Coil Embolization in Ruptured Inferior Thyroid Artery Aneurysm with Active Bleeding
Article information
Abstract
We present a unique experience of urgent parent arterial embolization for treatment of an aneurysm of the inferior thyroid artery (ITA) that bled during tracheostomy. The event happened to a 69-year-old female patient with subarachnoid hemorrhage and hospital-acquired pneumonia that required tracheostomy. Abrupt and massive bleeding developed during the procedure, and the source could not be identified. Under manual compression, angiography revealed an 8-mm aneurysm that arose from the inferior thyroid artery. The superselected parent artery of the aneurysm was successfully occluded with a single pushable coil. The patient's postoperative course was uneventful.
INTRODUCTION
A true aneurysm of the inferior thyroid artery (ITA) is extremely rare15). Despite its rarity, several authors have recommended aggressive management because the lesion has the potential to be highly lethal4). Surgical ligation and/or excision and endovascular embolization were reported as possible treatments for this rare disease6).
Here, we present a case of ruptured ITA aneurysm successfully treated with embolization. To the best our knowledge, this is the first report of parent arterial embolization using a single pushable coil for ITA aneurysm.
CASE REPORT
A 69-year-old woman was hospitalized in a stupor and was diagnosed with subarachnoid hemorrhage due to rupture of an anterior communicating artery aneurysm. During hospitalization, she developed pneumonia, which worsened and required endotracheal tube insertion, and eventually tracheostomy, despite nearly complete neurologic recovery.
Bleeding occurred during blunt dissection with hemostatic forceps for tracheostomy. The bleeding was too abrupt and massive to be controlled, and the source could not be identified. Her respiration was relatively stable due to the endotracheal tube. Temporary hemostasis was achieved with manual compression followed by meticulous packing of gauze and pad. Her hemoglobin decreased to 9.6 from 12.4 g/dL.
Neck computed tomography (CT) angiogram with three-dimensional reconstruction demonstrated a saccular aneurysm of the right ITA (Fig. 1). The patient was immediately prepared for endovascular intervention because the tentative hemostasis and poor general condition of the patient made surgical exploration risky. After groin site puncture, conventional angiography through the thyrocervical trunk (TCT) revealed an ITA aneurysm 8 mm in diameter (Fig. 2A). The right TCT was superselected, and a microcatheter was placed adjacent to the aneurysm. A single pushable embolization coil (18S, 3/2, Tornado Embolization Microcoils Soft, Cook, Bjaeverskov, Denmark) was inserted and placed in the parent artery immediately proximal to the aneurysm (Fig. 2B). The aneurysm was no longer visible on angiogram 10 minutes after insertion of the coil (Fig. 2C). There was no additional bleeding after removal of the packed materials. Follow-up CT three days after embolization evidenced the complete disappearance of the aneurysmal sac (Fig. 2D).

Neck computed tomography angiogram immediately after temporary hemostasis showing a saccular aneurysm (arrow) at the inferior thyroid artery.
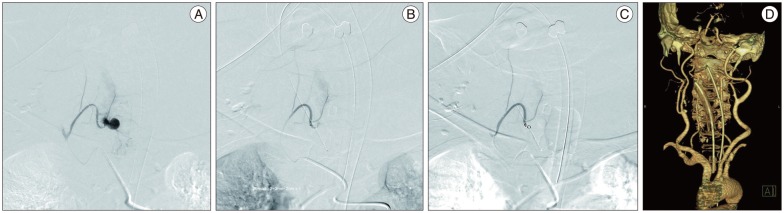
A : Selected angiography into the thyrocervical trunk shows an inferior thyroid aneurysm 8 mm in diameter. B : Immediately after insertion of a single pushable coil into the parent artery, staining of the aneurysmal sac is still visible. C : Ten minutes later, the parent artery is completely occluded. D : Three days after the procedure, no aneurysm is seen on follow-up neck computed tomography angiogram.
Detailed history taking to investigate possible causes of the rare aneurysm did not reveal any history of previous neck surgery, percutaneous procedure, or trauma. There was no history of other connective tissue disorder. Follow-up angiography on the seventh postoperative day confirmed the absence of the aneurysmal sac. The patient's postoperative course was uneventful.
DISCUSSION
A true aneurysm arising from the TCT is extremely rare. Although ITA aneurysm is the most common form of TCT aneurysm, there have been fewer than 25 cases reported in the literature13). Among these, only four cases were treated by coil embolization alone4,5,9,10). Various clinical manifestations of these aneurysms have been reported, including palpable neck mass, hoarseness, dysphagia, respiratory distress, or evaluation of a possible thyroid nodule1,8,12,14).
ITA aneurysms are widely considered to require aggressive management, because mortality has resulted from conservative management in all but one case4). Moreover, a report on the only patient who survived conservative management did not include follow-up data, and such treatment was not recommended. Rather, the patient refused to consent to any invasive procedures7). An abrupt death could result from hypovolemia due to excessive blood loss into soft tissues or the thorax, including the pleura and mediastinum, or respiratory distress due to airway compression by the hematoma itself.
Surgical ligation and/or excision, endovascular embolization, and a combination of these tactics have been reported as a treatment of ITA aneurysm4,13). Among these methods, surgical ligation could be the most suitable, especially in cases of rupture, because the mass effect of the hematoma remains troublesome for airway maintenance after coil embolization. Pop et al.13) reported a case of ruptured ITA aneurysm treated with aneurysmal coil embolization followed by surgical excision. They suggested that embolization had the advantage of easy detection and embolization, while surgical exploration and excision was needed for hematoma evacuation to decompress the airway. Surgery, however, also has the disadvantage of risks including recurrent laryngeal or phrenic nerve injury and wound site infection13).
In the present case, tracheostomy was routine and performed by experienced surgeons. The aneurysm ruptured during blunt dissection, although it is unclear if the rupture was caused by direct contusion of the aneurysmal sac by hemostat forceps or tearing of previously adhesive aneurysmal sac to adjacent soft tissue by blunt dissection. Sharp surgical tool or monopolar electrocautery that could incur an arterial injury was not used at the timing of event. We had concluded that it was a true aneurysm that ruptured during procedure. However, there was no absolute evidence of a true aneurysm like pre-procedural image or pathologic specimen in this case. There were several reports about iatrogenic aneurysm near thyroid gland, following vascular catheterization2), percutanous needle biopsy of adjacent organ8) and radiotherapy3). There was also a case report of tracheostomy-related pseudoaneurysm that developed in superior thyroid artery11). However, those authors described that it was a revision tracheostomy and they found densely fibrotic change at that site that may leaded blunt injury. Moreover, in most cases of iatrogenic pseudoaneurysm, there were delayed intervals between traumatic events and aneurysmal developments, except in that case of penetrating injury. In this case, immediate CT angiogram and conventional angiography showed a saccular aneurismal sac.
Bleeding was so severe that it could not be directly controlled in this patient. Percutaneous intervention was effective in this urgent case for both diagnosis and treatment. Moreover, parent arterial embolization following superselection was advantageous for its speed and effectiveness. Tornado®, the single pushable coil that contains numerous fibrous hairs, completely ablated the vessel within several minutes with minimal mass effect. This method could be also beneficial even in a case of pseudoaneurysm that contains a fragile wall. Mass effect from a hematoma was not a problem in this case due to prompt manual compression.
CONCLUSION
ITA aneurysm is a rare, but potentially lethal lesion. Selective angiography is the diagnostic modality of choice, particularly in emergency settings, because it can be promptly transformed into a therapeutic procedure. The author suggests that embolization of the parent artery using a pushable coil is a simple and effective treatment modality for ITA aneurysm with rupture.