Feasibility of Posterior Cervical Foraminotomy for Adjacent Segmental Disease after Anterior Cervical Fusion
Article information

Abstract
Objective
The aim of this study is to evaluate the feasibility of posterior cervical foraminotomy (PCF) for adjacent segmental disease (ASD) after anterior cervical fusion (ACF). As ACF is accepted as the standard treatment for cervical spondylosis, many studies have been conducted to evaluate the efficacy of various surgical techniques to overcome symptomatic ASD after the previous surgery. Herein, PCF was performed for the treatment of symptomatic ASD and the feasibility of the surgery was evaluated.
Methods
Forty nine patients who underwent PCF due to symptomatic ASD from August 2008 to November 2017 were identified. For demographic and perioperative data, the sex, age, types of previous surgery, ASD levels, operation times, and bleeding amount were recorded. The clinical outcome was assessed using the visual analogue scale for the neck and arm, the modified Odom’s criteria as well as neck disability index. Radiologic evaluations were performed by measuring disc softness, disc height, the cervical 2–7 sagittal vertical axis, cervical cobb angle, and facet violation.
Results
Thirty-seven patients were enrolled in this study. The patients were divided into two groups based on the location of the pathology; paracentral (group P) or foramina (group F). Both groups showed significant clinical improvement (p<0.05). The proportion of calcified disc and facet violations was significantly larger in group F (p<0.05). The minimal disc height decrease with mild improvement on sagittal alignment and cervical lordosis was radiologically measured without statistical significance in both groups (p>0.05).
Conclusion
PCF showed satisfactory clinical and radiologic outcomes for both paracentral and foraminal pathologies of ASD after ACF. Complications related to anterior revision were also avoided. PCF can be considered a feasible and safe surgical option for ASD after ACF.
INTRODUCTION
Anterior cervical fusion (ACF) is widely accepted as the standard treatment option for cervical spondylosis with radiculopathy or myelopathy. Anterior cervical discectomy and fusion (ACDF) with or without fixation, cervical disc replacement (CDR), and anterior cervical corpectomy and fusion (ACCF) are representative surgical techniques in this category. Although ACF provides direct decompression at the index level, the surgical technique affects the kinetics of adjacent levels, facilitating degenerative changes on those levels [13]. Adjacent segment disease (ASD) is a disease that can develop either iatrogenically after ACF or through the natural progression of degenerative changes [22]. The incidence of ASD is reported to range from 2.1% to 22% and most cases are asymptomatic [21]. However, surgical treatment should be considered for ASD that cannot be relieved with conservative treatment or procedures [9]. Hilibrand et al. [9] reported that two-thirds of patients in this category may require secondary surgery.
A variety of approaches and surgical techniques are available for the treatment of ASD after ACF. Reported techniques for ASD after ACF include repeat ACDF, ACDF with a zeroprofile device, CDR, and laminoplasty [3,14,16,18,22]. All of these techniques have shown good clinical results, with Wang et al. [22] reporting a lower incidence of dysphagia in the zero-profile group. Although ASD occurs at the level above or below the level of the previous operation, adhesive tissue and scars from the previous surgery are likely to exist in the anterior corridor. This can increase the difficulty of performing a secondary operation and predispose patients to complications related to vital organs in the anterior neck region such as the trachea, esophagus, recurrent laryngeal nerve, and carotid sheath. In contrast, the posterior approach provides access to virgin tissue; hence, damage to vital organs can be avoided. Laminectomy with internal fixation and laminoplasty have been reported as posterior approach techniques for ASD after ACF [22]. However, posterior cervical foraminotomy (PCF) as a surgical option has never been reported. PCF is appropriate for posterolateral soft disc herniation or cervical foraminal stenosis due to osteophytosis or hypertrophy of the facet joint [10]. The procedure can preserve the range of motion (ROM) at the index segment with a minimal decrease in disc height (DH). It may also improve sagittal alignment and the lordotic angle in addition to preserving the ROM in select cases [5,12]. In this study, PCF was performed for ASD after ACF and the clinical and radiological outcomes were assessed. The location of the pathology was also taken into consideration to determine the appropriate surgical option. Foraminal or extra-foraminal stenosis and disc extrusion are risk factors for facet joint violation; therefore, ACF is widely accepted as a standard treatment option for such cases [17]. However, massive facet violation during PCF can be avoided by widening the vertical width during foraminotomy with inferior lamina resection, making PCF a viable option for these types of pathologies [2]. To evaluate the feasibility of this approach, the study population was divided into two groups, namely the paracentral (group P) and foraminal (group F), based on the location of the pathology and the clinical and radiologic outcomes in the two groups were compared.
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of Wooridul Spine Hospital, and all patients gave informed consent before enrollment.
Patient population, indications, and inclusion criteria
Fifty-four patients that required repeat cervical surgery due to symptomatic ASD from August 2008 to November 2017 were identified. All patients failed to improve after more than 6 weeks of conservative management and developed new radiologic degenerative changes at adjacent levels. Forty-nine patients presented only unilateral radiculopathy without myelopathy, but five patients also suffered from neck pain with myelopathic symptoms. The indication for PCF was unilateral radiculopathy without myelopathy, posterior neck pain, or focal dynamic instability. Focal dynamic instability was defined as a translation of more than 3.5 mm and angulation exceeding 11° in sagittal dynamic plain radiographs [5]. Five patients with myelopathy, posterior neck pain, and focal dynamic instability on adjacent levels were excluded as they had undergone revisional ACDF. Therefore, PCF was performed for 49 patients.
Patients who underwent PCF less than a year after the previous surgery or at a level distant from the prior surgery were also excluded. Complete data with 1 year of medical and radiologic follow-up were available for 37 patients. Four patients were excluded from this study because PCF was performed within a week after the previous surgery due to incomplete decompression or sustained radiculopathy. Five patients underwent surgery at locations distant from the original operated level. Three patients were lost before the 1-year follow-up. Consequently, 12 out of 49 patients were excluded and 37 patients were enrolled in this study.
Surgical technique
All patients underwent surgery in the prone position under general anesthesia. After confirmation of the cervical level using a lateral X-ray, a 3 cm vertical skin incision was made and routine muscular dissection was performed to expose the lamina and facet. A semi-tubular retractor (Papavero-Caspar speculum; B Braun, Melsungen, Germany) was used. Target level confirmation was achieved by checking the lateral X-ray with a micro-surgical probe placed on the targeted lamina. Open microscopic laminotomy and foraminotomy with partial facetectomy were performed using high-speed drills. The medio-lateral course of the nerve root was exposed. If tension on the nerve root remained after foraminotomy, additional bony decompression of the inferior pedicle with a 3 mm diamond burr was performed for patients with foraminal stenosis with calcified discs or traction spurs. For soft disc extrusion cases, additional decompression was performed by discectomy with pituitary forceps. After surgery, patients were placed in a soft collar for 2–4 weeks.
Demographics
Demographic data was collected from the patients’ medical charts. The operated levels, sex, age, type of previous surgery, affected level, relationship of affected levels to the operated levels, interval between first and second operation, and duration of symptoms were recorded as the demographic data. The perioperative data were collected from a review of the patients’ medical charts and operation records. For perioperative data, the operation time, bleeding amount, number of admission days, and complication types were recorded.
Clinical outcomes
Patients were asked by the surgeon to rate their neck and arm pain intensity using the visual analogue scale (VAS) at three time points : prior to operation, postoperative day (POD) 1, and at the 1-year follow-up outpatient visit. Odom’s criteria and the neck disability index (NDI) were applied based on the subjective symptoms and working capacity at POD 1 and at the 1-year follow-up. The data were collected from pre and postoperative medical charts or telephone interviews.
Radiologic outcomes
The disc location, disc softness, DH, C2–7 sagittal vertical axis (C2–7 SVA), cervical Cobb angle (CA), and facet violation ratio were measured from the preoperation, POD 1, and 1-year follow-up plain cervical radiographs (X-ray), computerized tomography (CT) images, and magnetic resonance imaging (MRI) data. The preoperative ROM for the affected level was measured to exclude focal dynamic instability. The angle between the superior endplate of the upper vertebra and the lower endplate of the lower vertebra was defined as the ROM and was measured from flexion and extension images using Cobb’ s method. Discs located medial to the midpoint of the facet were placed in the paracentral group (group P), and those lateral to the midpoint of the facet were placed in the foraminal group (group F) (Fig. 1A). Disc softness was classified as soft, calcified, or mixed based on the density of the CT image. Discs with Hounsfield units similar to that of the cortical bone of the vertebral body were defined as calcified discs. The DH was measured from the midpoint of the upper endplate of the lower vertebral body to the midpoint of the lower endplate of the upper vertebral body (Fig. 1B). The DH was the average value from the X-ray, CT, and MRI results. C2–7 SVA was measured from lateral cervical X-ray images as the distance between the vertical line at the center of the C2 vertebral body and the vertebral line at the superior posterior of the C7 vertebral body (Fig. 1C). CA was measured to evaluate the change in the overall cervical sagittal alignment. Two spinal neurosurgeons individually measured the CA between C2 and C7, which was defined as the angle formed by lines drawn at the base of the axis and the superior endplate of the C7 vertebral body on the lateral radiograph. The mean angle was calculated to accommodate investigator error in assessing the margins of the vertebral bodies (Fig. 1C) [5]. Kyphotic alignment was indicated as a negative value and lordotic alignment was indicated as a positive value. The percentage of the facet joint removed was measured as the ratio of the horizontal length of the original facet joint (A) and the horizontal length of the remaining facet joint (B). The formula for this calculation was [(A–B) / A] × 100. (Fig. 1D) [6]. Measurements were quantified using features included in a picture archiving communication system (PACS; PiViewSTAR; INFINITT Healthcare Co, Seoul, Korea). All radiologic data were measured by each operator, the first author, and the corresponding author of this article. The measurements of the three investigators had an intra-class correlation of 93.2% with statistical significance (p=0.000). The mean value of the three measurements was obtained to further adjust the errors between the investigators.
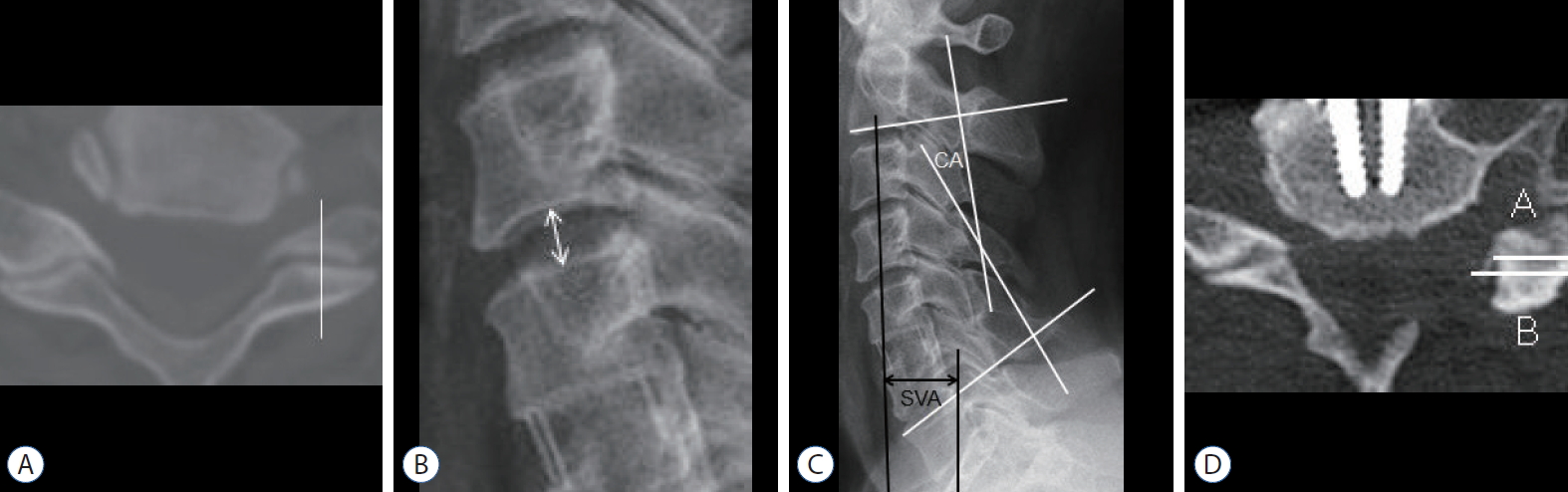
A : The white line is the midline of the facet joint. Pathology across this line was categorized as paracentral while that outside the line was categorized as foraminal. B : Double headed arrow indicates the disc height. It was measured as the length from the midpoint of the upper endplate of the lower vertebral body to the midpoint of the lower endplate of the upper vertebral body. C : The C2–7 sagittal vertical axis (SVA) was measured as the length from the vertical line starting at the center of the C2 vertebral body (vertical black line) to the end point of the superior posterior of the C7 vertebral body (horizontal black line). The cervical Cobb angle (CA) was measured as the angle between two lines parallel to the lower margin of the C2 vertebral body and the upper margin of the C7 vertebral body (white lines). D : The amount of facet resection was measured as the proportion of resected facet (A, white line) compared to the original facet (B, white line). The formula was (A–B) / A × 100.
Statistics
Statistical comparison of the clinical and radiological outcomes was made between groups P and F. An independent sample t-test was used to compare variables with average values and the chi-squared test was used for categorical values between the two groups. A paired t-test was used to compare variables with average values between preoperation and the 1-year follow-up within each group. Statistical analysis was performed using standard software (SPSS ver. 16.0 for Windows; SPSS, Inc, Chicago, IL, USA) and statistical significance was set at p<0.05.
RESULTS
Demographics
As shown in Table 1, ASD after ACF showed male predominance in this study (29, 78.4%). The average age of the patients was 51.7±9.7. The types of previous surgery were ACCF for two patients (5.5%), ACDF for 20 patients (54%), ACDF with a stand-alone cage for 12 patients (32.4%), and CDR for three patients (8.1%). The affected levels were as follows : C3–4 for two patients (5.5%), C4–5 for six patients (16.2%), C5–6 for eight patients (21.6%), C 6–7 for 15 patients (40.5%), and C7–T1 for six patients (16.2%). The affected levels were above the operated level in 10 patients (27%), below the operated level in 20 patients (54%), and the same as the operated level in seven patients (19%). The interval between the first and second operations was 67.70±54.97 months and the symptom duration before the second operation was 11.46±20.78 weeks. Foraminotomy with discectomy was performed in five cases (13.5%) and sufficient decompression was achieved without discectomy for the other 32 patients (86.5%). The operation time was 115.22±46.30 minutes and the bleeding amount was 202.57±105 mL. The average number of admission days was 18.67±29.84 days for all patients but was 9.75±29.06 days for patients without complications. Thirty-three patients (89.1%) did not experience any complications but there were two cases of wound dehiscence (5.5%), one case of wound infection (2.7%), and one case of cerebrospinal fluid leakage (2.7%).
Demographics
Clinical outcomes
The mean follow-up period was 18.5 months, ranging from 13 to 47 months. Patients were divided into two groups based on the location of the pathology that caused the radiculopathy : 14 patients were in group P and 23 were in group F. The clinical outcomes for both groups are summarized in Table 2. The mean VAS for arm pain improved from 8.76±0.83 to 2.76±0.83 in group P and from 8.79±0.77 to 3.03±0.56 in group F. The mean VAS for neck pain improved from 6.13±0.60 to 2.76±0.75 in group P and from 5.71±0.73 to 2.57±0.50 in group F. The improvement persisted until the 1-year follow-up in both groups without significant change. The mean NDI improved from 30.91±4.78 to 11.0±5.42 in group P and from 30.93±3.77 to 10.9±4.22 in group F. In terms of VAS arm, neck and NDI, there was a significant within-group difference between preoperation and 12 months follow-up (p<0.05). The improvement also persisted until the 1-year follow-up in both groups. Based on Odom’s criteria, three patients (21.5%) in group P and five patients (21.7%) in group F were rated as excellent (Odom I), while 11 patients (78.5%) in group P and 15 patients (65.2%) in group F were rated as good (Odom II). None of the patients in group P were rated as Odom III or IV, but two patients (8.6%) in group F were rated as Odom III and one patient (4.5%) was rated as Odom IV. The proportion of patients rated as Odom I and II remained constant until the 1-year follow-up visit. There were no significant statistical differences in the clinical outcomes between the two groups and the outcomes after surgery were satisfactory in both groups.
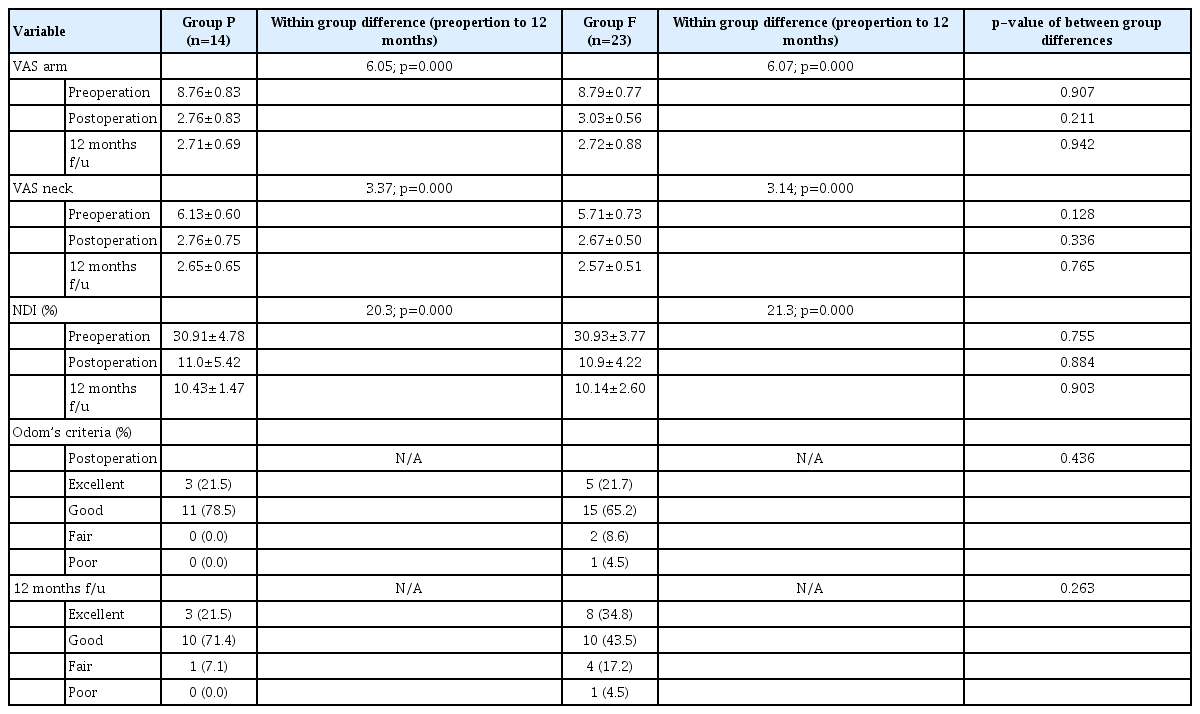
Clinical outcomes
Radiologic outcomes
The radiologic outcomes are summarized in Table 3. The preoperative ROM at the affected level was 9.78±3.45° in group P and 9.34±2.32° in group F and there was no significant difference statistically. These values indicated both groups had ROM restrictions without focal dynamic instability. The majority of patients (12, 85.6%) in group P had soft disc herniation, whereas most (15, 65.2%) group F patients had stenosis with calcified discs or traction spurs. The average Hounsfield unit for calcified discs or traction spurs was 854.23±113.77. Statistical differences were also observed between the two groups (p<0.05). The preoperative average DH was 7.01±1.49 mm in group P and 6.36±1.48 mm in group F. The postoperative DH decreased minimally, with an average DH of 6.86±1.59 mm in group P and 6.19±1.38 in group F. DH was maintained without a significant decrease at the 1-year follow-up in both groups (Fig. 2A). There were no significant within and between group differences. The preoperative C2–7 SVA and CA were 20.62±13.77 mm and 3.14±12.58°, respectively, in group P, and 23.62±12.27 mm and 3.59±11.78°, respectively, in group F. The postoperative C2–7 SVA and CA improved to 16.43±11.60 mm and 7.56±11.13°, respectively, in group P, and to 22.09±10.60 mm and 7.29±11.69°, respectively, in group F. C2–7 SVA and CA remained unchanged at the 1-year follow-up in both groups (Fig. 2B and C). In terms of C2–7 SVA, and CA, there were no significant within and between group differences. Facet violation was significantly larger in group F (p<0.05). The mean facet violation was 29% in group P and 44% in group F.

Radiologic outcomes

A : Disc height change with time shows a minimal decrease after posterior cervical foraminotomy (PCF). B : C2–7 sagittal vertical axis change with time shows the improvement of the sagittal alignment after PCF. C : Cervical Cobb angle with time shows mild recovery of cervical lordosis after PCF. Pre-op : preoperation, Post-op : postoperation, f/u : follow up.
DISCUSSION
There were some interesting findings in the demographic data for the study population. Firstly, 20 cases (54%) of ASD occurred at a level below the index segment and 28 cases (78.3%) were at the lower cervical area (C6–T1). Previous studies reported that lower segments have greater influence on the cervical ROM [4]. Once ACDF is performed, the motion at the index level is fixed and a compensation mechanism is triggered to maintain the cervical ROM. Lin et al. [17] reported that the cervical ROM decreases after ACDF, while the ROM at the upper and lower segments increases. They also reported a significant correlation between the ROM for the lower segment and that of the entire cervical region [17]. The findings in the current study support previous reports indicating the lower segments contribute substantially to the cervical ROM.
Secondly, the previous surgery in 32 cases (86.4%) was ACDF and 12 (37.5%) of these were performed using a standalone technique. ACDF is a widely accepted standard surgery for cervical spondylosis; however, recent studies suggest that the ROM at adjacent levels is significantly higher than that obtained with CDR or PCF by fixing the ROM for the index level [11,17]. Han et al. [8] reported that the stand-alone ACDF group showed more frequent segmental subsidence and cervical kyphosis than the conventional ACDF group. The relatively high proportion of stand-alone ACDF in this study could be explained by the combination of these two effects. Additionally, there were seven cases of surgery at the index level, which was likely induced by the progression of foraminal stenosis after incomplete decompression with the previous ACDF. It is difficult to remove pathologies in the most lateral area using the anterior approach because of uncinate processes; therefore, a combined operation involving anterior foraminotomy or uncinate process resection should be considered for patients with foraminal stenosis to avoid secondary surgery [6].
Performing PCF for ASD after ACF in both the P and F groups resulted in satisfactory clinical and radiologic outcomes in this study and the outcomes persisted 1 year later. Radiologic examinations showed minimal DH decrease with slight recovery of the cervical alignment and lordotic angle as the patients’ symptoms were relieved. Kyphotic cervical deformity with malalignment is known as a contraindication for surgery with a posterior cervical approach. However, a report indicated that the deformity could be overestimated because of pain-induced muscle spasms [5]. Temporal kyphosis and shifted SVA can also be caused by posterior neck pain and muscle spasms; therefore, PCF can be performed for select patients with acute malalignment. Since C2–7 SVA and CA cannot be fixed by mechanical deformity, the alignment and lordotic angle could be improved for such patients [5,12,15]. Acute onset kyphosis should not be considered as an absolute contraindication.
Group F had a higher facet violation rate (44%) than group P (29%) in this study. This is because the pathology was located in a more lateral area in group F and facetectomy was necessary for complete decompression. Some studies suggest that facet resections greater than 50% can induce instability; however, existing evidence suggests complete decompression is more important than the avoidance of facet resection as long as the proportion of the violation falls in the range of 25–50% [6,23]. There was also no instability observed in this study within 1 year of follow-up, but a longer follow-up period is needed. For patients with diffuse foraminal stenosis, which may invade the facet joint by more than 50%, ACDF is recommended [5].
Performing surgery for ASD after ACF through the anterior corridor bears the risk of damaging anterior vital organs. Complications such as dysphagia, dysphonia, and injury to the vertical axis, sympathetic chain, esophagus, and other structures have been reported [19]. Basques et al. [1] reported that there were more thromboembolic events, surgical site infections, and readmission within 30 days in the revision ACDF group. On the other hand, posterior approaches provide access to virgin tissue in the ASD region, thus, complications related to revision anterior-approach surgery can be avoided. In this study, there were no severe complications except for two cases of CSF leakage and one case of wound infection. Total laminectomy with lateral mass fixation or laminoplasty have been reported as surgical options for ASD after ACF that can avoid complications related to anterior organs [22]. However, these techniques require a wider incision and muscle dissection, consequently damaging the posterior neural arch. This affects not only the postoperative neck pain, but also aggravates postoperative kyphosis. In contrast, PCF can be performed with fewer invasions on the posterior neural arch, less bleeding loss, and a shorter operation time. Furthermore, PCF can preserve the ROM at the operated level, which can prevent further ASD occurrence on levels above or below. However, there are several pitfalls of this technique such as postoperative neck pain, progression of kyphosis, nerve root injury, and difficulty with bleeding control [7,10]. The procedure is contraindicative for central disc herniation, axial neck pain without radicular symptoms, and patients with dynamic instability [20]. PCF therefore appears to be a feasible surgical option for ASD after ACF capable of preserving cervical motion and preventing the occurrence of additional ASD.
This study is meaningful as it is the first to analyze PCF as a revision surgery for ASD after anterior-approach cervical surgeries. However, this study is retrospective with a relatively small number of patients and lacked randomization. There is a possibility of selection and recall bias, and generalization of the results of this study should be approached with caution due to the small patient population. A prospective study with a larger number of patients is need to validate the effectiveness of PCF after ASD and a longer follow-up period is needed to confirm the improvement in C2–7 SVA and CA is not temporary.
CONCLUSION
Minimal invasive microscopic PCF on ASD after ACF showed good clinical and radiologic outcomes for paracentral and foraminal pathologies. The complication rate was also minimal, with no severe complications related to anterior revision. Based on the results of the study, PCF is presented as an effective and safe option for secondary surgery for ASD after ACF.
Notes
No potential conflict of interest relevant to this article was reported.
INFORMED CONSENT
Informed consent was obtained from all individual participants included in this study.
AUTHOR CONTRIBUTIONS
Conceptualization : HJK, MSK
Data curation : HJK, SWC, ESP
Formal analysis : HJK, YHS, SYL
Funding acquisition : SHL, CHP
Methodology : HJK, MSK
Project administration : SHL, CHP
Visualization : HJK, MSK
Writing - original draft : HJK, MSK
Writing - review & editing : HJK, MSK