Ultrasound Diagnosis of Double Crush Syndrome of the Ulnar Nerve by the Anconeus Epitrochlearis and a Ganglion
Article information
Abstract
Double compression of the ulnar nerve, including Guyon's canal syndrome associated with cubital tunnel syndrome caused by the anconeus epitrochlearis muscle, is a very rare condition. We present a case of double crush syndrome of the ulnar nerve at the wrist and elbow in a 55-year-old man, as well as a brief review of the literature. Although electrodiagnostic findings were consistent with an ulnar nerve lesion only at the elbow, ultrasonography revealed a ganglion compressing the ulnar nerve at the hypothenar area and the anconeus epitrochlearis muscle lying in the cubital tunnel. Careful physical examination and ultrasound assessment of the elbow and wrist confirmed the clinical diagnosis prior to surgery.
INTRODUCTION
Upton and McComas first reported double crush syndrome in 1973, postulating that proximal compression could render the distal nerve more susceptible to a second compression14). In clinical practice, we often observe cervical radiculopathy and carpal tunnel syndrome occurring together in what is known as double crush syndrome41112).
Double compression of the ulnar nerve at the elbow and wrist is a very rare condition, however. In the present study, although electrophysiologic findings were consistent with an ulnar nerve lesion around the elbow, ultrasonographic findings showed that the anconeus epitrochlearis muscle lay in the cubital tunnel compressing the ulnar nerve, and that a ganglion cyst had compressed the motor branch of the ulnar nerve around the wrist. Awareness of the double crush syndrome of the ulnar nerve by preoperative diagnostic ultrasonography can improve the accuracy of the clinical diagnosis and prevent possible operative complications.
CASE REPORT
A 55-year-old man presented with a 3-month history of a tingling sensation and weakness in the right hand. He also reported tenderness in the hypothenar eminence. A neurologic examination revealed weakness in the abductor digiti minimi and first dorsal interosseous muscles, whereas the right forearm and arm muscles were strong. A slightly decreased sensation was noted in the fourth and fifth fingers of the right hand. The Tinel sign was present over the elbow.
In the electrodiagnostic examination, nerve conduction studies were performed on bilateral upper limbs, and needle electromyography was performed on the right upper limb. The ulnar compound muscle action potential amplitude was low, and a decrease in conduction velocity over the elbow focal lesion was observed by the inching technique. The right ulnar sensory nerve action potential (SNAP) was normal, but the dorsal ulnar cutaneous SNAP amplitude decreased slightly, compared with the left side. Electromyography revealed spontaneous activity in the first dorsal interosseous muscle, whereas the flexor carpi ulnaris, the other non-ulnar innervated right arm, and hand muscles were normal. Electrophysiologic findings were consistent with an ulnar nerve lesion around the elbow; however, ultrasonographic findings showed that the anconeus epitrochlearis muscle lay between the medial epicondyle and olecranon in a close proximity with a swollen ulnar nerve around the elbow (Fig. 1A), and that a hypoechoic ganglion cyst had displaced the ulnar artery and compressed the ulnar nerve around the wrist (Fig. 1B). The cross-sectional area of the ulnar nerve was 0.083 cm2 at the elbow with a hypoechoic appearance, and 0.087 cm2 at the wrist.
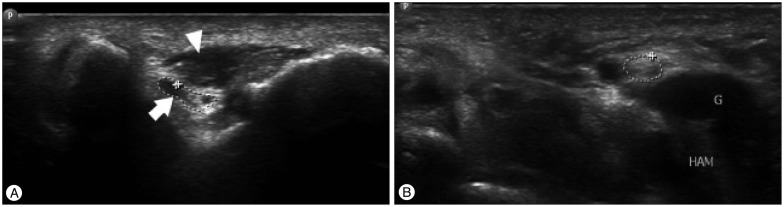
Ultrasonographic findings, revealing (A) the anconeus epitrochlearis muscle (arrowhead) in close proximity to a swollen ulnar nerve (arrow), and (B) a hypoechoic ganglion cyst (G) and ulnar nerve (circle) between the hamate hook (HAM) and pisiform.
During surgery, the anconeus epitrochlearis muscle (Fig. 2A), extending from the medial epicondyle to the olecranon, was found to be compressing the ulnar nerve at the elbow level. The muscle was tight in flexion, and it significantly compressed the ulnar nerve. The aberrant muscle and flexor retinaculum were split longitudinally, and an anterior subfascial transposition of the ulnar nerve was performed. There was a 2.5×2.0-cm, welldefined, encapsulated, cystic mass compressing the motor branch of the ulnar nerve at the wrist (Fig. 2B). The mass was excised, and histopathology confirmed a ganglion. Symptoms improved immediately after surgery, and the patient was symptom free 1 year later.
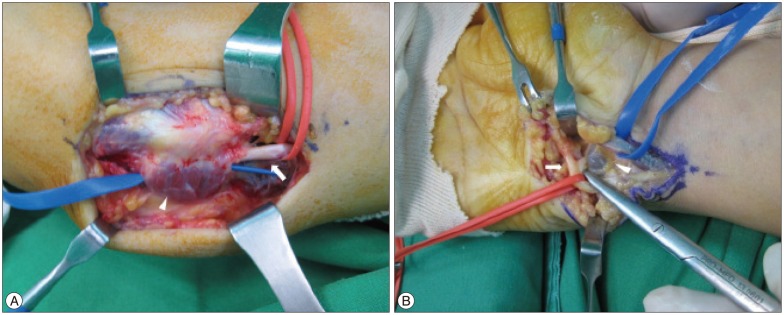
Operative findings, showing (A) the anconeus epitrochlearis muscle (arrowhead) compressing the ulnar nerve (arrow), and (B) a ganglion (arrowhead) compressing the ulnar nerve (arrow).
DISCUSSION
The term "double crush" is appropriate in cases in which a nerve is compressed at 2 separate levels. Multiple compressions can produce vague, nonspecific, or atypical symptoms. The diagnosis and treatment of variable compression at multiple levels is difficult, as multiple compressions along a nerve have a cumulative effect on both antegrade and retrograde conduction12). Double compression of a peripheral nerve is not rare in medical practice. Other researchers have reported series of patients showing the frequent association of proximal and distal nerve compression syndrome, including carpal tunnel syndrome, associated with cervical radiculopathy or brachial plexus compression411).
Double compression of the ulnar nerve is a very rare condition, however. The most important finding of the present study is that the double crush syndrome occurred in the ulnar nerve, including Guyon's canal syndrome associated with cubital tunnel syndrome caused by the anconeus epitrochlearis muscle. Furthermore, this study demonstrated that double crush syndrome cannot be fully diagnosed by electrodiagnostic findings. To the best of our knowledge, there is only 1 report in the literature on ulnar nerve neuropathy along the elbow and wrist segments10); however, the ulnar nerve neuropathy of the elbow was not caused by the anconeus epitrochlearis muscle in that case.
Ulnar nerve compression in the cubital tunnel can have different causes, including the arcade of Struthers, medial intermuscular septum, cubital tunnel retinaculum, humeroulnar aponeurotic arcade, ligament of Osborne, and an anatomic elbow deformity7). In the present report, compression neuropathy of the ulnar nerve at the elbow was caused by the anconeus epitrochlearis muscle. The anconeus epitrochlearis muscle was first described by Wood16) in 1868 as an accessory muscle of the medial elbow that originates from the medial epicondyle of the humerus and insets onto the olecranon process of the ulna. The prevalence of an anconeus epitrochlearis muscle is 4–34% in cadaver studies5). Although it is rarely seen in clinical practice, ulnar nerve compression due to the anconeus epitrochlearis muscle is reported to range from 5% to 16% in the operative series391315).
In the present report, the electrodiagnostic findings of our patient were compatible with ulnar nerve neuropathy around the elbow. However, the patient presented with symptoms of ulnar nerve neuropathy around the elbow and tenderness in the hypothenar area. Ultrasonography revealed anatomic changes, showing that the Guyon's canal syndrome was caused by a ganglion cyst and that the cubital tunnel syndrome was caused by the anconeus epitrochlearis muscle. Although electrodiagnostic studies are the main tools for localizing and assessing nerve injuries, they do not reveal the exact location, intensity, or cause of the lesions, nor do they provide spatial information on the nerve and the surrounding structures1). Flak er al.4) proposed that evaluation of double crush syndrome requires both structural and functional diagnosis of the peripheral nerve by imaging studies and electrophysiologic examination. Indeed, if physical examination had not been carefully performed, we could not have identified double crush syndrome of the ulnar nerve. Therefore, imaging studies may play an important role as an additional accurate diagnostic test.
Ultrasonography is a useful diagnostic tool when the results of electrodiagnostic studies are unclear, such as clinical ulnar neuropathy around the elbow17) or carpal tunnel syndrome68). Sensitivity increases when ultrasonography is added to the electrodiagnostic test with ulnar neuropathy around the elbow2). Ultrasonography can complement the electrodiagnostic examination, and it is readily available, painless, inexpensive, and does not involve radiation exposure. Therefore, we emphasize that double crush syndrome of the ulnar nerve may be diagnosed by careful physical examination, electrodiagnostic studies, and ultrasonography.
In summary, we describe a case of double crush syndrome of the ulnar nerve, including Guyon's canal syndrome associated with cubital tunnel syndrome caused by the anconeus epitrochlearis muscle, which has not been reported before. Careful physical examination and awareness of the double crush syndrome of the ulnar nerve with the use of preoperative diagnostic ultrasonography can improve the accuracy of the clinical diagnosis and prevent possible operative complications.