INTRODUCTION
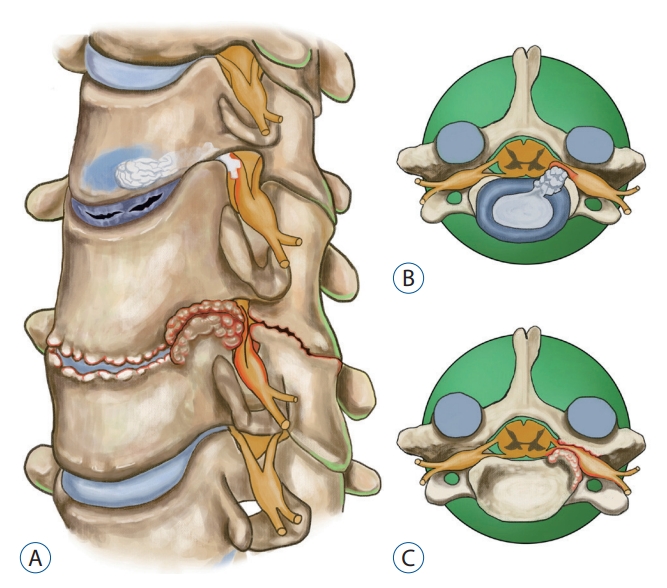
Cervical spondylotic radiculopathy (CSR) is a common disease resulted from cervical degenerative changes. The common cause of damage to cervical nerve root is either lateral disc herniation or osseous nerve root canal stenosis [4,25] (Fig. 1). Conservative therapy is recommended for at least 2 months in the treatment of CSR without myelopathy. Surgical decompression should be considered if conservative therapy fails [11].
Microscopic anterior cervical discectomy and fusion (ACDF) has been considered as the golden standard treatment for CSR [16]. However, the complications attributed to ACDF cannot be ignored although the overall incidence is not high, including symptomatic adjacent disc disease, pseudoarthrosis, instrumentation failure, and ventral approach-related complications, etc. [5,6,8,15,21]. Posterior cervical foraminotomy (PCF) with or without discectomy is another classic operation for the treatment of CSR and serves as an alternative to anterior cervical surgery. It has good therapeutic effect similar to that of anterior surgery with the added characteristics, such as avoiding the trouble related to the approach, instrumentation and fusion, preserving motor function and decreasing the incidence of adjacent level degeneration [1,13,18,20].
With the great improvement of percutaneous endoscopic spine surgery during the past several decades, the posterior endoscopic cervical foraminotomy (PECF) has gradually got popular for the treatment of CSR [7,26,28]. More and more studies have demonstrated PECF provides equivalent outcomes to microsurgical PCF with better visualization, less soft tissue injury, shorter rehabilitation time and less hospital length of stay [7,10,19,24,26,28].
Endoscopic high-speed drill is the mostly used tool for grinding bone in PECF. Posterior endoscopic cervical discectomy can be performed on the basis of PECF when the ventral compression to the nerve root comes from lateral soft disc herniation (Fig. 1B) [23]. It is an ideal model because the surgical decompression to the affected nerve root is direct decompression. However, osseous nerve root canal stenosis is a different condition, usually resulted from hyperplasia of Luschka joint, calcified discs, hyperplastic ligaments and loss of the intervertebral height (Fig. 1A and C); using a high-speed drill to grind these hard lesions in the ventral region of the nerve root and dura is a relatively high-risk manipulation. For this reason, the currently mainstream is dorsal decompression without ventral bony resection. Most of the time, this kind of indirect decompression is enough to alleviate clinical symptoms. However, this method which is less attractive sometime will not achieve famous performance due to insufficient decompression [22,29].
In recent years, the emergence of endoscopic ultrasound osteotome gives a better choice for these cases suffered from osseous nerve root canal stenosis. Ultrasound osteotome is the safest bone cutting tool. It has the property of selective bone-cutting without rotating, bouncing or rolling which can result in entangling the surrounding soft tissue and injury to surrounding nerve tissue [2,3,9,14]. It has been suggested in the literature that ultrasonic osteotome is safer and more accurate and efficient than abrasive drilling [2,3,9,14,27].
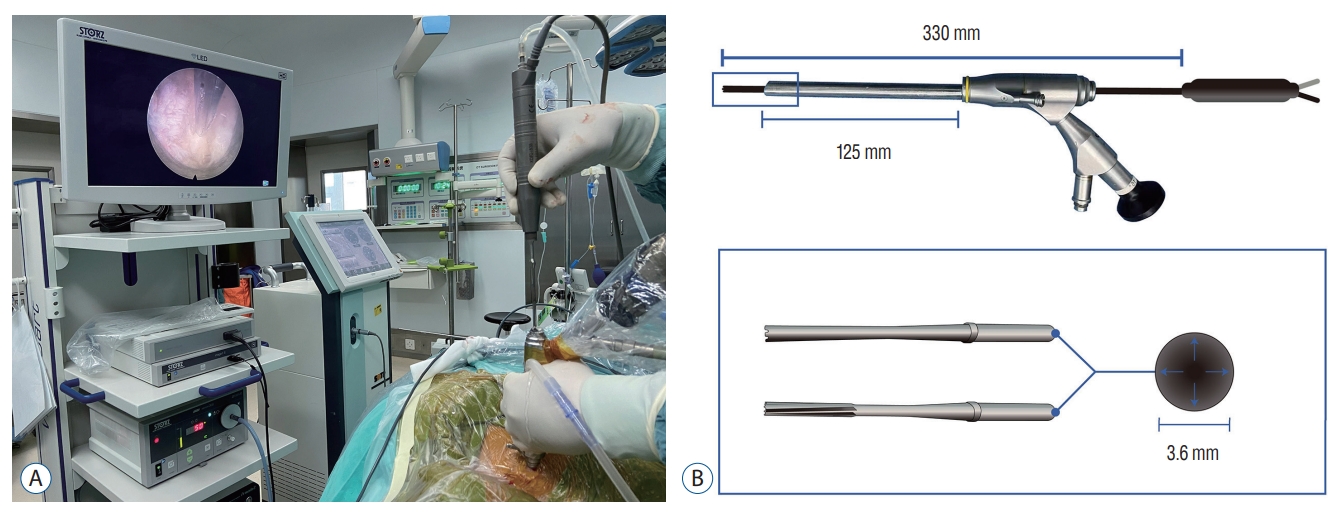
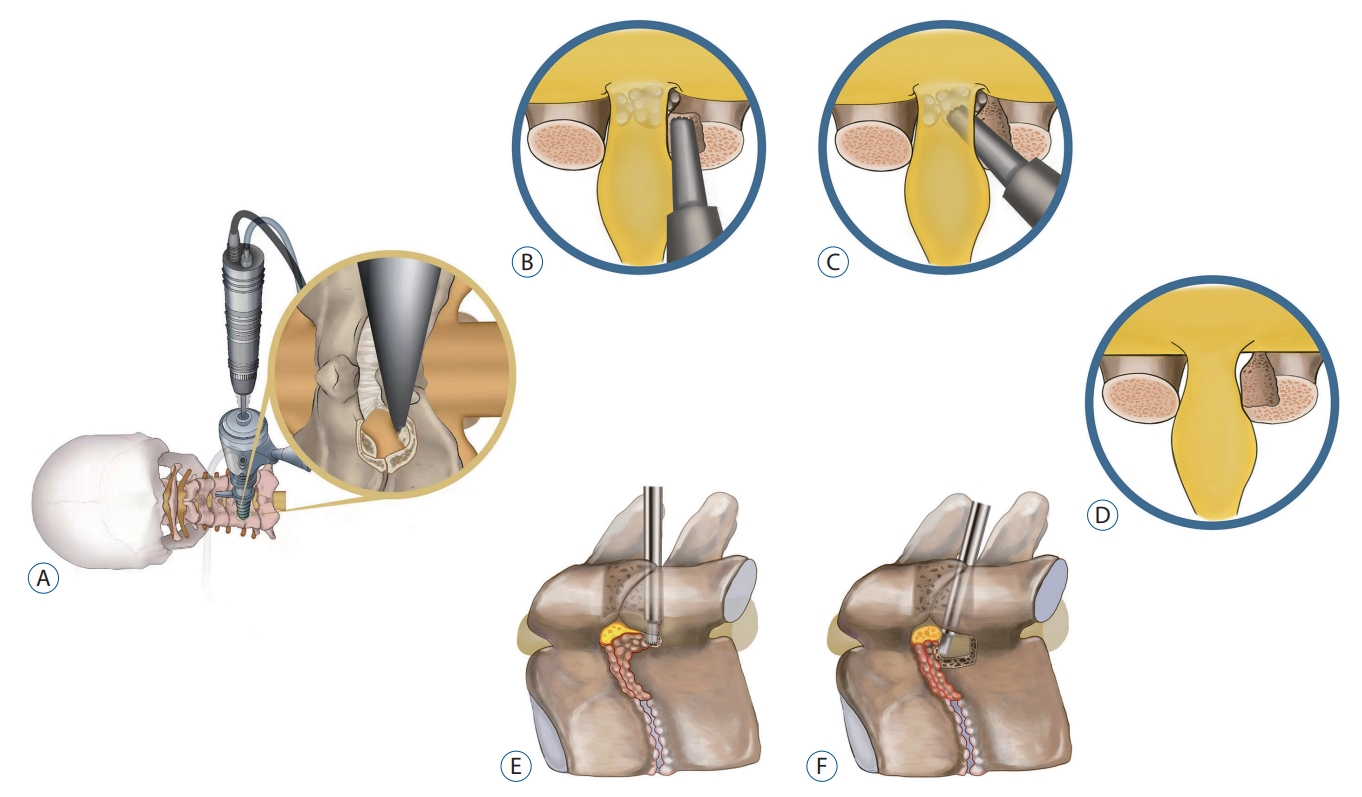
From April 2018 and April 2021, we performed PECF using ultrasonic osteotome in 19 patients with cervical osseous nerve root canal stenosis. To the best of our knowledge, this is the first report about ultrasonic osteotome involving PECF (Fig. 2). The purpose of this report is to investigate the efficacy and safety of the PECF using ultrasonic osteotome for the treatment of cervical osseous foraminal stenosis, focusing on introduction of the advantages of ultrasonic osteotome in partial pediculectomy and ventral osteophyte resection in PECF.
MATERIALS AND METHODS
This study complied with the principles of the Declaration of Helsinki. Patients and their guardians have signed informed consent forms for surgery. The study has been approved by the Ethics Committee of Zhongshan Hospital, Fudan University (Institutional Review Board [IRB] approval number 2021-042), as well as Minhang Hospital, Fudan University (IRB approval number 2021-037-01X).
Patient population
Between April 2018 and April 2021, 19 patients with cervical osseous nerve root canal stenosis in our institutions were enrolled in this prospective clinical study. Among the 19 patients, nine were male, and 10 were female; with a mean age of 57.4 years (range, 42-78); there were two cases (10.5%) of C3-4 lesions, two cases (10.5%) of C4-5, 11 cases (57.9%) of C5-6, and four cases (21.1%) of C6-7 (Table 1). All operations were performed by the same senior author, who has specialized training in spinal neurosurgery and robust experience in full-endoscopic spine surgery.
Inclusion criteria were as follows : 1) single-level CSR, unilateral radiculopathy with arm, neck or shoulder pain consistent with preoperative magnetic resonance imaging (MRI) and computed tomography (CT); preoperative cervical CT reconstruction imaging revealing osseous foraminal stenosis. 2) single-level CSR with unilateral osseous foraminal stenosis who has undergone ACDF surgery. And 3) failure of standard conservative treatment for at least 2 months.
Exclusion criteria were : 1) clear segmental instability or deformities; 2) myelopathy; 3) lateral and medial localization of disc herniation; and 4) more than two-level or bilateral osseous foraminal stenosis.
Endoscopic instruments
The full endoscopic surgical system iLESSYS® Delta (Joimax GmbH, Karlsruhe, Germany) and ultrasonic osteotome device (XD860A; SMTP Technology, Beijing, China) was applied to perform the surgery. The Delta system includes an endoscope, endoscopic sheaths, nucleus pulposus clamp, and laminectomy rongeurs. The radiofrequency probe (Trigger-Flex® Bipolar System; Elliquence LLC, Baldwin, NY, USA) was utilized to control bleeding and ablate.
The ultrasonic osteotome device is made by SMTP Technology Co., Ltd located in Beijing Zhongguancun National Independent innovation demonstration center. The diameter of the ultrasonic osteotome is 3.6 mm, and the length of the ultrasonic osteotome is 330 mm. It can be matched with the spinal endoscope system which has working channel more than 3.6 mm in diameter (Fig. 2B).
Clinical evaluation
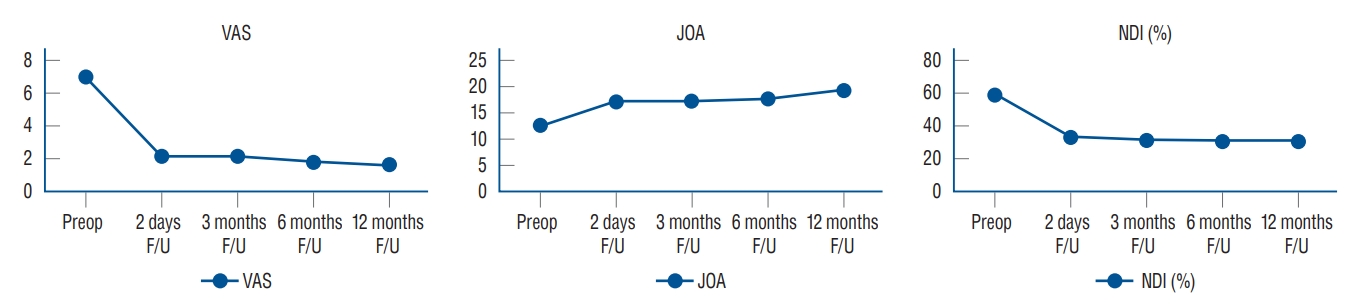
Operative time, hospitalization time, and complications were recorded. Visual analog scale scores for neck and arm pain, Japanese Orthopaedic Association (JOA) scores and Neck disability index (NDI) scores were evaluated preoperatively and on the second day, 3, 6, and 12 months postoperatively. MacNab criteria was used to evaluate surgical effectiveness.
Statistical analysis
SPSS ver. 23.0 (IBM SPSS Statistics, Chicago, IL, USA) was used to study data for statistical analysis. For continuous variables that conform to the normal distribution, the visual analogue score (VAS) score, JOA score and NDI are expressed as mean┬▒standard deviation; the VAS score, JOA score and NDI at different time points were compared using repeated-measures analysis of variance. p<0.05 was considered to be statistically significant.
Surgical procedure
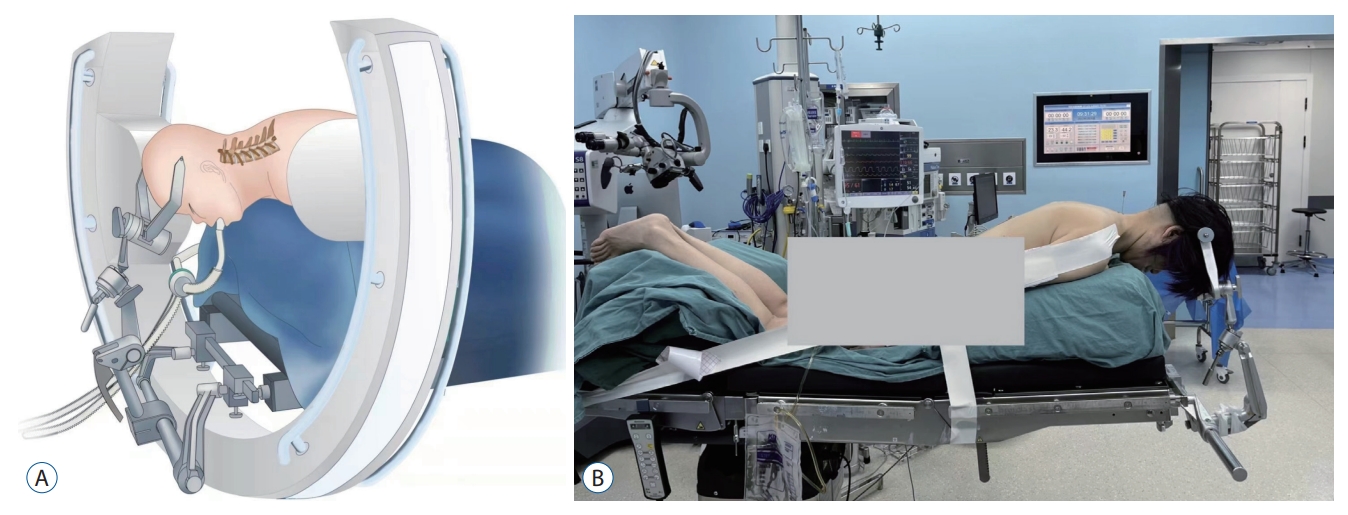
General anesthesia was used for all the patients. The patient was placed in a prone position with head fixed with Mayfield clamp. The neck was slightly flexed, and the shoulders were pulled downward with wide tape for intraoperative lateral fluoroscopy (Fig. 3).
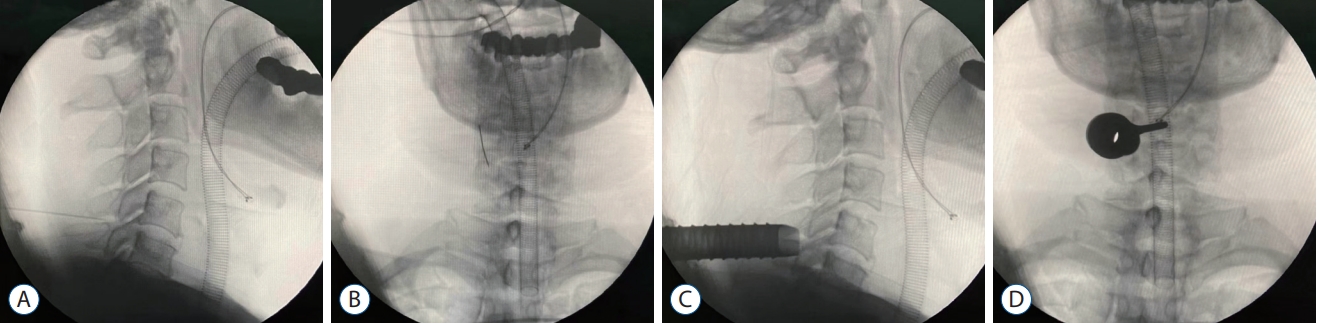
The patient was routinely sterilized and draped. Under fluoroscopic guidance, an 18-gauge spinal needle was introduced to touch the bone, which is lateral facet joint on the lesion side of the target segment (Fig. 4A and B). Then the spinal needle was replaced with a guidewire. A 10-mm stab wound was made centered the guide wire in the skin. The paravertebral muscles and fascia were dilated gradually by soft-tissue-dilators. The dilator could be used to slightly strip the muscles from laminar. Then the 10 mm delta working cannula with oblique mouth was inserted. The final position of working cannula was controlled radiologically in anteroposterior and lateral position (Fig. 4C and D). Finally, the endoscopic surgical system was introduced and all the subsequent steps were performed under constant irrigation with excellent endoscopic visualization.
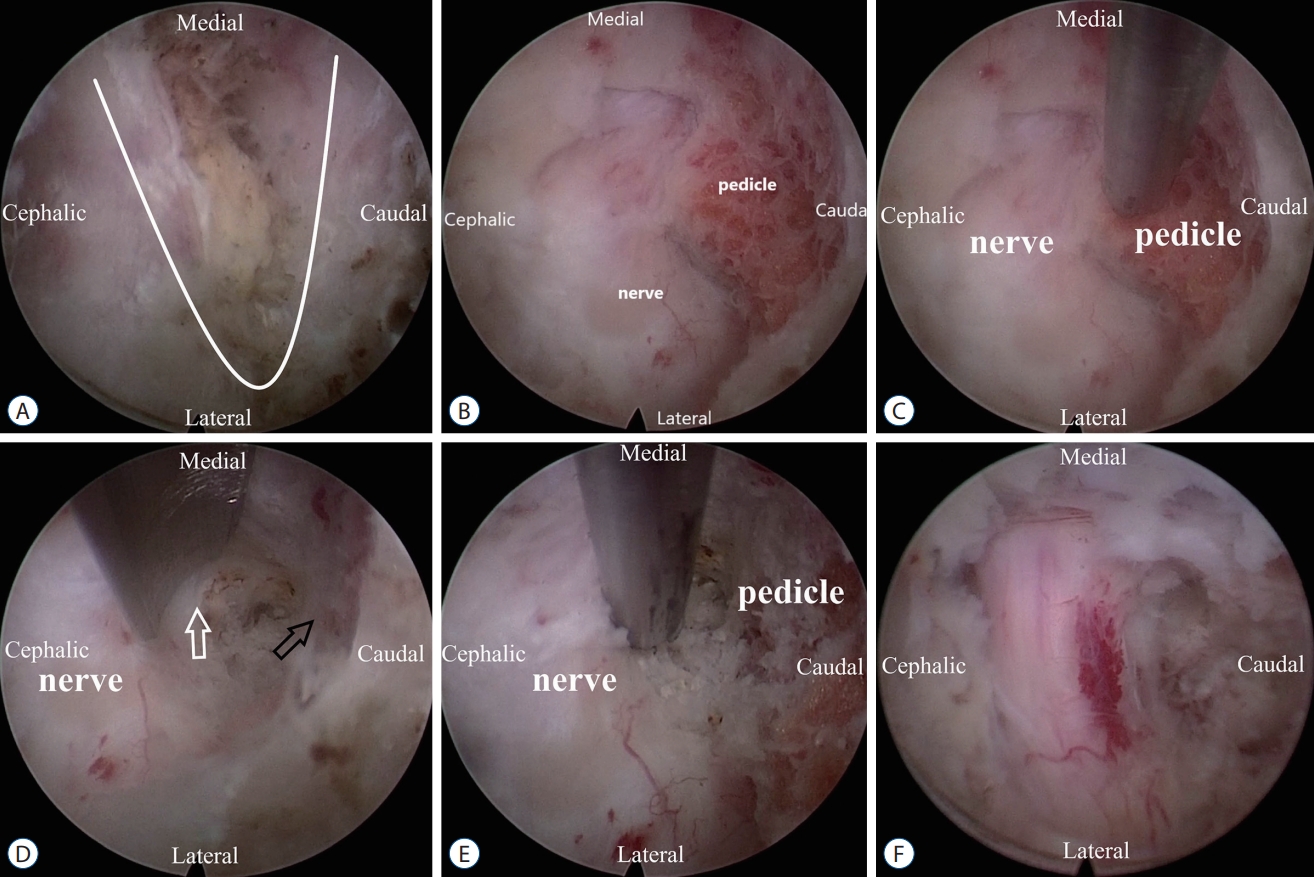
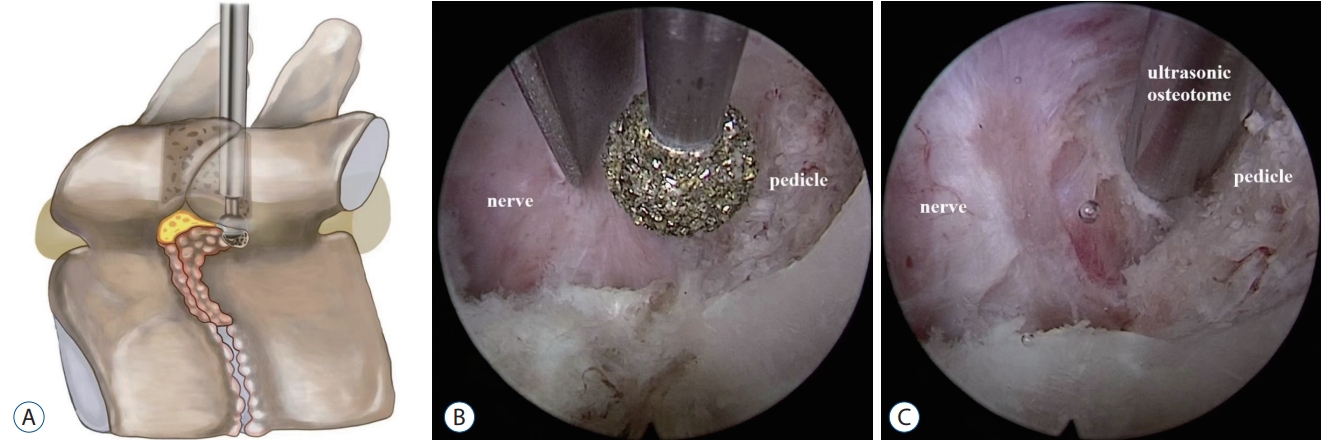
After the soft tissues overlying the facet joint and laminae was cleaned using the tissue forceps and a bipolar radiofrequency probe, the ŌĆ£V-pointŌĆØ structure was identified, which is formed by two adjacent laminae and the affected facet joint (Fig. 5A). The endoscopic ultrasound osteotome was applied to resect bone tissue including partial lamina and medial half of the facet joint. The ligamentum flavum and affected nerve root was identified (Fig. 5B). In this step, the ligamentum flavum was kept in situ to prevent bleeding and protect dura. Endoscopic ultrasound osteotome was continue used to perform partial pediculectomy to enlarge the operation space (Figs. 5C, 6B and E), especially in the condition that the intervertebral height was lost and the distance between the upper and lower pedicle was significantly reduced (Fig. 7B and C). The working cannula was shifted toward the subneural working space (Fig. 5D). The ventral osteophyte could be handled by ultrasonic osteotome without significant neural retraction (Figs. 5E, 6A, C, and F). After the completion of bony decompression, the ligamentum flavum and bands around neural elements were removed. The full decompression was confirmed with free mobilization of the nerve root (Figs. 5F, 6D, and 7D). Then, the endoscopic operation system was removed and the skin was closed with a single stitch. There was no drainage was needed.
RESULTS
Demographic data
The patientŌĆÖs basic information and operative characteristics are summarized in Table 1. The average operative time was 54 minutes (range, 42-70). The average hospital stay was 2.55 days (range, 2-3). Among the 19 patients, there were no surgery-related complications, such as nerve injury, cerebrospinal fluid (CSF) leakage, and wound infection.
Clinical outcomes
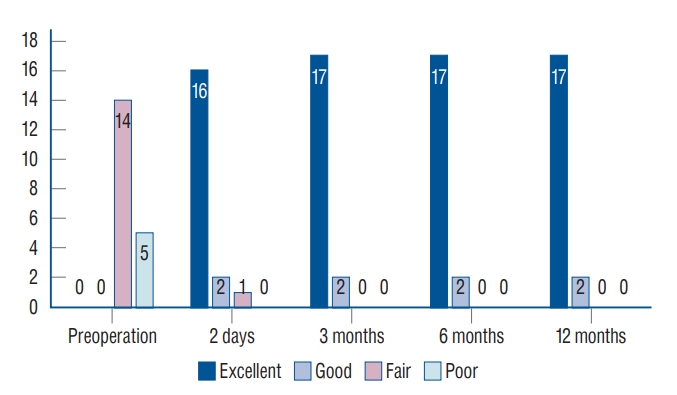
All 19 patients underwent successful surgery and completed the follow-up visits for up to 12 months. As time went by, the change of the VAS score, the JOA and the NDI was shown in Table 2 (F values were 133.003, 67.529, 168.568, respectively; all p<0.001). The differences in the scores before and after surgery were statistically significant (p<0.001; Table 2 and Fig. 8). All 19 patients showed satisfactory effects according to the modified MacNab criteria at the last follow-up visit (Fig. 9).
Postoperative management
The patients were allowed to ambulate with neck brace after 8 hours of bed rest. Symptomatic medication treatments, aiming to eliminate swelling and pain, were routinely applied postoperatively. The patients were instructed in rehabilitation training and followed regularly. In our institution, patients would be advised to wear neck braces for 1 week and participate in normal activities 2 weeks postoperatively.
Perioperative complications
There were no severe surgery-related complications, such as nerve root injury, dura tears, hematoma, CSF leakage, or wound infections were observed. Two cases had transient paresthesia after surgery, which disappeared in 2 to 3 weeks. There were no cases of cervical instability, cervical pedicle fracture and further recurrence at the time of the final follow-up.
Representative cases
Case 1
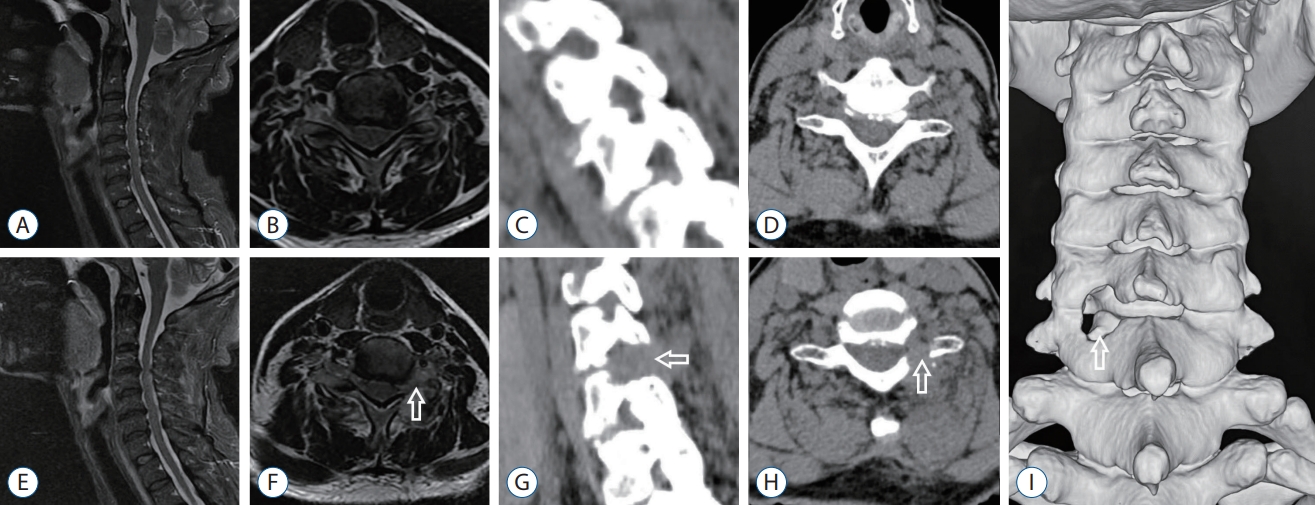
A 62-year-old woman presented with neck, shoulder and left arm pain radiating to the two fingers on the ulnar side about 3 months. She received several conservative treatment measures during the 3 months include medication, physical therapy, Chinese acupuncture and local anesthetic injection. However, her daily activities were seriously disturbed due to the pain had not been controlled effectively. When hospitalization, she rated the pain 9/10 on VAS scale. Preoperative MRI and CT revealed osseous foraminal stenosis at the left side of the C6/7 level. The patient underwent PECF using ultrasonic osteotome to remove part of facet joint, part of pedicle and ventral osteophyte. After the direct and sufficient C7 nerve root decompression, the pain was effectively relieved, with a VAS score of 1/10. Postoperative MRI demonstrated removal of the ventral osseous and decompression of the nerve root. Postoperative CT 3D reconstruction showed the keyhole decompression range, which preserved the facet joint more than 50% (Figs. 5 and 10).
Case 2
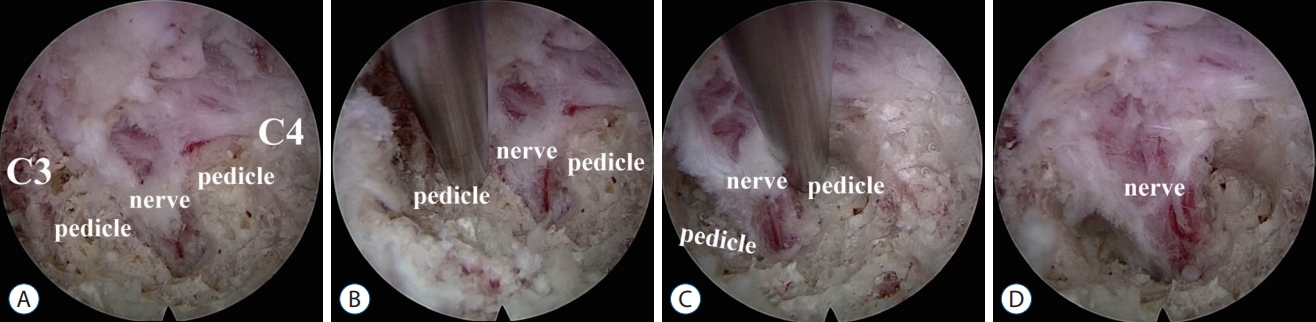
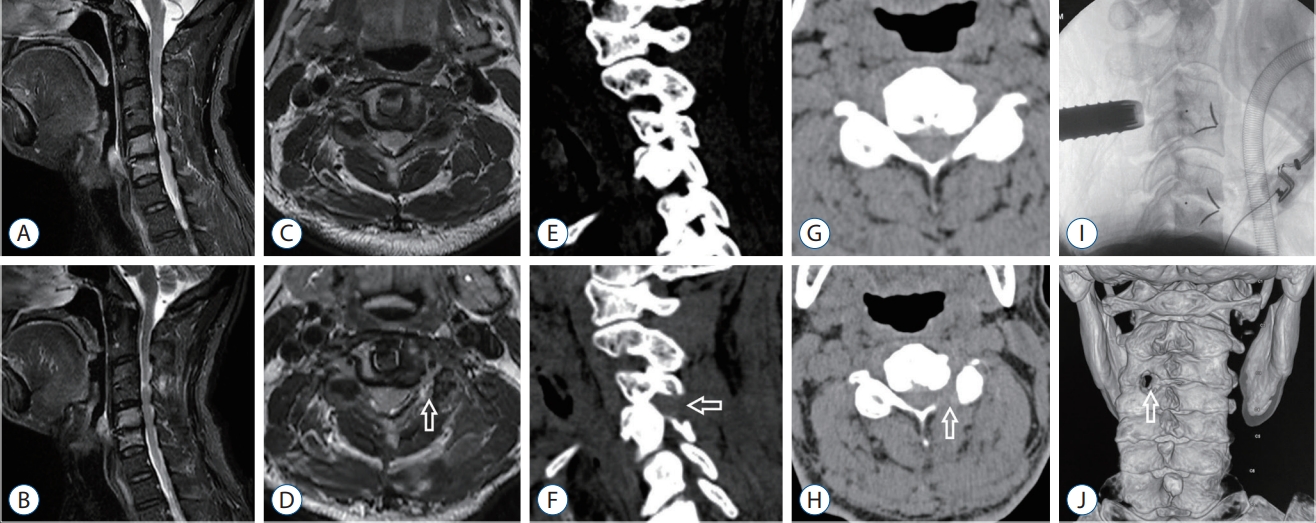
A 67-year-old man presented with left neck and shoulder pain 3 years combined with left arm pain and numbness. He had undergone ACDF surgery two times by other surgeons. One was C3-4 and the other was C5-6. He rated the pain 9/10 on VAS scale and his daily activities were seriously disturbed. Physical examination showed the decreased cervical motive range, left C3-C4 paravertebral tenderness and pain spreading to the left arm. Huffman sign was negative in bilateral hand. Preoperative MRI and CT 3D reconstruction images revealed osseous foraminal stenosis at the left side of the C3/4 level due to cage subside and insufficient decompression. For this complicated case, selective nerve root block (SNRB) to the C4 nerve root was performed to further clarify the diagnosis. The pain decreased more than 70% after SNRB, and the duration was about 4 hours. Hence, the patient underwent PECT using ultrasonic osteotome to remove part of facet joint, part of pedicle and ventral osteophyte at the left C3/4 level. After the procedure, the pain decreased sufficiently, with a VAS score of 2/10. Intraoperative endoscopic photos showed the 360┬░ decompression of C4 nerve root. Postoperative MRI scans and CT 3D reconstruction demonstrated removal of the osseous and decompression of the nerve root (Figs. 7 and 11).
DISCUSSION
Ultrasonic osteotome is a new type of bone-cutting tool based on piezoelectric high-frequency mechanical vibration, which utilizes a back and forth micromotion rather than high-speed rotation to allow precise removal of bone tissue without entangling the surrounding soft tissue [14]. The energy can be preferentially transmitted to bone from the cutting edges of ultrasound osteotome. Hence, it has the property of selective bone-cutting without damaging adjacent soft tissue [2,3,9,14,27]. Ultrasonic osteotome has been applied in open spine surgery for some time, as well as in the fields of skull base surgery, otolaryngology, maxillofacial surgery, etc. [14,27]. In addition, the ultrasonic osteotome is stable and not easy to slip during operation without resulting in accidental injury to the surrounding tissue. At this point, it is superior to high-speed drill, which relies on a high-speed rotating bit to grind bone tissue. However, endoscopic ultrasound osteotome need to be specially designed to be slim and long enough to match the channel requirements of percutaneous endoscopic spine surgery. Fortunately, we now have this excellent weapon, which has been verified in our case series.
In PECF, bone tissues need to be resected may include lamina, facet process, pedicle and uncinate process, which are located on the dorsal, horizontal and ventral sides of nerve elements respectively. In terms of dorsal-located lamina and facet process resection, we believe that the high-speed drill is fully competent in the hands of experienced surgeons [10,12,19,23,24,26]. As for the pedicle and uncinate process, which are horizontal located and ventral located respectively relative to the nerve root and dura sac, it is dangerous to grind the hard bony structure (Fig. 12). Inadvertent slippage of high-speed rotating drill bit and involvement of nerve elements will be a great disaster. Just because of this, the current mainstream is dorsal indirect decompression without ventral bony resection for cervical osseous nerve root canal stenosis, which is a less attractive choice to avoid above risks [12,29].
Thanks to the property of endoscopic ultrasound osteotome, we can securely resect part of the pedicle which is very close to the nerve root without worrying about to damage it (Fig. 6B and E). Partial pediculectomy can provide sufficient space to reach the posterior wall of the vertebral body. We can further remove part of vertebral if necessary to create more space. Partial pediculectomy enable us to have adequate space and get an appropriate angle to the ventral side of nerve root and lateral dura sac through the axillary or shoulder of the root without need of excessive root traction [10,24] (Fig. 6C and F). In our case series, postoperative images demonstrated ventral bony decompression had been achieved successfully in all the patients using ultrasound osteotome. The representative case 2 in this report is difficult to handle. The patient had severe C3-4 osseous foraminal stenosis after ACDF surgery two times because of cage subsiding and unsuccessful decompression (Fig. 7A). The osseous stenosis is 360┬░ surrounding the nerve root. Using ultrasonic osteotome, we achieved 360┬░ decompression of the affected nerve root safely. Moreover, it is worth mentioning there was no dura and nerve root injury associated with bone cutting in our cases. It has been reported in the literature that nerve structures injury occurred in the resection procedure of pedicle and/or ventral bony lesion [10,24,29].
Some scholars may query that the ventral bony lesions do not need to be removed in the treatment to CSR. Oh et al. [17] reported that 12 of 101 CSR patients (11.9%) experienced poor surgical effect who underwent PECF which is indirect dorsal decompression. Among them, seven patients had to undergo anterior revision surgery to remove nerve ventral osteophytes. Tong et al. [22] retrospectively compared the surgical effect of indirect dorsal decompression group and direct ventral bone decompression group in the treatment of CSR caused by osseous intervertebral foramen stenosis. The clinical excellent and good rates were 60.87% in the former and 91.29% in the latter. These experiences indicated that adequate ventral decompression was still necessary. The clinical excellent rates in our series were 90% (17/19), which is corresponded to the reported conclusion. Furthermore, there were no surgery-related complications in our series. There were no cases of cervical instability, cervical pedicle fracture and further recurrence during follow-up.
The main disadvantage of endoscopic ultrasonic osteotome is that the price is too expensive nowadays. The main reason is that there are not many manufacturers of endoscopic ultrasonic osteotome. In addition, endoscopic ultrasonic osteotome with different tip shapes should be designed to meet the needs of different clinical operations. We believe these problems will be solved with the development of science and technology.
Limitations
To the best of our knowledge, this is the first report about endoscopic ultrasonic osteotome involving PECF. The limitation of this article is obvious, which is a prospective observational cohort study without large sample size and long follow-up time enough. However, the purpose of this report is to introduce the feasibility of endoscopic ultrasonic osteotome in partial pediculectomy and ventral osteophyte resection in PECF. We believe that it can be used as a reference for other doctors who are going to employ this technique.