INTRODUCTION
Subarachnoid haemorrhage (SAH) due to intracranial aneurysm (IA) rupture results in high mortality and morbidity rates. The risk of SAH due to IA rupture is 2% per year. The mortality rate of SAH is approximately 60% in the first 6 months [1-3,22]. Recently, surgical treatment of aneurysms has decreased, especially in some centres, due to the widespread use of endovascular modalities [13,14]. However, surgery remains the first-line treatment for complex aneurysms not suitable for endovascular treatment and for anterior circulation aneurysms [21,24].
Nowadays, in surgical training, clinical experience is traditionally gained through cadaver courses and by observing different procedures. Nevertheless, the cost of cadavers is gradually increasing for surgical training, and in several countries, obtaining cadavers is difficult. Furthermore, many hospitals and training centres offer several opportunities for neurovascular surgery and many types of surgical operations. A way of learning intracranial anatomy and neurovascular diseases is to use medical simulators for procedural training. With the help of simulation, young surgeons and surgeon candidates may combine theoretical knowledge with physical processes and surgical techniques.
Three-dimensional (3D) printers are advanced technological devices that convert 3D models, designed with the aid of computers, into real physical objects. Currently, 3D printing technology provides simulation from models obtained from medical imaging data as customised models, which are effective in developing surgical strategies and plans. Aneurysm simulation using 3D printing is especially important for training young neurosurgeons [11,12,17,18,24]. These models are useful in visualising aneurysm locations, sizes, and dimensions, as well as the direction of the aneurysm. It is also helpful in analysing the relationship between the aneurysm and the main artery. According to the literature, surgical planning has been previously performed using 3D aneurysm models; however, no prospective studies have been conducted regarding this topic [11,12,17,18,24].
This prospective study was conducted to compare patients who underwent preoperative planning performed using 3D modelling and 3D printing with those who did not undergo preoperative planning using the aforementioned techniques, in terms of surgical time and outcomes.
MATERIALS AND METHODS
In this study, the medical records of 47 patients with aneurysms who were treated between 2018 and 2019 in our clinic were evaluated. The Ethics Committee of Ege University approved this study (approval No. 193T/25). The demographic data of the patients; Glasgow coma scale (GCS) scores at admission, surgery, hospitalisation, and follow-up; postoperative modified Rankin scale (mRS) scores; and Glasgow outcome score were examined. The patients were clinically evaluated using the Hunt-Hess grading system, while radiological evaluation was performed using the Fisher grading system. Three patients with negative angiogram and four patients with multiple aneurysms were excluded, and 40 patients were finally enrolled in this study and were divided into two groups : group I (n=20) consisted of patients who did not undergo preoperative surgical planning using a 3D printer, and group II (n=20) comprised patients who underwent preoperative surgical planning using a 3D printer (Figs. 1-6). The study was terminated when both groups reached a total number of 20 patients per group. All surgical clippings of the aneurysms were performed by the same experienced neurovascular surgeon. Pterional craniotomy was performed in 37 patients, and anterior interhemispheric craniotomy was performed in three patients.
Creation of 3D models
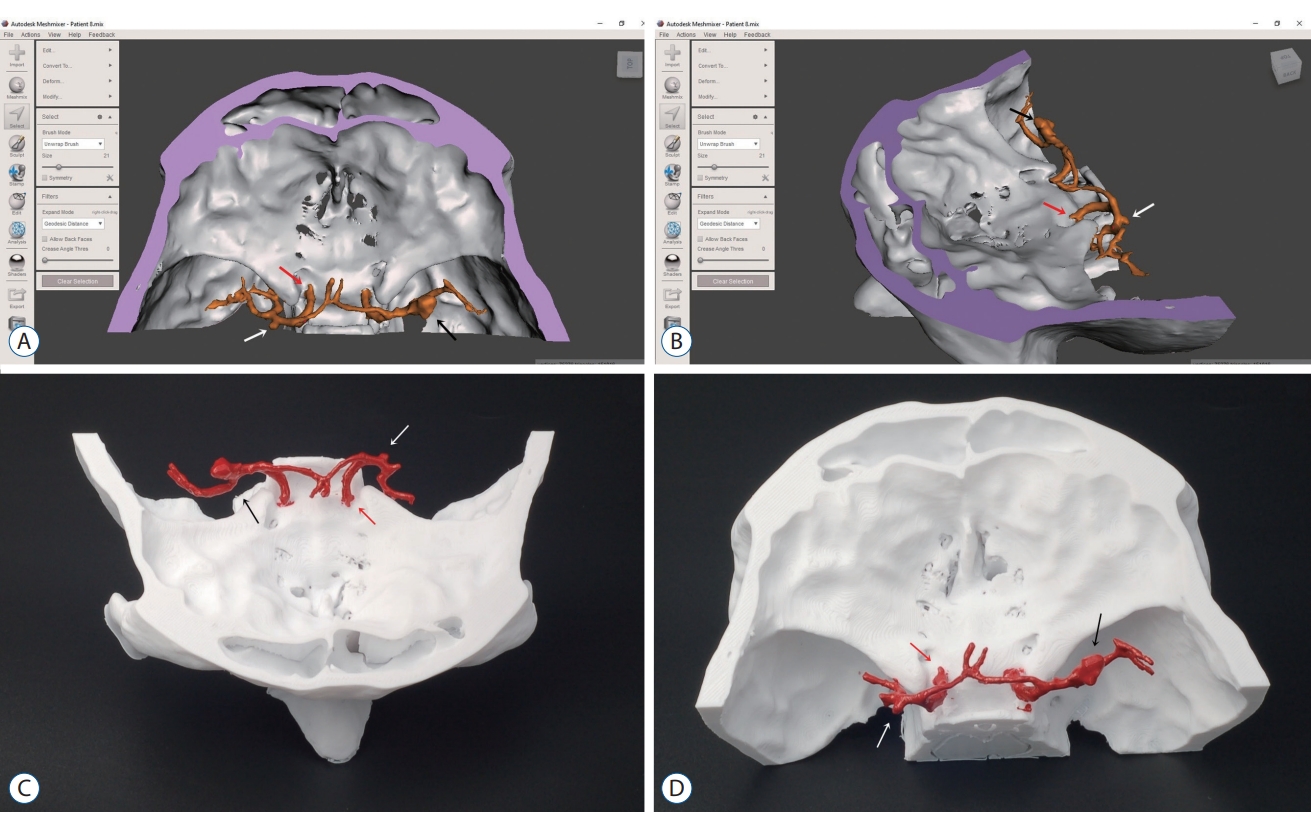
Digital Imaging and Communication in Medicine images obtained from computed tomography angiography (CTA) (Siemens Healthcare, Forchheim, Germany) images were reconstructed to create 3D models. Multidimensional datasets (axial, coronal, and sagittal) were transferred to a 3D Slicer (version 4.8; Isomics, Inc., Cambridge, MA, USA), a reconstruction software. Reconstruction of the intracranial artery was performed using a 3D Slicer after format conversion and extraction procedures. Subsequently, a masking procedure was performed. Segmentation was performed to isolate the cranium and aneurysmal main vessel geometries as binary masks. The data were converted to the stereolithography (STL) format for production using 3D printers. These procedures were performed by the same neurosurgeon and engineer in the study group.
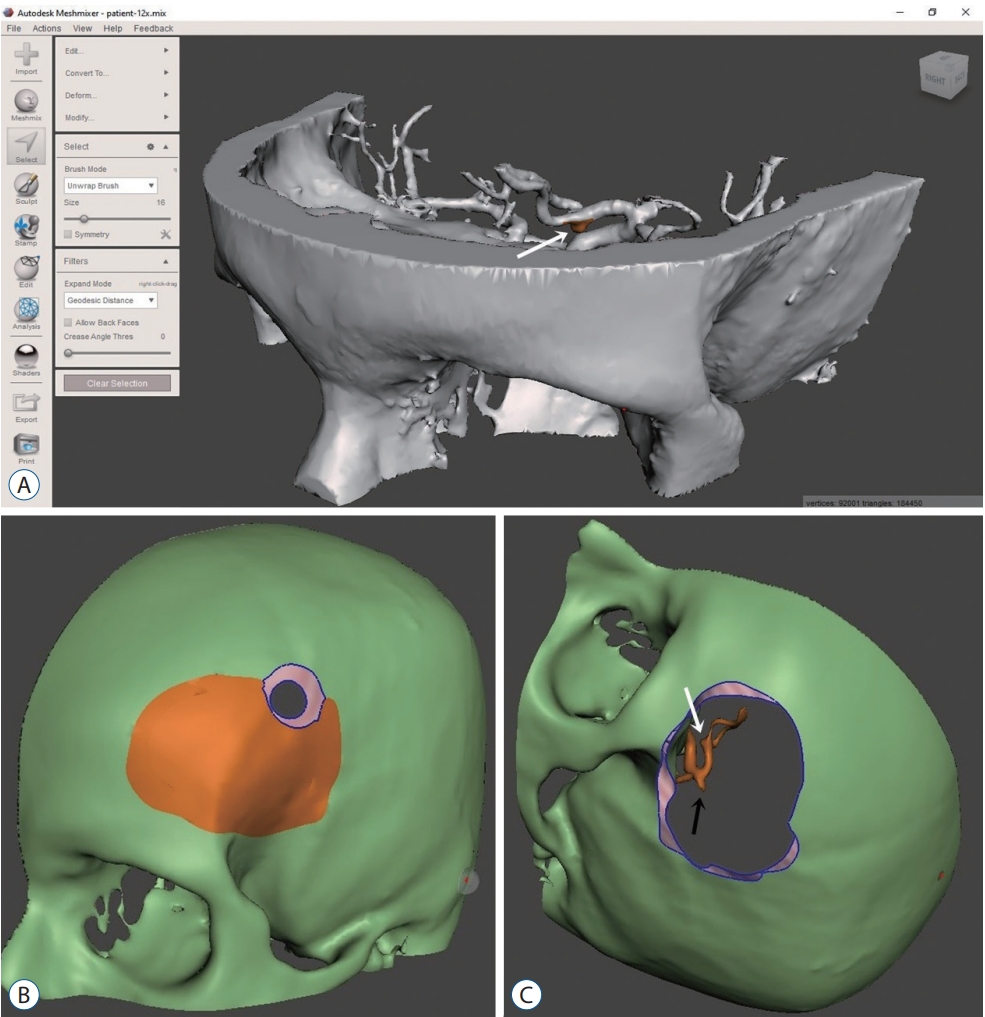
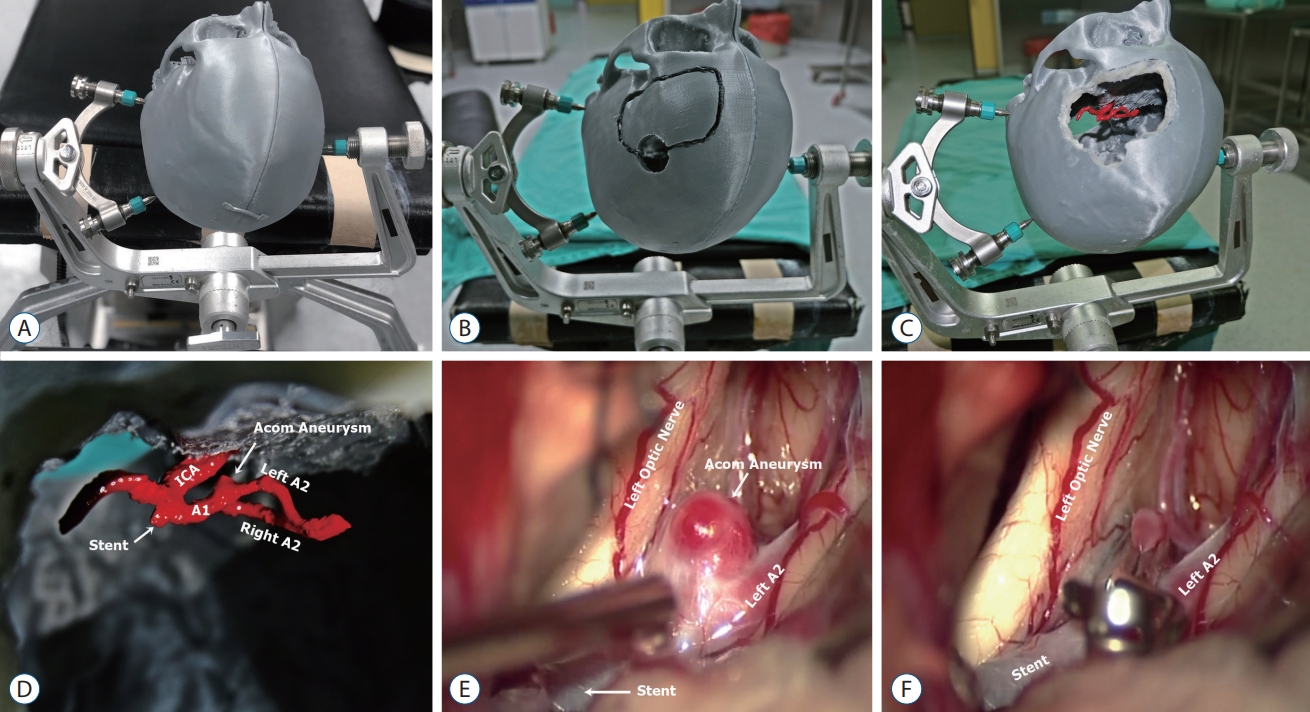
For the model, a 3D engineering software with the SLT file format was used for image processing of the targeted region. A Meshmixer (Autodesk Inc., San Francisco, CA, USA) was downloaded using the STL editing software for surface cleaning, mesh optimisation, smooth structure processing, and surface deformation removal on the created model. The model was then sliced using the Cura software (version 4.8.0; Ultimaker BV, Utrecht, Netherlands) to create G codes. After processing by various operations, the solid model was finalised by removing surface mistakes. The procedure settings were standardised as follows: extruder temperature, 215°C; room temperature, 24°C; primary layer height, 0.1 mm; and filling rate, 20%. The 3D models of the cranium and aneurysm were printed in double colour using Ultimaker 3 Extended (Ultimaker BV) and a dual extruder desktop 3D printer using polylactic acid as the main material in a 1 : 1 ratio. The printing procedure lasted 4-36 hours. The surgical team chose the best approach and the clipping procedure after working on the 3D model. The most favourable clips were prepared for surgery. Since our clinic is a reference center, most of our patients usually apply to us on the first day of bleeding time. In our clinic, hyperacute surgery is not performed except for re-bleeding. This saves us the time needed for 3D printing.
In three patients who underwent urgent surgery, only aneurysm modelling was performed; for the remaining patients, elective surgery was planned, and the lesion was modelled from the skull base. The models of the patients who underwent urgent surgery could only be examined perioperatively, whereas longer examination of the models of patients who underwent elective surgery was possible. After the printing process, the models were transported to our hospital in approximately 30 minutes.
Statistical analysis
The study data were statistically analysed using the Statistical Package for the Social Sciences (SPSS version 22.0; IBM Corp., Armonk, NY, USA). Data and median values of the data were processed and transferred to the statistical analysis program. The Mann-Whitney U-test was used to compare the mean differences, whereas the chi-squared test was used to compare ordinal and dichotomous variables. Statistical significance was set at p<0.05.
RESULTS
The mean patient age was 54.8±12.9 years (range, 26-79). Twenty-one patients (52.5%) were women and 19 (47.5%) were men. The average hospitalisation time was 14.6±12.9 days (range, 4-75). The mean GCS score was 13.7±2.6 (range, 5-15) (Table 1) at admission to the clinic. SAH was observed in 30 patients (75%). Among the 40 patients, 21 had a history of smoking. The average aneurysm volume was 149.9±155.4 mm3 (range, 5.2-658.8). Time interval between the SAH ictus and surgery is 2.9±1.1 days for 16 patients at group I, 3.2±0.8 days for 14 patients at group II (p=0.539).
Furthermore, among the 40 patients, 23 (76.7%) were ≤2 according to the Hunt-Hess grading system, and 24 were ≥3 according to the Fisher grading system. In this series, the most common IA localisation was the middle cerebral artery (MCA) (n=18, 45%), followed by the anterior communicating artery (n=12, 30%).
All patients underwent surgical clipping. The average time of surgery was 170.0±16.5 minutes (range, 150-210) in group I and 134.0±24.5 minutes (range, 90-180) in group II. The difference was statistically significant between the two groups (p<0.001). However, no significant differences in the initial GCS score (p=0.229) or hospitalisation time (p=0.838) were observed between the two groups.
In group II, in the three patients who had to be operated urgently, only aneurysm modelling was performed. Postoperatively, 11 patients (five in group I and six in group II) showed signs of vasospasm, and six patients had ischemia. Only one patient in each group had wound problems but were treated without the need for additional surgery.
Postoperatively, the mRS score was used to assess the status of the patients (Tables 2 and 3). The mean follow-up duration of the patients was 12.1±1.9 months (range, 8-15). Only six patients had transient neurological deficits in the early postoperative period. Furthermore, 35 patients were discharged without any complications. However, 11 patients developed vasospasm; one of them was GCS 3 and grade V on the World Federation of Neurological Surgeons grading system (before surgery), one patient had cerebrospinal fluid leakage, and five patients had pneumonia. One patient died in each group.
IA rupture is a disturbing condition for surgeons to consider even during preoperative planning. It can have dramatic effects on the morbidity and mortality of the patients. In this series, it occurred in three patients in group I, whereas only one patient in group II had IA rupture.
DISCUSSION
SAH caused by a ruptured IA remains a significant cause of morbidity and death, and despite the rapid development of endovascular treatment modalities, microsurgical clipping of IAs is a long-lasting, reliable treatment with a low recurrence rate [4,5,7,10,23].
Preoperative preparation with the evaluation of the angiograms, as well as the surgical experience of the surgeon, is important for successful IA clipping. In this study, the results of patients with personalised 3D aneurysm models were compared with those of the non-model group.
IA surgical training consists of cadaver model simulation and radiological 3D models; however, 3D solid model simulations have recently been used [9,11,12,18,24,25]. 3D printing is superior to the other two methods in terms of obtaining information from patients. Personalised models are used in all surgical fields, not only in neurosurgery. In particular, in cranioplasty operations, the advantage of these models is indisputable [16]. A surgeon’s understanding of pathology by seeing and touching is superior to seeing only.
3D models have different timing and costs in solid model production owing to the type of 3D printer. Mashiko et al. [11], using colour ink-jet printers, have produced models in approximately 3 days. Ploch et al. [17] have printed silicon brain models in 24 hours, whereas Wang et al. [24] have printed cranium and aneurysm models in approximately 13-22 hours. In this study, using fused deposition modeling-type printers, the models were printed in 4-36 hours. Ryan et al. [18] simulated the clipping techniques for young neurosurgeons using 3D models. After the training of aneurysm clipping, 14 residents concluded that this simulation is beneficial in terms of education [18]. Wang et al. [24] compared six aneurysm models to bone and aneurysm models using computed tomography angiography; both were found to be useful. In a different study by Wang et al. [25], eight MCA aneurysms were modelled, and a survey was performed. Although the models were found to be useful, the thickness of the aneurysmal wall was not composed well enough [25]. Mashiko et al. [11] developed three unruptured MCA bifurcation aneurysm models using a 3D printer. The skull base, dura mater, arachnoid mater, cerebrum, arteries, and veins were modelled. Using this 3D model, a hollow silicon model was produced, and clip application was performed, which was shown to be useful for training young neurosurgeons [11]. In our study, with the help of surgical models, inexperienced surgeons in the surgical team understood the surgical planning more easily. With clip preparation beforehand, the surgery time was significantly reduced in both groups. This proves that in the future, surgical simulation will be further developed to decrease morbidity and mortality. In this study, the shorter surgery time in the 3D model group was found to be statistically significant. The anaesthesia time, medications, blood transfusions, and risk of infections will also be reduced. In the literature, a shorter surgery time is related to low infection and morbidity rates [10,25].
Recently, clipping and coiling have been compared in all randomised studies. The International subarachnoid aneurysm trial has claimed that endovascular treatment is superior to clipping in the first year; however, in follow-ups, recurrence of haemorrhage was significantly higher in coiled patients [14]. Furthermore, the methodology of the trial has been heavily criticised after being published [6]. In the Barrow Ruptured Aneurysm Trial (BRAT) study, no difference in morbidity was observed between the treatment groups, and no re-haemorrhage was observed in patients who underwent surgical clipping [20,21]. The recent BRAT study has revealed that surgical clipping remains valuable in treating aneurysms.
In this study, vessel models were produced using solid models; hence, assessing the vessel wall thickness was difficult. Determining the relationship between the cranial nerves on CTA is difficult. Since perforated anterior communicating arteries are submillimetric, they could not be shown in the solid model, and this was the most important limitation of this methodology. This caused us to be unprepared for millimetre perforators coming out of the aneurysm during the real surgeries. Age is important for prognosis; in this study, the prognosis was worse in patients aged >50 years [26]. Nanda et al. [15] did not show the effects of age on prognosis in patients with unruptured aneurysms. The aneurysm occlusion rate was 94% in these patients after surgical clipping [15]. In a study by Jabbarli et al. [8], in patients with unruptured aneurysms, the morbidity rate was 2.5-8.5%, the mortality rate was 0-3.2%, and the postoperative complication rate was 25%. Song et al. [19] have shown that in patients with unruptured aneurysms, the morbidity rate was 0.5%, the mortality rate was 0.3%, and the postoperative complication rate was 2.8%. In this series, 10 patients (25%) had unruptured aneurysms.
CONCLUSION
Preoperative studies were conducted using one-to-one intracranial vessel modelling with the help of 3D printers, and a prospective comparison was made for the first time in the literature. Recently, 3D printers have been widely used in medical sciences; using this technology in neurosurgical practice with proper modifications and adaptation shows better results in terms of time and morbidity not only for aneurysms but also for tumour vascularization and spinal surgery. In order to exclude other factors, comparative study should be done only in the unruptured cerebral aneurysm group.