INTRODUCTION
Traumatic brain injury is a leading cause of injury-related disability and death worldwide, resulting in huge burdens on society [14]. In general, severe traumatic brain injury (sTBI) is defined as a Glasgow coma scale (GCS) score of ≤8 and is closely associated with high mortality and poor prognosis [18]. Intracranial pressure (ICP) mostly increases in the acute stages of brain injury, which causes additional injury to the brain resulting in negative functional consequences [3,20]. Accordingly, the importance of ICP management in patients with sTBI is widely known. Since second injury caused by a brain injury is preventable, it is important to detect and treat increased ICP through ICP monitoring [9,23].
The recent Brain Trauma Foundation guidelines provide a level IIB recommendation for ICP monitoring in salvageable patients with sTBI [2]. However, previous studies have shown that the incidence of ICP monitoring has high variations [1,4-7,9,11,15,19,26]. Furthermore, each study reported different opinions on the relationship between ICP monitoring and prognosis among patients with sTBI [3,4,9,11,13,16,17,19,23].
The Korean Neurotraumatology Society (KNTS) conducted a databank project for patients with neurotrauma in Korea, and many studies have been conducted based on the data generated [8,21]. Currently, data on patients with sTBI are registered in the second Korea Neurotrauma Databank (KNTDB).
This study aimed to investigate the current status of ICP monitoring in Korean patients with sTBI and to explore the association between ICP monitoring and patient prognosis using data from the second KNTDB. Further, a survey was administered to Korean neurosurgeons to investigate the perception of ICP monitoring in patients with sTBI.
MATERIALS AND METHODS
The second KNTDB project had been conducted with approval from each hospital’s Institutional Review Board (IRB). This study was approved by Pusan National University Hospital’s IRB (IRB No. 2018-008-105 and 2205-021-115).
Study design
First, we extracted ICP-related clinical data from the second KNTDB to conduct this study. The inclusion criteria of this databank for patients are as follows : age ≥18 years; sTBI, defined as a GCS score of ≤8 points; and abnormal findings on brain computed tomography (CT). The clinical data of 1198 patients were collected from 20 hospitals nationwide from September 2018 to March 2022.
Next, an online survey was administered to investigate the perception by Korean neurosurgeons regarding ICP monitoring in patients with sTBI (see Supplementary Material 1). The survey was conducted for neurosurgeons working for hospitals that provided care for patients with sTBI. Hospitals that provide care for patients with sTBI must include a functional emergency room, intensive care unit (ICU), and operation room. In addition, neurosurgeons who were interested in brain injury and able to provide professional care were included for the survey.
Patient selection and clinical data collection from the neurotrauma databank
For this study, we selected patients with extended Glasgow outcome scale (EGOS) score data over 6 months among adults with sTBI with a GCS score ≤8 points from the databank. In addition, the following clinical data were collected : age, sex, trauma center, GCS on admission, cause of injury, pupil reflex, systolic blood pressure on admission, Rotterdam score of initial brain CT scan, ICP monitoring, mortality, and 6-month EGOS scale.
Neurologic outcome was evaluated based on the scores of 6-month EGOS, which was categorized into the following : 1) death, 2) vegetative state, 3) lower severe disability, 4) upper severe disability, 5) lower moderate disability, 6) upper moderate disability, 7) lower good recovery, and 8) upper good recovery. These were dichotomized into the following : “unfavorable outcome,” defined as an EGOS score of 1-4, and “favorable outcome,” defined as an EGOS score of 5-8 [24].
Survey
We sent an online survey named “current status and perception of ICP monitoring in Korean patients with sTBI” to a total of 399 neurosurgeons. The survey was composed of the following five domains : 1) types of hospitals where the respondents worked, 2) personal information of the respondents, 3) ICP monitoring for patients with immediate craniectomy/craniotomy, 4) ICP monitoring for patients without immediate craniectomy/craniotomy, and 5) activation of ICP monitoring in patients with sTBI. Specific items are mentioned in Table 1.
RESULTS
Outcome of ICP monitoring in patients with sTBI
Among the 1198 patients with sTBI registered in the databank, 286 patients with no clinical data were excluded, and a total of 912 patients were included for analysis. Among them, 79 (8.7%) underwent ICP monitoring. ICP monitoring sensors were classified into a subdural, ventricular, and parenchymal types, which were used for 52 (65.8%), 11 (13.9%), and 16 (20.3%) patients, respectively. Spiegelberg® (Spiegelberg GmbH & Co. KG, Hamburg, Germany), Codman® (Integra LifeSciences, Princeton, NJ, USA), and LiquoGuard® (MÖLLER Medical, Fulda, Germany) ICP monitors were used for 38 (48.1%), 35 (44.3%), and two (2.5%) patients, respectively. ICP was monitored manually in the remaining four patients (5.1%).
Patients included in the study were divided into either a group with ICP monitoring or a group without, and the clinical characteristics of each group were analyzed (Table 2). The overall mean age was 58.46±17.45 years, and 697 patients (76.4%) were men. Patients who underwent ICP monitoring were found to be significantly younger. The most common cause of injury was traffic accident (40.9%), followed by a slip down (22.4%) and fall (21.4%). Among the 912 patients, 540 patients died, resulting in overall mortality of 59.2%. The outcome was assessed at 6 months after injury, and 225 patients (24.7%) showed favorable outcomes. Mortality and favorable outcomes between the patient groups with and without ICP monitoring were compared, and the difference was not statistically significant.
Types of working hospitals and personal information
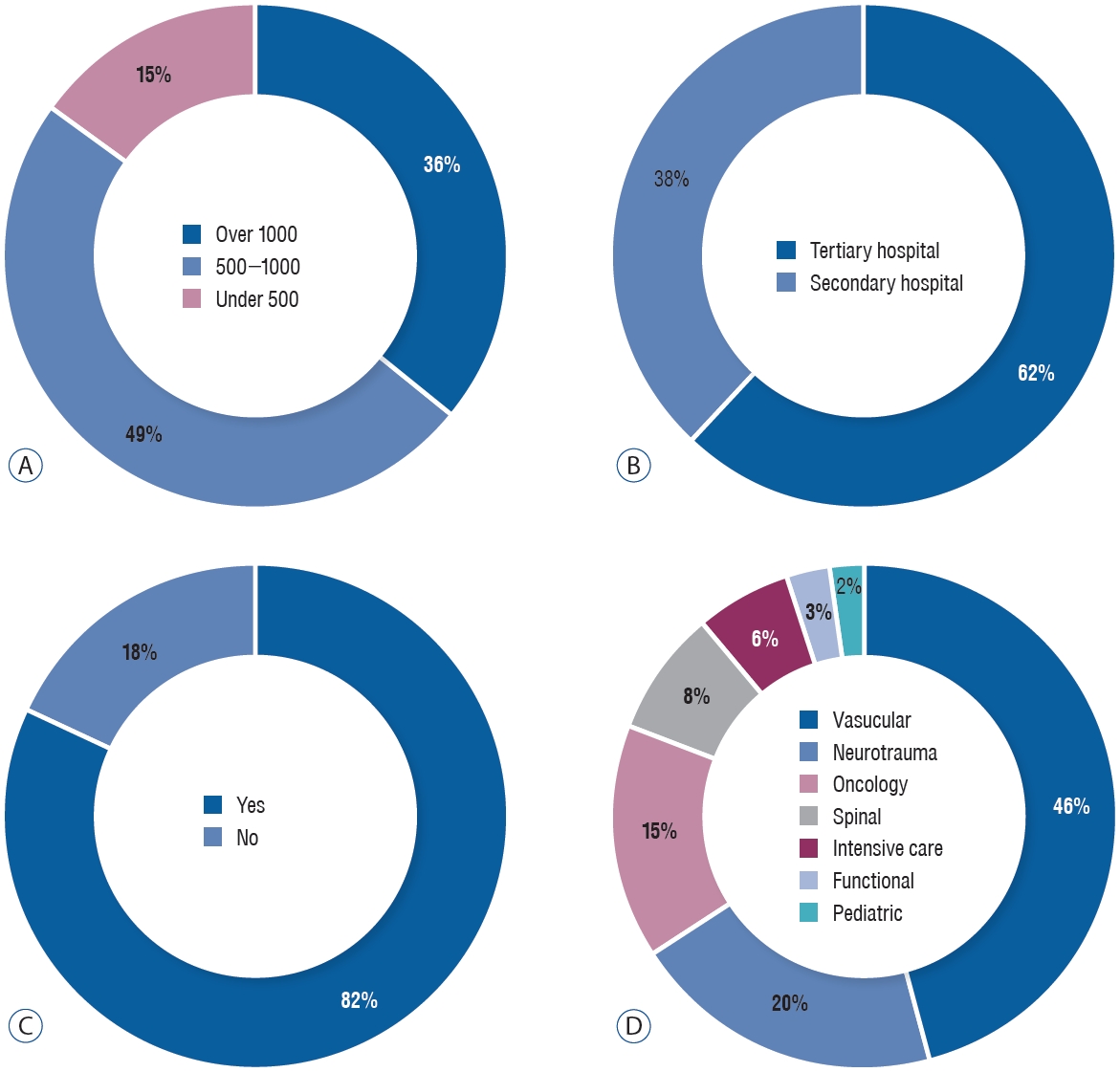
According to the survey, 22 respondents (36%) answered that they worked at hospitals with more than 1000 hospital beds, and 30 (49%) and nine (15%) respondents answered that they worked at hospitals with 500-1000 and <500 hospital beds, respectively (Fig. 1A). The proportions of those who worked for tertiary hospitals and secondary hospitals were 62% (n=38) and 38% (n=23), respectively (Fig. 1B). Overall, 50 respondents (82%) at the time were working at training hospitals for neurosurgery residents (Fig. 1C) and 20 respondents (32.8%) worked at hospitals with regional trauma centers.
Among the subspecialties mentioned in the survey, most neurosurgeons who responded were interested in vascular part, which accounted for 46% (n=28), followed by neurotrauma (n=12; 20%), oncology (n=9; 15%), spinal (n=5; 8%), intensive care (n=4; 6%), functional (n=2; 3%), and pediatric (n=1; 2%) parts (Fig. 1D). Only 10 respondents (16.4%) were trauma neurosurgeons who were dedicated to trauma patients only. There were 30 respondents (49.2%) who had more than 10 years of clinical experience, and 22 (36.1%) and nine (14.8%) respondents had 5-0 and <5 years of clinical experiences, respectively. Regarding clinical experiences with patients with sTBI in the past 3 years, 22 (36.1%) and 36 (59%) respondents had treated 5-20 and >20 patients annually, respectively.
ICP monitoring in patients who underwent immediate craniectomy/craniotomy
For a question (Q9) about whether the patients with sTBI who underwent immediate craniectomy/craniotomy were monitored for ICP, 18 respondents (29.5%) answered that they always monitored ICP, 24 (39.3%) selectively monitored ICP, and 10 (31.1%) never monitored ICP. The 24 respondents, who answered to Q9 that they selectively monitored ICP, were asked about the reason why ICP monitoring was not considered (Q10). Most of them (51.4%) answered that “ICP was sufficient reduced and good outcome was expected because no cerebral edema was observed.” The next highest stated reason (25.7%) was “exacerbation of clinical progress was expected due to severe cerebral edema,” followed by (14.3%) “surgery was stopped early because patient’s hemodynamic state was unstable.” Other reasons included “no extra equipment was available” and “a catheter for ventricular puncture was absent.”
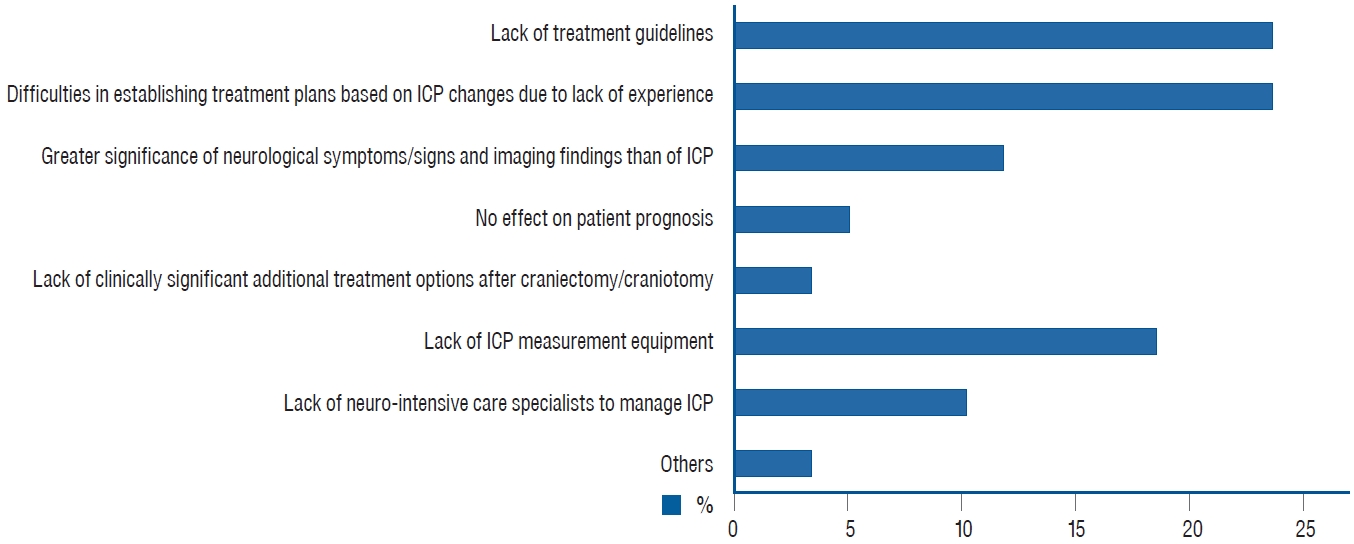
The 19 respondents who answered for Q9, “I have never monitored ICP after craniectomy/craniotomy,” were asked the reasons why they did the same (Q11). A total of 59 responses were selected. The answers are summarized in Fig. 2. Other reasons included “due to risk of infection” and “due to unidentified safety of the device.”
ICP monitoring in patients without immediate craniectomy/craniotomy
For a question (Q12) about whether they monitored ICP on deciding that no immediate craniectomy/craniotomy was necessary for patients with sTBI, only two respondents (3.3%) answered that they “always monitored” ICP. For the same question, 30 respondents (49.2%) answered that they “selectively monitored” ICP (they do or do not based on clinical situations) and 29 respondents (47.5%) answered that they “never monitored” ICP. The 30 respondents who answered for Q12 that they “selectively monitored” were asked to explain the clinical situations where ICP monitoring was required (Q13). Ten respondents (18.9%) answered “neurologically unassessable due to surgery/procedures performed in other departments owing to multiple traumas,” 14 (26.4%) and 28 respondents (52.8%) answered “neurologically unassessable due to the necessity of sedation” and “exacerbation of edema and hematoma determined based on clinical experiences,” respectively. Other answers included “due to the presence of a catheter for ventricular puncture.”
For a question about the place where a sensor was inserted for ICP monitoring if no craniectomy/craniotomy was performed, 21 (65.6%) and 11 (34.4%) respondents answered operation room and ICU, respectively. For a question about the time of inserting a sensor for ICP monitoring, 15 respondents (46.9%) answered “a sensor is inserted immediately after the hemodynamic state is stable,” 14 (43.8%) answered “between 2 to 8 hours after additional head CT scan was performed to monitor progression” and one (3.1%) answered “persistent deterioration of consciousness even after the duration (8 hours) of recovering from a concussion.” Other answers included “right after admission to the ICU.”
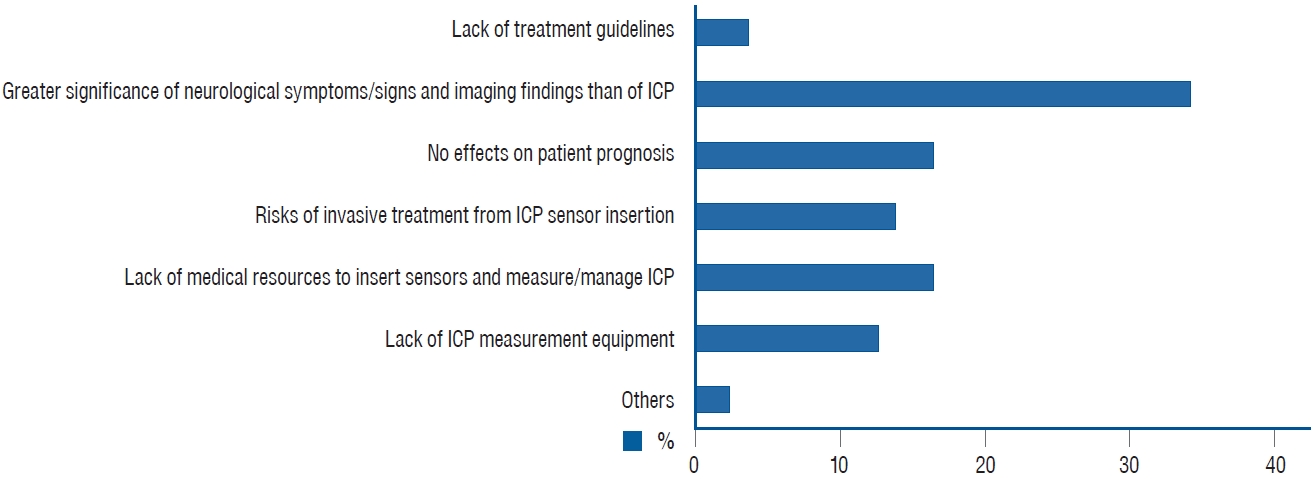
The 29 respondents who never monitored ICP (Q12) were asked for the reasons (Q16). A total of 79 responses were selected. The answers are summarized in Fig. 3. Other reasons included “It may be better to do craniectomy/craniotomy right away if ICP monitoring needs.” and “Since the ICP sensor insertion is also included in surgery, there is a burden on this.”
Activation of ICP monitoring in patients with sTBI
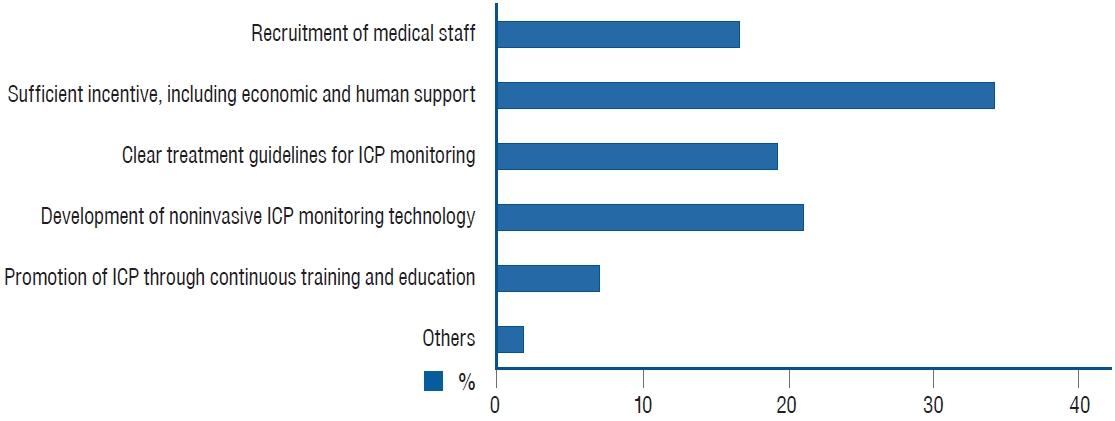
For a question (Q17) about the factors necessary for increasing ICP monitoring in patients with sTBI, a total of 114 answers were selected. The answers are summarized in Fig. 4. Among other opinions included, one stated “when performing craniectomy/craniotomy after ICP monitoring, legal protection is needed if surgery is inevitably delayed.”
DISCUSSION
According to many studies on ICP monitoring in patients with sTBI, the proportions of performing ICP monitoring are known to vary, ranging from 9.6% to 64% [1,4-7,9,11,15,19,26]. In this study, the proportion of performing ICP monitoring for Korean patients with sTBI was 8.7%, which was significantly lower than the proportions reported in previous studies. Although data analyzed in this study were not collected from all hospitals in Korea, we believe that data were uniformly collected from multiple areas nationwide, as a project which was conducted by the KNTS. Therefore, this study is somewhat representative of the overall trend, which we believe to be not much different from the actual trend.
However, several studies demonstrated better outcomes in terms of prognosis, length of ICU stay, and mortality when performing ICP monitoring [3,9,16,22,23]. Recent studies have reported that ICP monitoring can be helpful in managing patients [12,16,25]. However, this study did not show statistically significant differences in the mortality and 6-month neurological outcome between the groups with and without ICP monitoring. Surely, there are studies reporting that ICP monitoring is not helpful in managing patients [4,5,8,11]. In this study, no analysis was performed on the factors (length of hospital stay, mortality within 2 weeks, and duration of mechanical ventilation) associated with ICP monitoring’s effects on patients with sTBI [9,10]. Furthermore, although the number of patients analyzed in this study was not small, the number of patients who underwent ICP monitoring were insufficient to completely evaluate its efficacy. Well-designed prospective studies are required to identify the roles of ICP monitoring in patients with sTBI.
We administered the survey to neurosurgeons to additionally analyze the reasons for the low rate of ICP monitoring in patients with sTBI in Korea. As a result of this survey, 70% of neurosurgeons responded negatively to performing ICP monitoring after craniectomy/craniotomy, while 96.7% of neurosurgeons responded negatively to performing ICP monitoring when craniectomy/craniotomy was not performed. The reasons why ICP monitoring was not performed were investigated, and most respondents answered that there were no actual guidelines for, or experiences with, ICP monitoring post craniectomy/craniotomy. In cases wherein which craniectomy/craniotomy was not performed, most respondents answered that ICP monitoring was not helpful because other neurological signs or imaging findings were comparatively more important. Next, for both abovementioned cases, most respondents added that the lack of sources (medical staff or operation rooms) or equipment was another reason. In summary, the low rate of ICP monitoring in patients with sTBI is mainly attributed to insufficient guidelines and experiences and a lack of medical sources and equipment. Since establishment of actual guidelines require many additional studies, it is hard to accomplish within a short period of time. In contrast, problems with medical resource and equipment can be resolved within a relatively short period of time by improving medical expenses for ICP monitoring, reflecting it in hospital evaluation, and providing additional incentives to the medical staff. Higher rate of ICP monitoring in patients with sTBI can resolve the problem of insufficient experience and can be helpful in future studies since there would be sufficient data to use. In addition, in this survey, most respondents’ answers for the question about activation of ICP monitoring included that economic or institutional incentives could be helpful in increasing ICP monitoring. Accordingly, to promote ICP monitoring, distribution of human resources and financial support are preferentially required, and additional incentives for ICP monitoring should be considered.
CONCLUSION
The rate of ICP monitoring in patients with sTBI was relatively low in Korea, and there was no association between the ICP monitoring and the mortality and neurological prognosis. Korean neurosurgeons somewhat negatively recognized ICP monitoring for patients with sTBI. Adequate medical staff and financial support are required to improve the frequency of ICP monitoring in Korea. Future large-scale, well-designed studies are warranted to better understand the necessity of ICP monitoring.