management [101].
Not all patients with low NIHSS scores are equivalent in terms of clinical outcomes, highlighting the limitations of using NIHSS as a screening tool for treatment eligibility. The heterogeneity of clinical outcomes emphasizes the need for better methods of patient selection. While guidelines emphasize the importance of disabling symptoms in patient selection for IVT, there is currently no evidence supporting the differentiation of patients with low NIHSS scores based on the presence or absence of disabling symptoms [40,93]. More proximal LVO and longer thrombus length are known predictive factors of END [65,94], while hypoperfusion severity, such as the volume of Tmax >10 seconds or the hypoperfusion intensity ratio (HIR), is another candidate for predicting END [21,30]. The upcoming RCTs, ENDOLOW (Endovascular therapy for low NIHSS ischemic stroke; NCT04167527) and MOSTE (Minor Stroke Therapy Evaluation; NCT03796468), are expected to shed light on the benefits of EVT compared to medical management.
EVT for distal and medium vessel occlusion (DMVO)
DMVOs constitute 25-40% of AIS [89]. With advances in catheter technology, the development of smaller thrombectomy devices, and increasing expertise in neuroendovascular procedures, DMVOs have been identified as a potential frontier in the EVT of AIS. However, there are disagreements regarding the use of EVT for DMVO, primarily due to concerns about the procedural safety of performing EVT in small-calibered vessels. Additionally, it has been observed that more distal occlusions tend to exhibit a better response to IVT. Nevertheless, IVT fails to achieve successful recanalization in 50% of DMVOs [11,77]. Moreover, dealing with secondary DMVOs after primary intra-arterial or intravenous procedures is becoming a matter of concern as EVT becomes more widespread. It is worth noting that currently, no further RCTs have reported on expanding the indications for DMVOs.
Efforts to expand the indications of EVT for more distal vessel occlusions began with M2 occlusion [88]. Distinguishing M2 occlusion from M1 occlusion can be challenging due to anatomical variations. However, an analysis of patients with M2 segment occlusion from the HERMES collaboration demonstrated that EVT resulted in improved functional outcomes for individuals with M2 segment occlusion [61]. Importantly, this improvement was achieved without an increased risk of complications related to the treatment. The 2019 guidelines from the Society for Neuro-interventional Surgery have issued a class I, level A recommendation for thrombectomy in the middle cerebral artery-M2 location [64].
For more distal occlusions, the TOPMOST (Treatment for primary distal, medium vessel occlusion stroke) study, a case-control study involving 184 patients with distal occlusion of the posterior cerebral artery (PCA), demonstrated the clinical benefit, feasibility, and safety of the endovascular technique for treating such occlusions [62]. However, apart from this clinical trial of EVT for PCA occlusion, the issue regarding occlusions in locations even more distal than the M2 segment remains unclear.
The current EVT technique for LVO is mainly focused on how to effectively access tortuous distal vessels and reduce thrombus fragmentation. However, the fragility of distal and medium intracranial vessels, characterized by smaller caliber and thinner arterial walls compared to proximal large vessels, hesitates the application of the same techniques used for EVT in LVO due to hemorrhagic complications and thrombectomy-related vessel injury. A combined strategy, mediated by blind exchange mini-pinning (BEMP), utilizing a low-profile mini aspiration catheter and a micro-stent retriever for thrombectomy in small-calibered vessels, has been proposed to achieve a higher rate of recanalization while reducing the incidence of hemorrhagic events and vessel injury [34]. However, given that symptoms in patients with DMVOs tend to be mild, careful patient selection should be ensured.
EVT for posterior circulation strokes
Posterior circulation LVO comprises 5% of all LVOs [23]. With devastating nature of posterior circulation strokes, the rate of mortality or severe morbidity was reported up to 90% [53]. According to prospective registries of EVT for acute basilar artery occlusion (BAO), although the successful reperfusion rate after EVT is comparable to that of anterior circulation LVO, only about 27.4% of patients experience favorable outcomes, indicating a high rate of futile recanalization [104].
Until 2022, the endeavor to establish the superiority of EVT over medical treatment in acute BAO faced a setback with the neutral results from two RCTs. These trials enrolled patients with BAO who presented within the 6-hour window in the BASICS (Basilar Artery International Cooperation Study) trial and within the 8-hour window in the BEST (Basilar Artery Occlusion Endovascular Intervention Versus Standard Medical Treatment) trial. Experts have pointed out that the study design of both RCTs has pitfalls, including high rates of crossovers in the BEST trial and a lack of consecutive enrollment in BASICS [46,54]. According to subgroup analysis of the BASICS trial and previous observational studies, which indicated that patients with minor deficits (NIHSS <10) [46,92] and extensive baseline infarction or large pontine infarct do not derive significant benefits from EVT compared to medical therapy [4,59,107], the eligibility criteria of other ongoing RCTs, the ATTENTION (Endovascular Treatment for Acute Basilar Artery Occlusion trial) and BAOCHE (Basilar Artery Occlusion Chinese Endovascular) trial, have undergone refinement, resulting in narrower criteria.
The ATTENTION trial randomized 340 patients with BAO who presented within 12 hours of the estimated time (i.e., onset of severe symptoms or coma) of BAO, had moderate to severe symptoms defined by an NIHSS score of ≥10, and a posterior circulation ASPECTS (pc-ASPECTS) of ≥6 (or ≥8 in patients ≥80 years) [98]. On the other hand, the BAOCHE trial recruited 217 patients with BAO who presented from 6 to 24 hours since symptom onset. Although the BAOCHE trial included patients with an pc-ASPECTS score ≥6 and ponsmidbrain index of ≤2, the majority of patients included had an NIHSS score higher than 10 [37]. Given the anticipated dismal prognosis of BAO, the primary outcome in both trials was defined as achieving a mRS of 0-3. In both trials, EVT demonstrated improved functional outcomes compared with medical therapy. The ATTENTION trial showed higher rates of favorable functional outcomes, with an mRS score of 0-3 at 90 days in the EVT group compared to the medical management group (46% vs. 23%; relative risk, 2.06; 95% CI, 1.46 to 2.91; p<0.001) [98]. Similarly, in the BAOCHE trial, which included patients in the late time window without advanced imaging assessment, similar functional outcomes were noted for EVT (46% vs. 24%; relative risk, 1.81; 95% CI, 1.26 to 2.60; p<0.001) [37]. Notably, the rates of symptomatic hemorrhage in both trials were comparable to the reports of anterior circulation LVO [37,98]. Therefore, EVT appears to be beneficial in patients with BAO who present with moderate to severe symptoms.
Assessing the perfection and effectiveness
Angiographic outcomes after EVT have shown a tendency toward greater success. According to an early period study, the reported overall successful recanalization rate was 70.5% [28]. In a recent trial, both the contact aspiration and stent retriever groups demonstrated higher rates of TICI ≥2b, exceeding 80-90% [50,99]. Furthermore, multiple combined techniques with minor variations have been updated, leading to nearly 100% successful reperfusion rates [57,103]. Achieving complete or near-complete reperfusion has been linked to better clinical outcomes and fewer adverse effects. Meanwhile, the proliferation of numerous variations and hybridizations of the technique has made it challenging for operators to select the appropriate technique for specific situations [68].
However, despite advancements in EVT techniques and increased expertise, complete reperfusion is only achieved in approximately half of cases, often necessitating multiple attempts and the use of rescue therapy. Moreover, the level of difficulty in performing EVT could be elevated by the underlying pathology of LVO.
Chronology of target for EVT
The extent of reperfusion achieved is among the few but most critical modifiable determinants for better clinical outcomes. The higher the amount of the reperfused tissue, and the lower the chance of penumbra evolving into infarction.
The modified Thrombolysis In Cerebral Infarction (mTICI) score, introduced in 2013, has been the main parameter for assessing angiographic outcomes, with most landmark studies demonstrating the superiority of EVT over medical treatment for LVO of AIS patients defining mTICI 2b or 3 as successful reperfusion for EVT [111]. Consequently, the target angiographic endpoint has been set to mTICI 2b, although further attempts for better reperfusion could be made. Predicting clinical outcomes concisely with mTICI 2b-3 is challenging due to the heterogeneity of the damaged volume in the cerebral hemisphere. A subsequent expanded TICI (eTICI) grade, which subdivides categories more finely into seven groups, has been shown to correlate incrementally with clinical outcomes [52]. With meaningful differences in clinical outcomes between mTICI 3 and mTICI 2b, the old-fashioned definition of successful reperfusion confronts its clinical efficiency [20,29,44]. This implies that maximal effect for reperfusion is desirable for clinical outcomes after EVT. Recently published studies have aimed to set successful reperfusion as eTICI 3 or 2c [80].
Additionally, achieving the best possible reperfusion with a single passage is considered another treatment goal of EVT. Maximal reperfusion after multiple attempts with passage of devices versus achieving maximal reperfusion with a single attempt of EVT seem to be two different scenarios. The first-pass effect (FPE), defined as complete revascularization (eTICI2c-3) following a single passage of the device without the need for rescue therapy, has been applied as a metric of mechanical thrombectomy success [108]. While it is controversial whether FPE is a major factor contributing to favorable outcomes or merely an epiphenomenon, studies have reported that FPE is an independent predictor of good clinical outcomes, regardless of procedural time. A matched case-control study, which controlled for onset-to-reperfusion time between single and multiple passages, has demonstrated that FPE improves clinical outcomes by reducing the likelihood of radiographically negative small embolic infarctions and periprocedural vessel injury, regardless of procedural time or duration of ischemic time [71,108]. Even among patients who achieve total recanalization after EVT, the presence or absence of FPE could still make a difference in clinical outcomes [8,71].
Debates regarding techniques of EVT
Numerous EVT techniques have emerged to improve the speed and quality of reperfusion, thereby increasing the likelihood of positive outcomes. Comparing the contact aspiration technique versus the stent retriever as a front-line technique may be somewhat outdated, given the variety of thrombectomy devices now frequently used in combination with advanced techniques.
Using direct aspiration in its infancy confronted the drawbacks of lacking catheters with a large enough diameter for sufficient aspiration and an absence of catheters with enough flexibility and atraumatic feature to navigate the tortuous intracranial vasculature. Therefore, at that time, the stent retriever technique became the predominant method for EVT, following landmark RCTs in 2015 [10,14,15,27,63,75,90]. But, with the availability of large-bore catheters that offer improved distal trackability, the contact aspiration technique, also known as A Direct Aspiration First Pass Technique (ADAPT), has gained favor.
Subsequently, two RCTs, ASTER (The Contact Aspiration vs Stent Retriever for Successful Revascularization) and COMPASS (Aspiration thrombectomy versus stent retriever thrombectomy as first-line approach for large vessel occlusion) trials, demonstrated similar procedural and clinical outcomes between the contact aspiration and stent retriever techniques [50,99]. After demonstrating the non-inferiority of aspiration thrombectomy in the COMPASS trial, subsequent studies have focused on determining which techniques are superior based on individual patient and clot characteristics. However, the preference for first-line techniques is still influenced by the facility and the interventionist [58].
Efforts to enhance the likelihood of successful reperfusion have led to combination techniques involving stent retrievers and large-bore aspiration catheters. When combined with proximal aspiration or flow arrest using a balloon guiding catheter, the technique commonly known as the Solumbra technique has undergone significant modifications and adaptations, resulting in heterogeneity in its application and outcomes [68]. Although reported rates of successful reperfusion (TICI ≥2b) have reached nearly 100%, this has resulted in a low level of evidence for each individual technique based on single-center experiences [57,103].
The ASTER2 trial, a RCT comparing the concomitant use of direct aspiration and stent retriever versus stent retriever alone, failed to demonstrate an improved rate of near-total or total reperfusion (eTICI2c/3) at the end of the EVT using combined technique. However, aspects such as a higher FPE, a lower number of attempts, and a lower rate of distal embolization associated with the usage of the combined technique are encouraging [49].
Considering the first-line thrombectomy technique for the posterior circulation, recent studies suggest that contact aspiration may result in better clinical outcomes compared to the stent retriever, contrary to the leveled outcomes observed in anterior circulation EVT [26,55]. The STAR collaboration, which compared the effects between the combined technique and direct aspiration alone, showed that first-line contact aspiration could achieve better reperfusion and clinical outcomes than the combined techniques [2]. The ongoing pc-ASTER trial (NCT05320263) aims to elucidate which technique, either contact aspiration or stent retriever, is better for the treatment of BAO.
The question of how to achieve the best angiographic results remains unanswered. Despite numerous inconclusive and contradictory reports regarding the superiority of different EVT techniques, it is important to reflect on the changing paradigm of the thrombectomy goal.
Rescue strategies for formidable cases of EVT
While EVT has shown promising results for many AIS patients, certain subsets face challenges in deriving benefits from it. Notably, cases involving underlying intracranial atherosclerotic stenosis (ICAS) represent formidable obstacles. ICAS has been identified as a prevalent cause of LVO, particularly among Asian and African American populations [97]. Detecting ICAS before undergoing EVT can be particularly challenging, especially in patients lacking clear angiographic clues, such as intracranial vessel calcification, concurrent ICAS in other intracranial vessels, fluctuating symptom presentations, or a well-established preprocedural leptomeningeal collateral status [7,13]. A substantial proportion of ICAS-related LVO cases require multiple passages, with or without reperfusion, leading to delayed reperfusion times and cumulative risks of procedural complications. Skepticism regarding the use of empirical angioplasty or stenting for reperfused ICAS-related LVO (when TICI ≥2b has been maintained) for the preventive purpose of reocclusion is based on concerns about the potentially high rate of periprocedural complications [18,66,73,109]. Meanwhile, in clinical practice, instances of failed reperfusion following multiple attempts with conventional EVT techniques call for the development of contingency plans that involve alternative methods. These rescue techniques encompass balloon angioplasty, intraarterial thrombolytics with glycoprotein IIb/IIIa inhibitors, intracranial stenting, and various combinations of these techniques [43,81]. Limited evidence, primarily from a few observational studies conducted mainly in Asian populations, has reported positive effects on target vessel patency and improved functional outcomes, all without an increase in intracranial hemorrhage or mortality rates [6,74]. When comparing the effectiveness of different rescue strategies, it was observed that the combination of rescue stenting and thrombolytic infusion resulted in a better reperfusion rate and more favorable outcomes compared to using a single rescue modality [5]. Ongoing ANGEL REBOOT (Randomised study of bailout intracranial angioplasty following thrombectomy for acute large vessel occlusion; NCT05122286) aims to assess the efficacy and safety of rescue intracranial stenting following failed EVT in acute AIS LVO, regardless of the underlying etiology of the stroke.
CONCLUSION
Based on positive high-quality data, justifying the expanded application of EVT for AIS to a wider population through guideline changes seems reasonable. Optimizing reperfusion and minimizing the number of passages during endovascular procedures are key objectives for improving clinical outcomes. Despite institutional or provider variability in procedural techniques, efforts to investigate controversial issues should continue.