Minimally Invasive Suturectomy and Postoperative Helmet Therapy : Advantages and Limitations
Article information
Abstract
Various operative techniques are available for the treatment of craniosynostosis. The patient's age at presentation is one of the most important factors in the determination of the surgical modality. Minimally invasive suturectomy and postoperative helmet therapy may be performed for relatively young infants, whose age is younger than 6 months. It relies upon the potential for rapid brain growth in this age group. Its minimal invasiveness is also advantageous. In this article, we review the advantages and limitations of minimally invasive suturectomy followed by helmet therapy for the treatment of craniosynostosis.
INTRODUCTION
Most infants with craniosynostosis require surgery for its correction. For the past few decades, various surgical methods have been proposed for the treatment of craniosynostosis, from open strip craniectomy to extensive cranial vault remodeling316313538). New techniques have also been applied to the surgical treatment of craniosynostosis such as distraction devices, absorbable plates and endoscopes2462136).
Open strip craniectomy was first performed in 1890 for the treatment of microcephaly22), and it has been used for the treatment of craniosynostosis since 19278). Then, it was widely used to release fused sutures and to correct head contour in craniosynostosis. However, advancements in open strip craniectomy have led to arguments against its use due to dissatisfying and inconsistent esthetic outcomes. The late timing of surgery, the incomplete release of the involved sutures and an insufficient maintenance of this release are considered to be the causes of these problems35).
With the development of intraoperative management and anesthesia in pediatric patients, more extensive surgery such as extensive cranial vault remodeling became possible. Extensive cranial vault remodeling methods have enabled effective cranial volume expansion and cephalic index (CI) correction via the removal and division of the skull bones into many parts to reshape bony contours, followed by rigid fixation11). These approaches became popular conventional methods for treating craniosynostosis, replacing open strip suturectomy2526). However, extensive cranial vault remodeling has also raised concerns among many surgeons due to the potential for blood loss and the required operation time, even though efforts to reduce the need for blood transfusion have been made379101720). Aggravation of the deformation while patients age sufficiently to endure this extensive operation is another problem1429). The necessity of stable fixation of the skull also restricts the use of extensive cranial remodeling to relatively early ages.
These concerns related to extensive cranial vault remodeling have raised a need for surgical methods with minimal invasiveness. Minimally invasive suturectomy is one method that began to appear in tandem with this concept. This method reappeared with modifications of the previous open strip suturectomy in 1998, from Jimenez and Barone15). They reported their experiences of endoscopic suturectomy for sagittal craniosynostosis. Using an endoscope during dissection made this procedure minimally invasive, and the use of an orthotic helmet applied after the operation assisted in reshaping the head contour. Suturectomy itself is not different from open strip craniectomy, but its minimal invasiveness enabled the operation to be used with early infants. Comparable esthetic outcomes were also reported in the literature, and this technique was acceptable to many surgeons121415273440). Smaller incisions, less blood loss and shorter operative times and lengths of hospital stay were achieved with minimally invasive suturectomy1319313440). Minimally invasive suturectomy has been performed since 2011 at our institution. In our experience, the magnification and illumination of the endoscope can be substituted with a loupe magnifier and a suction tip with a fiber optic cable and light source to visualize the operative field. Therefore, we will use the term 'minimally invasive suturectomy' and 'endoscopic-assisted suturectomy' interchangeably, although two terms do not mean precisely the same thing.
PATIENT SELECTION AND PREPARATION FOR THE TREATMENT
Patient age is the most important factor in deciding whether a surgical candidate is appropriate for minimally invasive suturectomy. Because taking advantage of a period of rapid brain growth phase as much as possible is the main point in this procedure, patients under the age of 6 months are good surgical candidates, and ages closer to 3 months of age are more ideal. Patients between 6 to 9 months of age may also be considered as surgical candidates for minimally invasive suturectomy if the deformity is minimal16).
The diagnosis of craniosynostosis is made by clinical examination of the deformed head shape and confirmed by plain-skull radiographs and craniofacial computed tomography (CT) scans with 3-dimensional (3D) reconstruction. Gross photographs and anthropometric data are required to obtain preoperative morphologic information and to determine trends for postoperative correction.
SURGICAL TECHNIQUES
Surgical techniques for minimally invasive suturectomy in previous articles are all similar in that they were all aim to release a fused suture with small exposure12152731). Procedures in our center are both similar and different from previous articles introduced as follows.
In sagittal craniosynostosis, the patient is prepared with the head extended in a prone position. Skin preparation is done with povidone-iodine. Two transverse incisions are made of 3–4 cm length at 1 cm behind the anterior fontanelle and 1 cm in front of the lambdoid suture. An additional incision may be needed between the two sites to manipulate safely in a patient with a longer head. A subperiosteal dissection is made along the desired craniectomy site. Burr holes are placed over the fused suture at both incision sites. The dura is dissected and carefully detached from the fused bone. During these procedures, a fiber optic suction tip or endoscope is used for the safe and accurate manipulation of the compromising space. Strip craniectomy is performed using curved Mayo scissors, sternal scissors and straight rongeurs. The fused bone is removed from the anterior fontanelle anteriorly to the lambda posteriorly. The width of the craniectomy site is targeted to be between 3 cm to 4 cm. After the strip craniectomy, additional lateral wedge osteotomies or barrel stave osteotomies might be conducted according to the surgeon's preference. Bleeding from the diploic space is controlled by bone wax and monopolar electrocautery. With the insertion of a drain, the wound is closed layer by layer (Fig. 1).
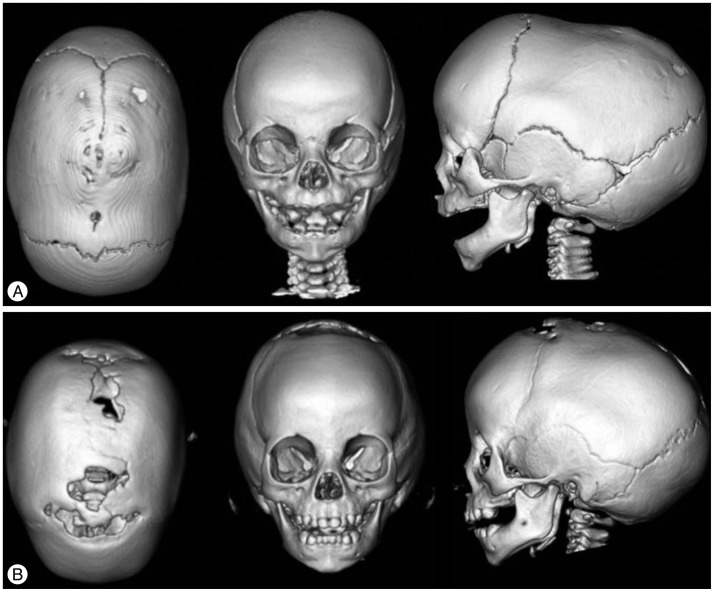
Preoperative (A) and 1-year postoperative (B) 3D reconstructed CT views of a patient with sagittal craniosynostosis treated with minimally invasive suturectomy and postoperatihelmet therapy (left : superior view, middle : anterior view, right : lateral view). Cephalic index is 68% preoperatively and is improved to 75% 1-year after the operation.
For the treatment of anterior plagiocephaly caused by unilateral coronal craniosynostosis, the patient is positioned supine with the head rotated to the contralateral side. A single incision on the stephanion is used by several surgeons, but we use two incisions1337). Two incisions, approximately 2 cm in length, are made at both ends of the fused coronal suture, just lateral to the anterior fontanelle and over the pterion. We prefer two incisions rather than a single incision for the feasibility of manipulation, the direct visualization of the fused ends and to accomplish complete release of the suture. A strip craniectomy is performed 1 cm in width subperiosteally. The craniectomy should run from the anterior fontanelle to the squamosal suture. An additional anterior directed wedge osteotomy might also be performed in cases of accompanied frontosphenoidal craniosynostosis at the level of the squamosal suture (Fig. 2).
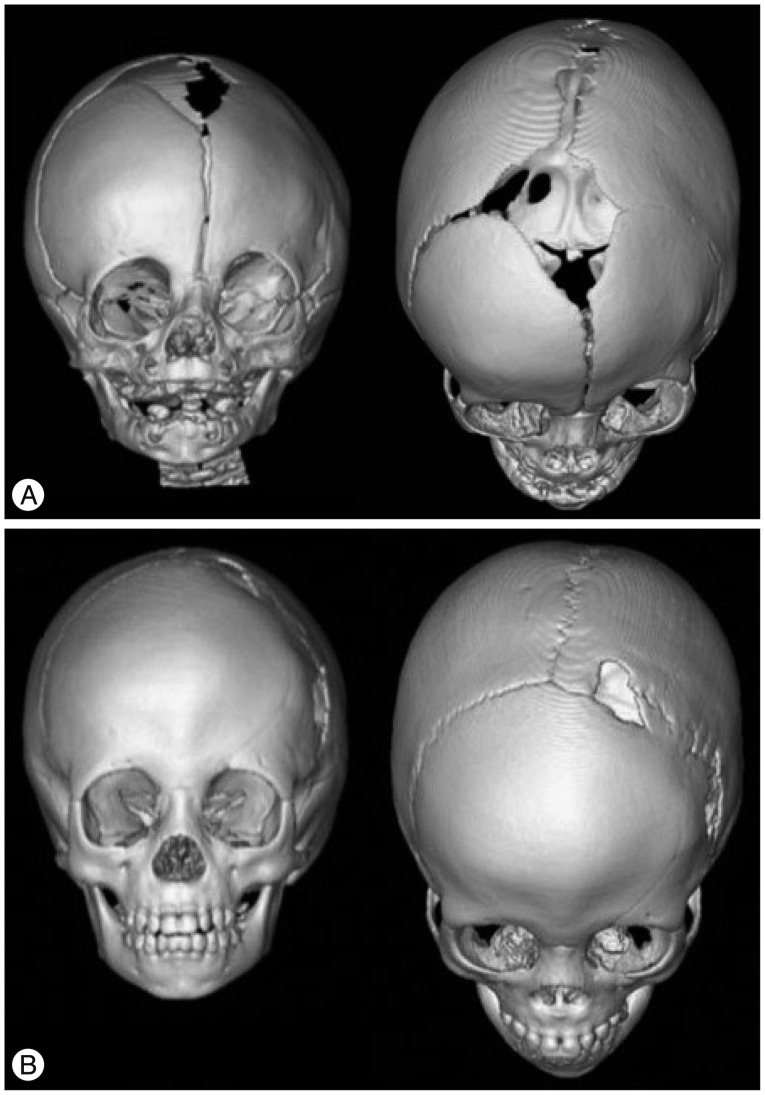
Preoperative (A) and postoperative follow up 3D reconstructed CT images at 2 year (B) after the minimally invasive suturectomy in a patient with left coronal craniosynostosis (left : anterior view, right : superoanterior view). Note that supraorbital asymmetry is improved in 2-year follow up images compared with the preoperative image.
In infants with unilateral lambdoid craniosynostosis presenting as posterior plagiocephaly, the operation is performed with the patient in the prone position. As mentioned for the anterior plagiocephaly, one incision on the fused suture is possible, but we use two incisions, one just lateral to lambda and the mastoid fontanelle along the fused bone. Dissection is conducted in a similar pattern, and the width of subperiosteal craniectomy is also 1 cm (Fig. 3).
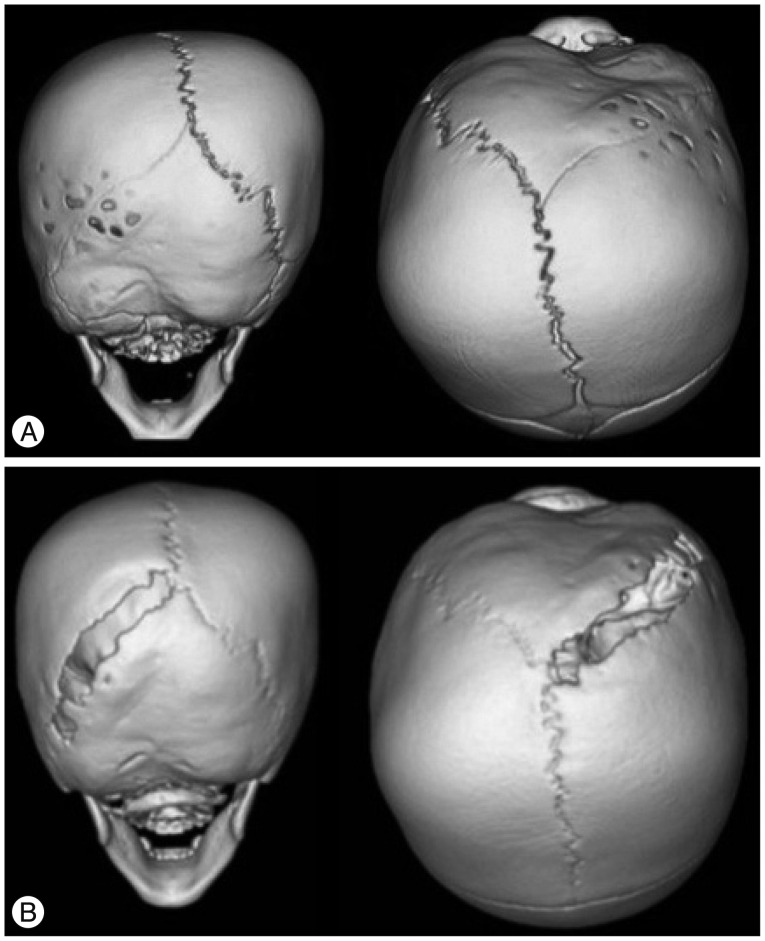
Preoperative (A) and postoperative 1-year follow up (B) 3D reconstructed CT images of a patient with left lambdoid craniosynostosis (left : posterior view, right : superoposterior view). Deformation at contralateral parietal bone and cranial base is improved at the postoperative 1-year follow up images.
POSTOPERATIVE HELMET THERAPY
After the subgaleal swelling is absorbed and all stitches are removed, a cranial helmet is prescribed to redirect balanced growth of the head. The helmet is fitted by orthotists. We recommend wearing it until patients are 12 to 18 months old, during which period rapid brain growth occurs. The helmet allows for three dimensional growth and individual adjustments to its course of correction30). As the patient's head grows, one or two additional orthoses may be required until sufficient correction is achieved. In our experiences, one helmet is sufficient for most cases of sagittal craniosynostosis, and two helmets might be required in cases with plagiocephaly similar to previous reports1431).
TREATMENT OUTCOMES
In sagittal craniosynostosis, correction of the scaphocephalic shape can be measured by changes in CI postoperatively. Jimenez et al.19) reported that 87% of sagittal craniosynostosis patients who were treated with minimally invasive suturectomy and postoperative helmet therapy showed excellent results (CI >75%), and 8.7% of patients showed good results (CI 70–75%). Similar supporting data have been presented by other groups, and comparisons of the CI between the minimally invasive suturectomy with helmet group and the extensive cranial vault remodeling group in a single center revealed equivalent outcomes1234). These results support the promise of minimally invasive suturectomy and postoperative helmet therapy and suggest it to be different from open strip craniectomy, which showed inferior outcomes compared with extensive cranial vault remodeling28). The feasibility of the operation in the early ages due to its minimal invasiveness might be important in this difference because manipulating or releasing the fused suture is important and similar in both open strip craniectomy and minimally invasive suturectomy. Correction of the CI occurs mostly within 2 months of the operation and improves until 6 months119). After that period, correction begins to decrease and reaches a plateau1). Suppressing relapse of the scaphocephaly is one of the expected roles of the postoperative helmet1633). However, we do not suggest that postoperative helmet therapy should be applied in all cases; improvements in CI could be achieved just by suturectomy, and there are few issues of asymmetry of laterality in sagittal craniosynostosis. More studies are needed to identify the effects of the postoperative helmet in sagittal craniosynostosis patients treated by minimally invasive suturectomy.
In view of its safety and minimal invasiveness, the outcomes of minimally invasive suturectomy are remarkable. Transfusion rates in minimally invasive suturectomy during the perioperative period range from 3.3% to 25%, while almost patients need transfusion in extensive cranial vault remodeling1319273140). The operating time (45–100 minutes) is also shorter than in extensive cranial vault remodeling (4–8 hours)4193134). These advantages make the patient less prone to morbidity and require shorter periods of hospital stay.
Treatment of unilateral coronal craniosynostosis is somewhat more complex than sagittal craniosynostosis because asymmetries between the ipsilateral and contralateral side should be considered. Frontal, supraorbital and orbital asymmetries and nasal deviations are well known deformations related to unilateral coronal craniosynostosis. Fronto-orbital advancement is one of the extensive cranial vault remodeling methods for the treatment of unilateral coronal craniosynostosis, which can expand cranial volume and correct asymmetries. However, fronto-orbital advancement often does not modify facial or ocular asymmetries sufficiently modify facial or ocular asymmetries, which result in ophthalmologic problems such as strabismus, ocular torticollis and astigmatism131423). These are problems with the age of the patient rather than the surgical methods because incidences are lowered when fronto-orbital advancement is performed at earlier ages524). Uncorrected facial asymmetries may persist or even worsen in some cases. Jimenez and Barone13) reported that craniofacial scoliosis was corrected completely in 14% of unilateral coronal craniosynostosis patients and partially in 66%. Improvement of vertical dystopia was also achieved completely in 14% and partially in 86% of patients. In comparison with fronto-orbital advancement, minimally invasive suturectomy and helmet therapy showed better outcomes for middle and lower facial asymmetries on comparison37). Contrary to the direct correction of forehead and supraorbital asymmetries in fronto-orbital advancement, changes in minimally invasive suturectomy and postoperative helmet therapy require time, and its final outcome is suboptimal in some cases (Fig. 4)13). However, its improvements in plagiocephaly may be persistent even following reossification of the suturectomy site, and further correction was noted when the frontal sinuses developed14).
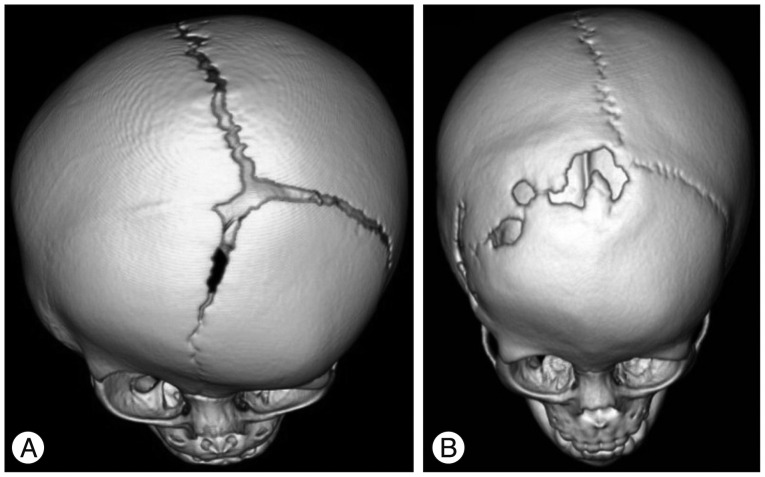
Persistent supraorbital asymmetry of patients with right coronal craniosynostosis. Compared to preoperative (A) images, asymmetry is improved but still present at postoperative 1-year follow up (B).
Unilateral lambdoid craniosynostosis has the feature of posterior plagiocephaly and compensatory contralateral parietal bossing. Compensatory and deformational growth also occurs at the cranial base level, which results in asymmetric external acoustic meatus and mastoid bulging. Extensive cranial vault remodeling for unilateral lambdoid craniosynostosis corrects the cranial vault shape but does not change asymmetries occurring in the cranial base directly. In one study of posterior cranial vault and base asymmetries after open and endoscopic operations, persistent cranial asymmetries were observed with both extensive cranial vault remodeling and minimally invasive suturectomy, and the treatment outcomes were equivocal40). Posterior asymmetries are more acceptable than anterior asymmetries because they can be concealed by hair. The simplicity of the procedure and the theoretical possibility of correction in the cranial base induced by rapid brain growth during the early infant period should make surgeons consider minimally invasive suturectomy favorably.
Multiple-suture craniosynostosis has many problems, including increased intracranial pressure, abnormal head shape depending on involved sutures, compensatory growth and asymmetric ophthalmologic findings. It is more complex than single suture craniosynostosis and differs case by case. Surgical strategies are also different depending upon the major problem. There are few studies of early minimally invasive suturectomy for multiple suture craniosynostosis, but good results have been presented in limited cases1832). In cases with increased intracranial pressure, distractor osteogenesis which is another minimal invasive technique would be more suitable for the sufficient volume expansion39).
LIMITATIONS
The underlying concepts in minimally invasive suturectomy and postoperative helmet therapy are releasing the fused suture in the early period, before severe deformity occurs, and utilizing the potential for normal rapid brain growth during early infancy to reshape it. Therefore, this technique has age limitations, and it is unlikely there will be good outcomes in late infancy, when the driving force is much diminished. Patients over 9 months of age are not suitable for this technique, and extensive cranial vault remodeling should be considered16).
Another limitation of this treatment is the necessity of wearing a helmet for up to 1 year. During that period, regular examinations and adjustments of the helmet are required. Compliance with helmet use can affect treatment outcomes.
CONCLUSION
Minimally invasive suturectomy and postoperative helmet therapy are safe methods to treat craniosynostosis in early infancy, and their esthetic results are comparable to conventional extensive cranial vault remodeling.
Acknowledgements
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI12C0066).