INTRODUCTION
Syphilis is a complex systemic illness with protean clinical manifestations caused by a spirochete, Treponema pallidum. The clinical course of syphilis is classically divided into the following phases : incubation period, primary syphilis, secondary syphilis, latent syphilis, and tertiary syphilis. During tertiary syphilis, relapse of secondary syphilis in a human immunodeficiency virus (HIV)-negative person can occur up to four years after contact.
The central nervous system (CNS) may be involved at any stage of syphilis infection in about 5% to 10% of untreated patients10). CNS involvement in syphilis patients is classified into four syndromes : syphilitic meningitis, meningovascular syphilis, and parenchymatous and gummatous neurosyphilis. Differentiation from a brain mass in HIV-negative patients with syphilis is a challenge to clinicians1,7,12,18,22). Herein, we report an unusual case of cerebral syphilitic gumma mimicking a brain tumor with the relapse of secondary syphilis in a HIV-negative patient that was successfully controlled by administration of ceftriaxone.
CASE REPORT
A 59-year-old woman was admitted to the emergency department with a 20-day history of speech disturbance. She had a medical history of diabetes mellitus and hypertension, controlled well with medication at a local clinic.
Vital signs at admission were stable. She was alert but had cognitive disturbance (Glasgow Coma Scale 15 and Mini-Mental Status Examination 16/30) and dysarthria. Both pupils showed normal light reflex. There were no abnormal neurological findings for muscle strength and deep tendon reflexes in the extremities.
Computed tomography (CT) scanning of the brain revealed a mass-like lesion at the left frontal lobe and severe cerebral swelling. Brain magnetic resonance imaging (MRI) revealed an irregular enhancing mass with central necrosis that measured 2.8×2.7×2.6 cm in size (Fig. 1A). There was severe cerebral edema around the enhancing mass (Fig. 1B). The mass was adjacent to the enhanced dura in the left frontal lobe (Fig. 1C).
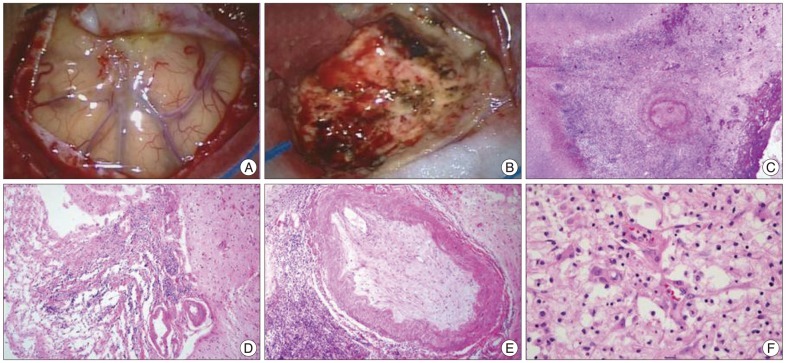
Malignant brain tumors including glioblastoma, metastatic brain tumor or primary CNS lymphoma were suspected with the need to rule out inflammatory conditions. To confirm the diagnosis, the mass was surgically resected with frontal craniotomy. On intraoperative findings, the mass was severely adhered to the dura. It was yellow in color and had a hard consistency (Fig. 2A, B). En bloc resection was performed and the intra-axial mass was completely removed. During the first admission, cerebrospinal fluid (CSF) examination was not performed, because lumbar puncture is contraindicated in the presence of increased intracranial pressure. On histopathological examination, the mass was first diagnosed as chronic inflammation originating from an unknown cause. Without any postoperative complications, she fully recovered from the cognitive defects and speech disturbance. She was discharged from the hospital 14 days after operation.
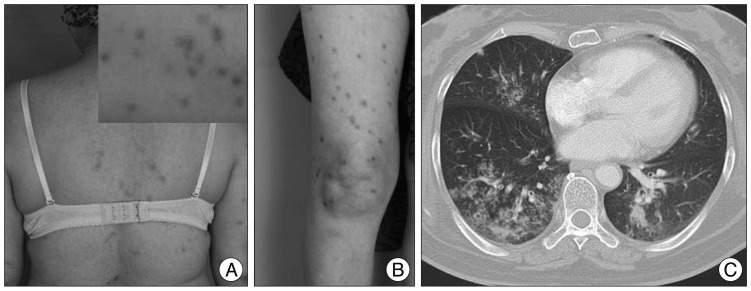
However, she was readmitted for high fever to the Department of Infectious Diseases 2 months after discharge. She had experienced non-itchy erythematous papules and macules over her whole body for three days (Fig. 3A, B). She had a history of sex with a partner who had multiple sex partners two years prior. She had an episode of primary syphilis at that time which was spontaneously resolved without any treatment. On admission, her initial vital signs were a body temperature of 39.5℃, blood pressure of 100/70 mm Hg, pulse rate of 91 beats/minute and respiratory rate of 22 times/minute. Physical examination revealed no generalized lymphadenopathy. On follow-up brain MRI, there was no enhancing mass lesion or severe edema at the cerebral parenchyma (Fig. 1D-F). Chest CT scans revealed an infiltration with interstitial pattern on the right lower lobe of the lung without respiratory symptoms (Fig. 3C). Results of a complete set of blood tests were as follows : white blood cell (WBC) count, 8200/µL, erythrocyte sedimentation rate, 42/mm3, and C-reactive protein, 187 mg/dL. Repeated blood and sputum cultures were negative. Serum mycoplasma antibody testing, including a follow-up test, were also negative. At that time, her serum Venereal Disease Research Laboratory (VDRL) titer was 1 : 16, and fluorescent treponemal antibody absorbed (FTA-ABS) test IgM and IgG were reactive. Histopathological examination of the skin tissue revealed heavy lymphoplasmacytic infiltration consistent with lymphomatoid papulosis. Analysis of the cerebrospinal fluid yielded the following findings : 0 white cells/dL, 1 erythrocyte/mm2, glucose level of 74 mg/dL, protein level of 16.8 mg/dL, negative VDRL test, and negative T. pallidum polymerase chain reaction (PCR) test. However, FTA-ABS IgG in the CSF was reactive. Cardiovascular involvement was not noted with chest CT scans and transthoracic echocardiography. Ophthalmic fundoscopic examination also revealed no abnormal findings. Histopathological reassessment of the previous brain tissue revealed intraluminal obliteration of a large blood vessel just below the meninges, suggesting endarteritis (Fig. 2C). Spirochetes were not identified in this tissue by Warthin-Starry stain. Necrotic tissue in the neighboring brain parenchyma was also seen (Fig. 2D). Around the occluded vessel, parenchymal infiltration of lymphocytes and plasma cells was found (Fig. 2E, F). Other immunohistochemical examinations were negative for the possibility of malignant lymphoma, glioma and inflammatory pseudotumor.
The patient was finally diagnosed with cerebral gumma accompanied by probable pulmonary involvement in tertiary syphilis concomitant with relapse of secondary syphilis, on the evidence of the histopathological findings and positive FTA-ABS IgG in the serum and the CSF. Based on this diagnosis, ceftriaxone was intravenously administrated at a daily dose of 2 g for 14 days. Thereafter, the fever and rash subsided in two days, and an infiltration with interstitial pattern on subsequent chest X-ray showed marked improvement in three days. On April 9, 2012, her follow-up VDRL titer was 1 : 4. Her symptoms associated with syphilis fully resolved without relapse and she was doing well fifteen months after hospital discharge.
DISCUSSION
This is a rare case of cerebral syphilitic gumma with relapse of secondary syphilis in a HIV-negative patient that was successfully controlled by administration of ceftriaxone. Since she had not been treated for primary syphilis two years prior, clinical manifestations of tertiary syphilis presented as neurosyphilis and probable lung involvement.
Neurosyphilis can occur 1 to 25 years following syphilis infection and has various clinical manifestations4). Cerebral syphilitic gumma, first described by Botalli in 1563, is a rare manifestation, typically of tertiary syphilis17). As the present case illustrates, cerebral gummas typically arise from the dura and pia mater over the cerebral convexity or at the base of the brain and produce symptoms similar to those of other intracranial tumors1,7,12,13,18,22). Differential diagnosis for cerebral syphilitic gumma should be performed for other cerebral nervous system diseases including toxoplasmosis, lymphoma, bacterial and fungal infections. All of them are rare, but more common in HIV-positive patients compared with HIV-negative patients3). Syphilitic gumma has been described as a circumscribed mass of granulation tissue that results from localized inflammation as an excessive response of the cell-mediated immune system that manifests as the invasion of lymphocytes and plasma cells. Spirochetes seem to be rarely found in cerebral syphilitic gumma2,19). In the previous study, among the 156 cases with cerebral syphilitic gummas, T. pallidum was found on the histopathologic staining of only one case (0.6%)8). PCR for T. pallidum could be useful for definitive diagnosis in cases where diagnosis is difficult11). In our case, however, no spirochetes were observed on Warthin-Starry staining and her CSF was PCR-negative for T. pallidum, whereas VDRL titer was 1 : 16, and FTA-ABS test IgM and IgG were reactive. Therefore, we suggest that definitive diagnosis for cerebral syphilitic gumma should be examined serologic test for syphilis as well as histopathologic staining and PCR for T. pallidum.
At the time of presentation, our patient's CSF VDRL and pleocytosis were negative, while her serum nontreponemal test for syphilis and FTA-ABS in serum and CSF were positive. Routine laboratory CSF tests will fail to identify some patients with CNS invasion, as in our patient's case. A positive CSF VDRL test is highly specific for active neurosyphilis, but the test is negative in about half of neurosyphilis patients8,16). Even so, the serum VDRL test reportedly is negative in 30% to 50% of all cases with neurosyphilis21). Furthermore, a previous study reported that CSF pleocytosis, defined as >5 WBCs/µL in patients with neurosyphilis was seen in 40% of cases, regardless of the syphilis stage14). Finally, in HIV or non-HIV patients, a normal CSF does not exclude neurosyphilis.
The first choice treatment for tertiary syphilis is penicillin. There are very limited alternatives for the treatment of neurosyphilis. Ceftriaxone is a potential alternative to penicillin G for the treatment of neurosyphilis5,9,14,15,19,20). It is active against T. pallidum, penetrates CSF well, and has a long half-life that enables it to be given once daily. Our patient fully recovered from her symptoms associated with syphilis without relapse for seven months after the administration of ceftriaxone.
During the course of syphilis in our case, the relevance to syphilis of the lung parenchymal lesions was uncertain because the pathological examination was not confirmed. Acquired syphilis of the lung is a rare condition with variable diagnostic criteria6). However, in our patient, the diagnosis of probable pulmonary syphilis was made based on the fact that the radiologically-detected lesion disappeared under anti-syphilitic treatment for a very short period of time, in conjunction with the absence of respiratory symptoms and leukocytosis and the repeatedly negative sputum for tubercle bacilli or bacteria before antibiotic treatment.
CONCLUSION
In conclusion, this patient was treated with ceftriaxone after appropriate diagnosis through the surgical intervention, and completely recovered on follow-up at fifteen months. Our case report suggests that cerebral syphilitic gumma should be considered among HIV-negative patients with space-occupying lesions of the brain and tertiary syphilis, although the patient's CSF VDRL and pleocytosis were negative. Clinical suspicion and diagnosis of syphilitic gumma by physicians are vital.