INTRODUCTION
Trigeminal neuralgia (TN) is a painful disease characterized by abrupt unilateral shock-like pain in the dermatome of the trigeminal nerve [38]. Typically, the pain is triggered by sensory stimuli such as a touch, and one or more divisions of the trigeminal nerve can be involved [28]. The pain is usually brief but can recurrently occur. According to the cause, TN can be differentiated into classical TN (type 1 TN) or secondary TN (type II TN) [22,26,28]. Classical TN is commonly caused by compression of the trigeminal nerve by a blood vessel, usually an artery in the cerebellopontine cistern, and leads to morphological and pathophysiological changes in the trigeminal nerve [35]. This is termed a neurovascular conflict with compression [35,36]. Anatomical studies have found that the vulnerable area to the compression of vessels is the transition zone in the trigeminal nerve, where myelination changes from Schwann cell to oligodendroglial cell [36,47]. Secondary TN is dependent on the etiology, such as multiple sclerosis plaques affecting the trigeminal root or space-occupying lesions, including tumors, arteriovenous malformations, or aneurysms [35,40]. Differential diagnosis is important for other types of facial pain, headaches, or dental diseases. Magnetic resonance imaging is an important diagnostic tool to identify the offending vessel and exclude other comorbidities such as tumors or multiple sclerosis [17,18,35].
The beta version of the International Classification of Headache Disorders, 3rd edition (ICHD-3) suggests that the diagnosis of TN can be made when at least three attacks of unilateral facial pain occur fulfilling these criteria : 1) occurring in one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal distribution and 2) pain with at least three of the following four characteristics : a) recurring in paroxysmal attacks lasting from a fraction of a second to 2 minutes; b) severe intensity; c) electric shock-like, shooting, stabbing, or sharp in quality; and d) precipitated by innocuous stimuli to the affected side of the face. No clinically evident neurological deficits or pain that cannot be attributed to another disorder is an important criterion as well for the diagnosis of TN [26].
For the treatment of TN, the first-line treatment is medical therapy with sodium channel blocker anticonvulsants, such as carbamazepine or oxcarbazepine [17,28,35,37]. However, generally, for medically refractory TN, which has failed medical treatment with at least three medications, has the presence of intolerable side effects, or has a relapse of symptoms; more invasive treatment is considered [7,28,35]. For surgical treatment microvascular decompression (MVD) is considered the gold standard in the treatment of TN [4,17,28,59]. However, percutaneous procedures can be a promising alternative for patients who are unable to undergo a surgery.
Various percutaneous treatment techniques for TN have been developed since 1911, when Harris successfully treated TN by percutaneous injection of alcohol into the trigeminal ganglion [3]. In 1914, Hartel described a method for accessing the foramen ovale for percutaneous injections, which is still used in percutaneous techniques today [60]. Percutaneous lesioning electrodes target the trigeminal ganglion by passing through the foramen ovale with the advancement of a cannula [3,28,60]. Percutaneous procedures aim to selectively destroy the afferent A-delta and C pain nerve fibers chemically by glycerol injection, mechanically by balloon compression, or thermally by radiofrequency thermocoagulation, while preserving A-alpha and A-beta sensory nerve fibers [28,35,38]. The reported outcomes of percutaneous procedures are variable, depending on the outcome measurement scale used [3,7,29,59,60].
In this review, we will discuss the technical procedures, outcomes, and side effects of three percutaneous rhizotomy procedures for TN.
GENERAL CONSIDERATIONS FOR PERCUTANEOUS TECHNIQUES
Several factors should be considered when making the right choice for the treatment of TN. MVD has surgical difficulties of which the surgical area is near the brainstem and has a deep narrow operation view while percutaneous procedures only require a cannula puncture. Percutaneous procedures can be better for elderly patients or those with multiple medical comorbidities for whom the surgical risks of MVD would be a burden, or MVD might be suitable for healthier patients who wish to minimize postoperative facial numbness [15,60]. However, MVD is not always ideal, and not every patient with TN has a neurovascular conflict. Indications for percutaneous trigeminal rhizotomy persist when patients experience idiopathic and episodic sharp shooting pain without a neurovascular conflict. The results of percutaneous procedures are not inferior to MVD. In addition, patients’ preference for a less invasive method can influence the procedure they will undergo. Recurrence and failure of the previous procedure can influence the decision to follow the treatment. Therefore, percutaneous techniques still play a role in treating patients with TN and offer several important advantages and efficiency in obtaining immediate pain relief, which is also durable in a less invasive and safe manner [15,60].
RADIOFREQUENCY THERMOCOAGULATION
Radiofrequency lesioning/radiofrequency thermocoagulation (RFT) of the preganglionic trigeminal rootlets was introduced by Sweet and Wepsic [55] in 1974. Since then, modifications in electrode types have allowed for more selective lesioning of the sensory fibers of the nerve and thus decreased the rates of sensory complications [46,57]. RFT can offer immediate pain relief of >90% with a recurrence rate of up to 25% [38].
Surgical technique
RFT is division-selective; preoperatively, patients must be trained to cooperate and localize pain during the procedure; therefore, the patient must remain awake during the procedure. Occasionally, short-acting anesthetic agents, such as propofol, can be used for the induction of sedation. To prevent bradycardia due to the trigeminal depressor response, atropine was administered before the procedure. The patient was positioned supine with slight flexion of the head at 15°. Hartel’s anatomic landmarks were drawn on the ipsilateral face of the patient, inferior to the medial pupil, 3 cm anterior to the external auditory meatus, and 2.5 cm lateral to the lips (Fig. 1). The skin insertion point of the guide cannula was lateral to the lips, with the trajectory guiding towards the other two landmarks. With the help of landmarks and C-arm fluoroscopy, the guide cannula was inserted and advanced along the target trajectory to the foramen ovale (Fig. 2). To prevent violation of the oral cavity and buccal mucosa, the surgeon can direct the cannula with a gloved hand. The electrode penetration should be avoided by placing it 10 mm beyond the clivus because the trochlear and abducens nerves are present there. After confirming the cannula position with C-arm fluoroscopy, the obturator was removed and the electrode was inserted. Test stimulation was performed by asking the patient to localize pain and thereby side effects could be prevented. Alternatively, the patient can be under sedation throughout the surgery, and combination of fluoroscopy and nerve stimulation can be used to verify the appropriate localization. Thermocoagulation was started at the previously tested locations, and lesions were made at a maximum of 0.5 V at 55-80°C for 30 seconds to 2 minutes per cycle. After the patient achieved pain relief, with normal sensory function being conserved, the cannula was removed. The procedure was completed with compression and dressing of the puncture site. The patient remained stable after the procedure and was discharged on the same day.
Outcome
RFT reduces pain by producing mild hypoalgesia, without causing significant sensory deficits in the affected trigeminal divisions. Pain relief outcomes are favorable, with most studies reporting >95% pain resolution [23,29,59,60]. The reported immediate response rate to RFT was 97.6-99%, and the response rate at 6 months of follow-up was 83.3-89.9% [23]. The recurrence rates varied from 38.2% at 1 year to 10% at 6.5 years of follow-up [23]. A large series reported that after 20 years, 41% of the patients remained in pain control [41]. The degree of sensory reduction correlated with pain control and the duration of pain relief [41,60]. In a prospective study of 154 patients, those with more hypoalgesia had lower rates of pain recurrence but higher rates of dysesthesia, whereas patients with mild hypoalgesia had higher rates of pain recurrence but lower rates of dysesthesia [56]. Type I TN is associated with better outcomes after RFT; in contrast, bilateral pain and psychiatric comorbidities are associated with worse outcomes [20,27]. RFT is effective for multiple sclerosis-related type II TN but requires the induction of anesthesia in the affected trigeminal divisions [41]. The advantage of RFT is that it allows for the most selective targeting of the divisions compared to any other percutaneous procedure [27]. Few studies have examined the predictors of outcomes after RFT [51]. In a study by Kosugi et al. [30], outcomes were superior for isolated third-division pain than for second-or multi-division pain.
Complication
Although RFT is durable and has a higher pain control rate than other percutaneous procedures, it is associated with relatively higher rates of side effects [60]. Side effects, such as dysesthesia, corneal anesthesia, and masseter weakness, may occur and seem to be related to the irreversible damage of small, unmyelinated pain fibers in the trigeminal nerve [38,54]. Mild-tomoderate facial numbness is a consequence of RFT, but dysesthesia may also occur [60]. Higher coagulation temperatures for RFT may be related to hypesthesia [15], which lasts for at least 1 month in 3.3% of the patients [27]. There is a 1-20% rate of decreased corneal sensation, with a 1% rate of conjunctivitis [23,29,41,57,60]. Approximately 3-29% of patients experience masseter weakness [60]. Masticatory weakness and diplopia mostly recovered within 6-12 months [60]. Rates of anesthesia dolorosa ranged from 0.6% to 0.8%, which are higher than those for percutaneous balloon compression (PBC) [29,41]. Other complications such as meningitis, hemorrhage, and carotidcavernous fistula formation can occasionally be observed [57,60]. Taha and Tew [57] reported that the use of a curved electrode allowed the creation of more selective lesions and decreased the rates of sensory complications.
GLYCEROL RHIZOTOMY (GR)
The first reported injection of alcohol into the trigeminal nerves was performed by Schloesser in 1904 [46]. Since then, physicians have injected various agents, including chloroform and osmic acid, into the nerve to cause chemoneurolysis [16]. The use of glycerol injection was discovered by chance when using glycerol as a medium to inject tantalum dust into the trigeminal cistern [25]. Although the exact mechanism is unknown, it is thought that glycerol injection causes a rapid rate of change in intracellular osmolarity and results in axonal demyelination and fragmentation, which selectively injures large myelinated fibers [44,60]. GR offers an initial pain relief of >90% and pain relief duration of 3 years in almost 50% of the cases [42,53].
Surgical technique
The procedure is performed under sedation with a shortacting anesthetic agent such as propofol. Atropine can be preadministered to prevent the trigeminal depressor response. A 20-gauge needle is directed using Hartel’s landmarks to access the foramen ovale and is followed by C-arm fluoroscopy to guide and confirm the needle. After accessing Meckel’s cave through the foramen ovale, cerebrospinal fluid often drains from the needle, confirming its position. Contrast-enhanced cisternography or injection of 1 cm3 of air can be used to outline the trigeminal cistern. The patient’s position is then changed to 60° head-up-tilt, and glycerol is injected. The volume of glycerol injected varies from 0.25 to 0.40 mL. Different volumes can be used to target different divisions. For multidivision pain, injection of the full volume treats all divisions. The needle is withdrawn after the glycerol is injected, and the patient is awakened to remain in a sitting position for 2-3 hours so that the glycerol remains in Meckel’s cave. The patient can be discharged on either the same day or the next day.
Outcome
The outcomes of GR vary significantly among the studies. The reported immediate and complete pain relief rates are 53-98% [3,5,14,20,23,42]. Outcomes vary in degrees of postoperative hypoalgesia; one study reported mild-to-moderate hypoalgesia in up to 70% of cases but lasting no more than 3-6 months [60]. GR has a mean pain control duration of 11 months [20]. At the 1-year follow-up, there was a 53-63% rate of pain control [5,6,12]. Recurrence rates were 72% after 54 months in one study [24] and 56.5% after 5 years in another study [23]. Another study reported 18.8% in a 10-year follow-up, and most recurrent cases occurred within the initial 3 years [14]. In a study by North et al. [42], female sex, type I TN, prior effectiveness of carbamazepine, shorter pain duration, and intraoperative cerebrospinal fluid outflow were associated with longer pain-free duration. In another study by Pollock [49], non-constant preoperative facial pain, immediate pain during glycerol injection, and new postoperative trigeminal deficits were related to a chance for better outcomes. Other potential prognostic factors for initial pain relief include postoperative hypoesthesia, pain-free intervals, and high preoperative pain scores [7,48]. Intact preoperative facial sensation and no history of prior procedures have been found to be prognostic factors for durable pain relief [60]. Several early reports suggested that cerebrospinal fluid outflow during the procedure indicates improved outcomes and lower recurrence rates; however, in more recent studies, this was not significant [14,45,60]. Three or more previous GR histories were associated with shorter recurrence times [8]. GR may relieve intermittent pain for type I TN but not the constant pain for type II TN; outcomes are worse for type II TN after GR, with a high recurrence rate of 78-100% within a year [12,20]. Another study reported a 59% recurrence rate at a mean of 17 months [48].
Complication
Postoperative hypoesthesia occurs in 23.3-72% of cases, and, typically, the facial numbness resolves within hours to days after the operation [8,12,14,23,24,60]. With repeated procedures, higher rates of hypoesthesia occur [24]. Similar to other percutaneous treatments, facial numbness is positively correlated with pain relief. Severe hypoalgesia and analgesia are rare, but patients undergoing repeat procedures are at a higher risk [50]. There is a low risk of anesthesia dolorosa ranging from 0% to 5% and masticatory weakness ranging from 0% to 4.1% [60]. The decreased corneal sensation is more common than in balloon compression, which occurs in up to 16% of cases [12,14,41]. There is a possibility of herpes reactivation in one series, presenting in 77% of postoperative cases [21]. Aseptic or bacterial meningitis can occur in 0.12-3% and 1.5-1.7% of cases, respectively [3,8,12,14]. Carotid puncture occurs at a rate of 0.77% [7,8]. Penetration of the buccal mucosa and buccal hematoma can occur at rates of 1.5% and 7%, respectively [7,8]. Hearing loss was reported at a rate of 1.9% [8].
PBC
Mullan and Lichtor [39] first introduced PBC of the trigeminal ganglion in 1983. Inflation of the balloon causes mechanical injury to the trigeminal ganglion and preganglionic rootlets by selectively injuring medium- and large myelinated pain fibers while sparing small fibers, which allows for the preservation of motor and sensory function and, theoretically, the corneal reflex [9]. The advantages of balloon compression are its low cost, simplicity, and being the only percutaneous procedure performed under general anesthesia [33,38]. PBC offers immediate postoperative pain relief ranging from 80% to 90% and a pain-free interval of 2-3 years [6,10,38,58].
Surgical technique
PBC is performed under general anesthesia. Similar to other percutaneous procedures, a trigeminal depressor response can be evoked. However, atropine is only prepared at the bedside but not administered preoperatively because of intraoperative monitoring of trigeminal compression. Thus, in cases of persistent hypotension and bradycardia, careful monitoring is necessary, and a transcutaneous or transesophageal pacemaker should be attached. With a 15° head elevation, Hartel’s landmarks are used in the same manner as RFT. A 14-gauge needle is inserted and advanced along the target trajectory to the foramen ovale. C-arm fluoroscopy is performed to guide the needle. Although not always observed, entering the trigeminal cistern may result in the outflow of cerebrospinal fluid. Proceeding through the foramen ovale can evoke a trigeminal depressor response. A straight guiding stylet is passed through the cannula under direct visualization using C-arm fluoroscopy. In the anteroposterior view, the stylet is heading toward the porus trigeminus, which is approximately 17 mm beyond the foramen ovale. Pointing the stylet towards the center of the porus is thought to treat second-division or multi-division pain, whereas the lateral position is thought to treat third-division pain and medial for first-division pain. When the stylet is placed in the appropriate position, it is then removed, and a 4-F balloon catheter is inserted and passed towards the target position. The balloon is inflated with 0.7-0.75 mL of contrast agent to a target pressure of 1000-1200 mmHg for 60-90 second. C-arm fluoroscopy visualizes the needle and balloon by showing a typical pear or dumbbell shape in the lateral view, which reflects their position within the porus. During balloon compression, the trigeminal depressor response can be observed again, which is an indicator of appropriate compression. After the procedure, the cannula and catheter are removed and light manual compression and dressing are applied to the skin puncture site. The patient can be discharged the same day or the next day.
Outcome
The rate of initial pain relief ranged from 82% to 93.8% [3,5,10,23,33,34,52]. Repeat balloon compression for patients with recurrent TN showed a pain relief range of 83-93.8% [13,43]. At a mean follow-up duration of 4 years, the pain control rate was 69.4% [1]. In another study with a median of 64.8 months of follow-up, 54.5% of patients remained pain-free [43]. Rates of pain recurrence range from 20% to 48%, and one report showed that 90% of patients with a history of surgery showed recurrence rates of 64% [32].
Achieving a typical dumbbell shape or pear shape during balloon compression has been considered a prognostic factor in several studies [3,32]. However, the shape eventually represents the correct positioning of the balloon catheter and an appropriate degree of compression pressure [60].
The time to recurrence also varies widely among studies; at 1 year, there is a 25.4% recurrence rate [41], with recurrence rates ranging from 19.2% to 29.5% after 5 years in another study [60], and a 31.9% recurrence rate at a mean of 10.7 years of follow-up [52]. Time to recurrence may be associated with balloon compression time and the duration and degree of hypoesthesia [13,31]. However, some studies have suggested that a longer compression time does not affect pain relief and only increases the complication rate [38]. Recently, trends have changed to shorter balloon compression times, with <60 seconds being considered adequate for achieving pain relief [32,52,60].
Complication
Common complications of PBC include numbness, masseter weakness, and dysesthesia. Although higher balloon pressure offers greater pain relief, it is reported that higher balloon pressures are also associated with higher rates of complications [10,11,33,62].
Most patients experience postoperative facial numbness, and 4.6-40% of cases have persistent symptoms that typically resolve within 3 months [23,33,34,52]. Approximately 1-11.4% of patients experience dysesthesia, which tends to decrease with less compression times [33,60]. Most cases of dysesthesia are minor and temporary [15]. Trigeminal nerve dysfunction may be related to pressure rate and compression time [1,23,33]. Anesthesia dolorosa has been reported in 0-3.4% of cases [43,52].
Postoperative masseter weakness due to injury in large myelinated fibers is reported in 10-50% of studies [19,23,33,34,52,60]. However, weakness mostly recovers within a few weeks to months [33]. Postoperative corneal anesthesia is reported to occur in 0-3.1% of cases [1,52,60]. The low rates of corneal anesthesia are associated with nerve fiber selectivity of the procedure, which selectively injures medium to large myelinated fibers while preserving small myelinated or unmyelinated fibers [15]. Repeat PBC procedures are associated with a higher rate of masseter weakness and corneal anesthesia [13,43]. Misplacement of the balloon can result in cranial nerve III, IV, and VI injuries, while the abducens nerve is most commonly injured, resulting in diplopia [2,5]. Herpes reactivation can occur after procedures, which is typically mild and does not require prophylactic antiviral therapy [19,60]. Meningitis is rare, ranging from 0% to 5% of cases [60]. Aseptic meningitis is reported in 0.7% of meningitis cases and bacterial meningitis in 0.7-1% [19,34]. Hearing loss occurs in 2.4-6.3% of cases, cheek hematoma in 3.5-6.7%, and pseudoaneurysm in 1% [1,19,23,33,34,52]. PBC has a higher rate of trigeminal depressor response than other percutaneous procedures, and bradycardia and brief hypotension caused by the trigeminal depressor reflex make it less suitable for patients with underlying cardiac disease [7,15,58].
NEW TECHNOLOGY TO FACILITATE THE PROCEDURE - INTRAOPERATIVE COMPUTED TOMOGRAPHY (CT)
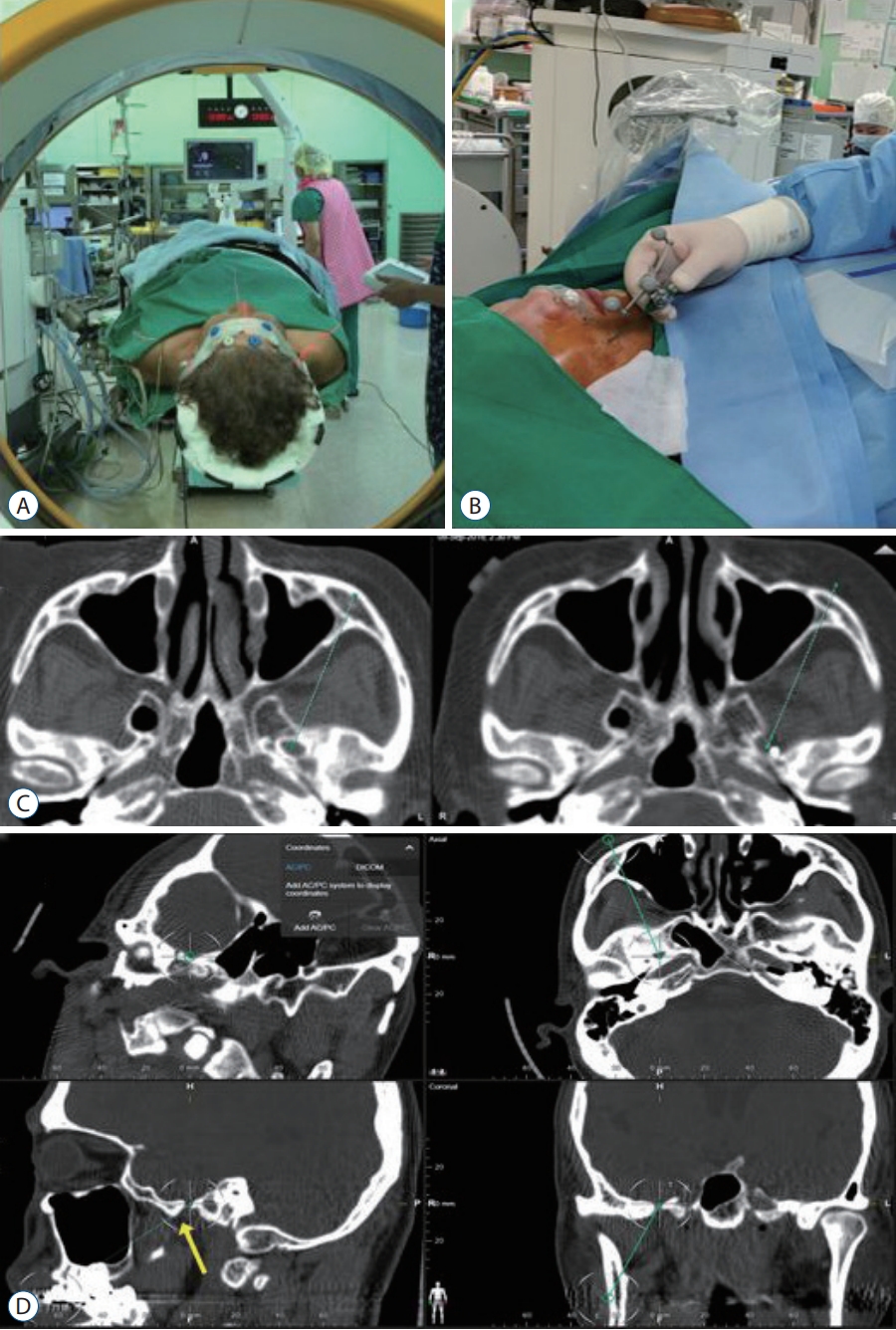
Intraoperative CT with integrated neuronavigation (during percutaneous procedures) has recently been introduced for challenging cases [61]. Patients with a small foramen ovale or a bony spur nearby or with a difficult angle to approach can benefit from this technique. Neuronavigation can guide the trajectory to the foramen ovale, which can reduce the possibility of violating other neurovascular structures and the number of cannulation attempts. If the entrance to the foramen ovale fails by colliding with the bony structure, the tip of the cannula can be detected using intraoperative CT. By redirecting the cannulation based on CT, we could reduce the number of attempts that could be painful to the patient (Fig. 3).
DISCUSSION
The degree of pain in patients with TN is severe. The goal of treatment is to minimize sequelae and improve the quality of life through effective pain reduction. However, to date, no randomized controlled studies have compared these three percutaneous procedures. Only a few retrospective and single-institute studies have compared the outcomes of these procedures. It is difficult to compare the results because the study differs in the patient population, treatment techniques that are operator-dependent, standardization of pain, and measuring the effect of each procedure. All these factors hamper the use of single-modality studies to compare outcomes across treatment modalities. Therefore, it is difficult to determine the superior modality.
Consequently, selection of the percutaneous procedure is often based on the experience and preference of the surgeon. Nevertheless, each technique has advantages and disadvantages (Table 1). Of the three percutaneous procedures, RFT is the most division-selective. However, to localize pain, the patient must be awake. This may be challenging for patients who cannot cooperate during the procedure or tolerate pain. In addition, the more selective the procedure is, the more operatordependent it can be. Therefore, the surgeon’s experience may be needed. Additionally, compared to other percutaneous procedures, higher rates of dolorosa anesthesia have been reported. GR is also division-selective (less than RFT but more than PBC) and can be performed under local anesthesia with or without sedation but requires a change in patient position from supine to sitting. These outcomes seem to be related to the volume of glycerin injected. However, the durability of the procedure is questionable because recurrence rates differ across studies. In PBC, there is a greater risk of a trigeminal depressor response; thus, hypotension and bradycardia can be easily seen. Therefore, patients with cardiovascular diseases are less appropriate. PBC can be pain fiber-selective; therefore, many prefer the use of PBC for isolated first-division pain.
While Hartel’s landmarks, which have been widely used for decades, guarantee safe access to the foramen ovale, risks of percutaneous procedures are still prevalent. The foramen ovale is proximal to critical neurovascular structures in the skull base, especially the internal carotid artery, which can be punctured and lead to pulsatile blood flow through the cannula. Serious injuries can result from unintentional violation of the jugular foramen or inferior orbital fissure. Inappropriate cannula placement can also result in intracranial hemorrhage. The trigeminal depressor response is also a cautious response that can lead to bradycardia, which requires atropine, or in serious cases, can lead to asystole. Although all three of the percutaneous therapies are considered safe and associated with low mortality rates, there have been reports of intraoperative deaths during the procedures.
MVD is considered the first-line treatment of choice for young, healthy patients; however, its role in percutaneous rhizotomy remains unclear. Percutaneous procedures offer immediate pain relief in over 80% of cases, which can last 3 years or more. There was a shorter recovery time and fewer surgical complications. This makes it more suitable for the elderly or for patients with comorbidities. Although recurrence rates exist, percutaneous procedures are repeatable. After several repeat procedures, if pain reduction is unsatisfactory, MVD surgery can still be performed. This is less complicated than revision or repeated MVD surgeries. In addition, for people who try to avoid surgery for cultural or cosmetic reasons, such as in Korea, percutaneous procedures may be a preferable option. Therefore, percutaneous rhizotomy offers many advantages and can be considered a treatment choice.