INTRODUCTION
Cushing’s disease (CD) is characterized by excessive secretion of adrenocorticotropic hormone (ACTH) by a corticotropic adenoma in the pituitary gland. In patients with CD whose hypercortisolism is inadequately corrected, morbidity and mortality can increase by up to 4.8 times due to Cushingrelated complications such as osteoporosis, hypertension, dyslipidemia, insulin resistance, and hypercoagulability [11,18].
Endoscopic transsphenoidal surgery (ETSS), the first-line treatment for CD [7], is performed to decrease complications while achieving remission and long-term disease control. Previous studies on CD have reported varying remission rates between 45% and 95% and recurrence rates ranging from 3−66% [2,4,9,16,21,30]. This wide range of differences can be primarily attributed to differences in surgical experience among centers: centers with higher surgical experience have fewer postoperative complications and higher remission rates [4,6]. However, despite initial remission, patients with CD may eventually experience recurrence. The mean recurrence rate at the 5-10-year follow-up is 23% for microadenomas and 33% for macroadenomas [19,23,30].
Since the postoperative rates in the literature are variable, additional data from experienced centers may be necessary to resolve these discrepancies. In this study, we present the medium- and long-term follow-up data from 96 operations for CD that were conducted in a center with a high level of experience for ETSS.
MATERIALS AND METHODS
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of Basaksehir Cam and Sakura City Hospital (No. 2022185). Informed consent was obtained from all patients. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
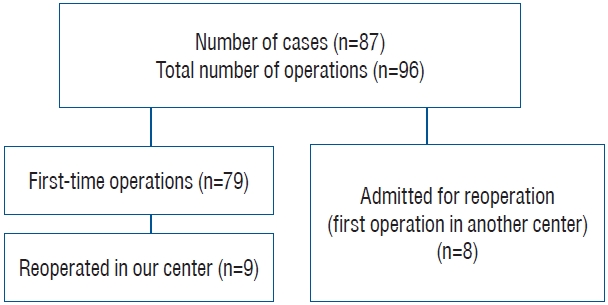
This retrospective study included pre and postoperative data of 96 ETSS performed in 87 patients with CD (Fig. 1). CD was diagnosed based on unsuppressed cortisol levels (>1.8 µg/dL) following the 1-mg dexamethasone suppression test, high levels of urinary free cortisol, or late night salivary cortisol and plasma ACTH levels >20 pg/mL [28]. Between 2014 and 2022, all surgeries were conducted by the experienced neurosurgical team (Ö.G., O.T., B.E., E.A.) responsible for endoscopic transsphenoidal procedures at the Pituitary Research Center. The surgeries were performed under perioperative glucocorticoid coverage.
Size, cavernous sinus invasion, sellar and suprasellar infiltration of adenoma on preoperative magnetic resonance imaging (MRI) scans, residual tumor on postoperative MRI scans, postoperative complications, pathology results, remission and recurrence status, and additional postoperative management were evaluated in addition to patients’ demographic data. For follow-up assessments, data obtained 3−6 months postoperatively and during the latest follow-up were included. Three different classifications obtained during radiologic evaluation using MRI were used for pituitary adenomas : 1) maximum size of tumor (MST) : 0−5 mm (group 1), 6−10 mm (group 2), 11−20 mm (group 3), and >20 mm (group 4); 2) Knosp classification : for evaluation of cavernous sinus invasion [22]; and 3) modified Hardy classification : for evaluation of sellar and suprasellar infiltrations [20,39].
In cases of CD without a lesion or with a lesion <6 mm on MRI, confirmation of the central origin and lateralization was provided by inferior petrosal sinus sampling (IPSS) with corticotropin-releasing hormone stimulation [25,26,29]. Under neuronavigation guidance, pure ETSS surgical interventions were performed for all patients by a single surgical team using the Medtronic StealthStation™ S7 and S8 systems (Medtronic, Minneapolis, MN, USA) together with 4-mm 0°, 30°, and 45° rigid optical instruments and an endoscope. A nasal decongestant spray was administered 1 hour before the operation. The sphenoid ostium was detected from both nostrils, and a bi-nostril approach was used by resecting the posterior nasal septum. After sphenoidectomy, the standard sellar approach was used for lesions in the sellar region. The details of these surgical procedures are described in previous study [14]. Selective adenectomy with ETSS was performed for preoperatively localized and visible tumors, whereas hemihypophysectomy was performed for non-lesional cases. In cases with cavernous sinus-invading tumors, particularly Knops 3-4, the defect which was created by the tumor on the medial wall of anterior cavernous sinus was identified and, it was expanded for resection of the tumor tissue within the cavernous sinus. If a defect was not visible, blunt-ended hook-shaped dissectors were used to create a defect on the medial wall, allowing access for the tumor to enter the cavernous sinus. Hematoxylin and Eosin (H&E) and immunohistochemistry staining were performed for the specimens obtained during ETSS. Adenomas showing positive immunohistological staining for ACTH were diagnosed histologically as corticotropinomas.
CD was considered to be in remission when the cases showed basal cortisol levels <5 µg/dL or suppressed cortisol levels (≤1.8 µg/dL) following the 1-mg dexamethasone suppression test, 3-6 months postoperation, and during the latest follow-up. The study protocol was approved by the ethics committee of our institution.
Data were statistically analyzed using the SPSS 15.0 package (IBM Corp., Armonk, NY, USA). The chi-square test was used for categorical variables. Sample distribution was evaluated with the Kolmogorov-Smirnov test. Continuous independent variables with a normal distribution were compared using the Student’s t-test. Continuous variables with non-normal distributions were compared using the Mann-Whitney U test. p<0.05 was considered statistically significant. A Kaplan-Meier survival analysis was conducted to determine probability and time to recurrence in cases with initial remission.
RESULTS
Demographic data
A total of 96 ETSS were performed for 87 patients with CD. Of the 87 patients, 68 (79%) were female, and 19 (21%) were male. The mean patient age was 42.2±12.9 years, and the mean duration of follow-up was 39.5±3.2 months. Of the 96 surgeries, 79 (82%) were performed for the first time, six (6%) were performed for residual tumors, and 11 (12%) were performed following a recurrence of the disease. Eight of the 17 patients who underwent reoperations had undergone their first operation at another center.
Preoperative imaging
Table 1 shows the maximum tumor size on preoperative pituitary MRI before each surgical procedure. Preoperative IPSS for lateralization was performed in 42 operations (44%), all of which were first-time cases. Knosp classification based on preoperative pituitary MRI and the modified Hardy classification is presented in Table 1.
Postoperative results
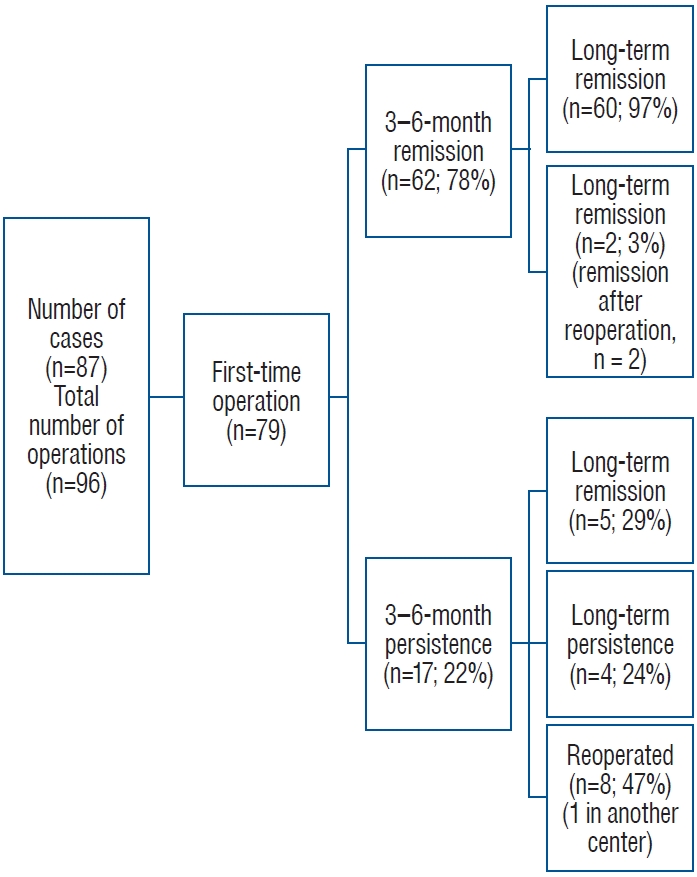
Remission was achieved between the 3rd and 6th months in 74 (77%) of the 96 operations, and long-term remission in 79 operations (82%). Among all 96 operations, eight (8%) concluded with a residual tumor. Regarding only first-time operations, five (6%) of the 79 concluded with a postoperative residual tumor. Of the 79 first-time operations, there were 62 cases (78%) of remission between 3 and 6 months. Two (2.5%) of these 79 operations involved recurrence during follow-up, while 60 (97%) showed sustained remission. Those with sustained remission had a median disease-free survival time of 31 months (interquartile range, 14-64) during long-term followup, two cases with recurrence had their recurrence 49 and 54 months after their operation. Survival analysis of cases with remisson and recurrence is presented in Fig. 2. CD persisted after 17 (21.5%) of the 79 first operations.
Ten (13%) of the 79 cases underwent reoperation; two were due to recurrence, and eight due to disease persistence. In five cases (29%), the patients were initially unresponsive but showed remission later during the long-term follow-up. Remission was achieved with stereotactic radiosurgery (STRS) and medical treatment in one of these cases, with only STRS in two and only medical treatment in two cases. At the latest follow-up visit, the total number of cases showing remission after the first operation was 65 (82%). Additional details regarding the results of the first operations are provided in Fig. 3.
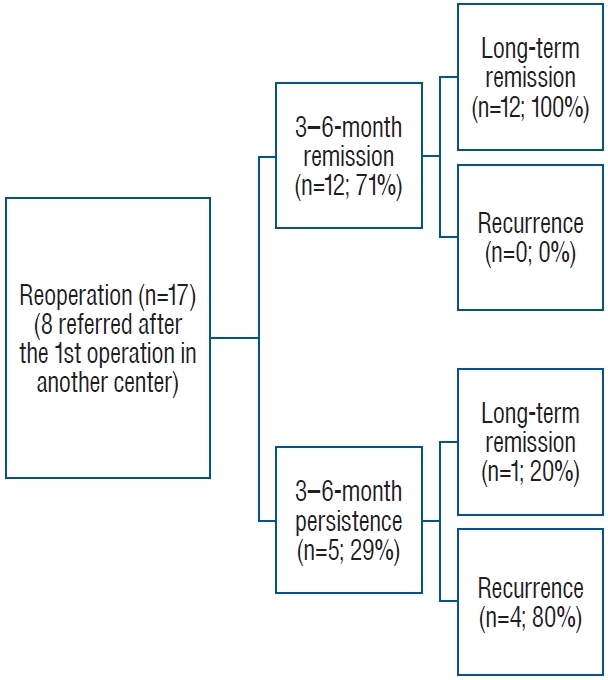
Of the 18 reoperations, the results for one case were excluded since the patient was operated at another center. After the reoperation (n=17), the medium and long-term remission rates were 71% (n=12) and 77% (n=13), respectively. The 3-6-month remission rate did not differ significantly between first-time and reoperations (p=0.5). Residual tumors were present in three cases (18%) after reoperation. Of the early non-responders, one case showed remission after STRS, and none of the responders showed recurrence during long-term follow-up. Additional details regarding the results of reoperations are provided in Fig. 4.
Remission rates based on tumor size are presented in Table 2. The initial remission rates of the tumors in MST group 4 were significantly lower than those in the other MST groups (MST 1 vs. 4, p=0.01; MST 2 vs. 4, p=0.001; and MST 3 vs. 4, p=0.006). Comparisons of the other MST groups showed no significant differences. When adenomas were stratified using the 10-mm cut-off, the remission rates did not differ significantly (remission rate, 81% for adenomas <10 mm and 68% for adenomas ≥10 mm; p=0.2). Postoperative residual tumors were observed in five of the 11 tumors (46%) >2 cm (MST group 4) and in one tumor in each of MST groups 1-3 (2%, 4%, and 5%, respectively, p<0.001). Reoperation rate was 17% (n=7) for adenomas ≤5 mm, 18% (n=10) for adenomas ≥6 mm (p=0.9), and 27% (n=3) for adenomas >20 mm (among all grades, p=0.3).
Remission rates based on Knosp and Hardy classifications are presented in Table 2, respectively. The medium-term remission rates in Knosp group 4 were significantly lower than the rates in the other groups (Knosp 0 vs. 4, p<0.001; Knosp 1 vs. 4, p<0.001; Knosp 2 vs. 4, p=0.04; and Knosp 3 vs. 4, p=0.003). Additionally, the medium-term remission rate of tumors in Knosp group 2 was lower than that in Knosp group 1 (p=0.04). However, remission rates did not differ significantly among the other groups. Comparing invasive (Knosp 3 and 4) and noninvasive (Knosp 0, 1, and 2) tumors, remission rates within 3-6 months were 50% and 83% in the invasive and noninvasive groups, respectively. We further stratified cases with tumor size ≥20 mm (n=11) using Knosp classification; one case (9%) was Knosp 0, one case (9%) was Knosp 1, two cases (18%) were Knosp 3, and seven cases (64%) were Knosp 4 tumors. For ≥20 mm, all cases with Knosp 0, 1, and 3 tumors achieved remission within 3-6 months postoperatively, while none of the cases with Knosp 4 tumors had remission (p=0.01). All the cases with Knosp 0, 1, and 3 tumors sustained remission, and three cases with Knosp 4 tumor later achieved long-term remission (p=0.3). Of the cases that achieved long-term remission, two underwent STRS, and one had medical therapy with additional STRS.
Of the 96 tissue specimens obtained during ETSS, 71 (74%) stained positive for ACTH and were histologically identified as corticotropic adenomas, while 25 (26%) were negative. Remission rates based on the pathology results are compared in Table 2. Of the lesions with conclusive findings on MRI (≥6 mm lesions), 89% (n=49) were pathologically confirmed as corticotropinomas, whereas 54% (n=22) of those with inconclusive MRI f indings were pathologically conf irmed (p<0.001). Among the lesions that showed negative results for both conclusive MRI findings (≤5 mm) and pathologic confirmation (negative for a corticotropinoma) (n=19), 12 (63%) showed remission at 3-6 months and 14 (74%) showed remission during long-term follow-up.
During the exploration of the cavernous sinus in one patient (1%), postoperative lateral gaze paralysis of the eye developed due to right abducens nerve palsy. The patient was treated with anti-inflammatory doses of steroids, and the symptom completely resolved within 1 month. In three other patients (3%), severe epistaxis was observed in the postoperative period, 1 to 3 weeks after surgery. Nasal packing was applied for 3 days. Additionally, three patients (3%) experienced postoperative rhinorrhea. To address this issue, a reconstruction of the skull base was performed using fat tissue harvested from the leg, fascia lata graft, and tissue adhesive material. These patients were monitored with a lumbar drain for 1 week. Among the patients who developed rhinorrhea, one patient also developed meningitis and received intravenous antibiotic therapy for about 3 weeks and, the situation compeletly resolved during follow-up. The postoperative complications are summarized in Table 3. Comparison of various characteristics of the cases with and without medium and long-term remission are presented in Table 3, respectively.
DISCUSSION
This study reported an overall postoperative 3-6 month remission rate of 77% and a long-term remission rate of 82% after 3 years of follow-up. The initial and long-term remission rates after first operations were 78% and 82%, respectively, with a recurrence rate of 2.5% over a follow-up period of 3-3.5 years. Additionally, our findings revealed that tumor size >2 cm and extended tumor invasion of the cavernous sinus (Knosp 4) might be associated with lower postoperative remission rates. Patients who showed remission within 3-6 months showed higher rates of long-term remission than those in patients without initial remission.
Pituitary surgery is the first-line treatment modality for CD. ETSS is a safe and less invasive method for treating pituitary adenomas; therefore, it has been increasingly preferred in CD [5,15]. However, the postsurgical outcomes in patients with CD have shown variable remission and recurrence rates [2,4,9,16,17,21,30]. These discrepancies may be attributable to differences in population and number of cases involved in the studies, tumor characteristics, criteria for remission and recurrence used by the centers, laboratory parameters, time of evaluation and followup durations, surgical and imaging techniques used by different centers, and neurosurgical expertise.
In this study, we present the medium- and long-term postoperative results of 96 ETSS procedures performed in 87 patients. The medium-term results (obtained 3-6 months postoperation) were preferred to immediate results since a subset of cases may show delayed remission, and immediate postoperative results could be misleading in almost 6% of cases [37]. The overall medium-term remission rate was 77%, consistent with the results published by Serban et al. [34], who reported an overall remission rate of 77% 2 months postoperation. A larger series of 1106 cases reported an immediate remission rate of 72.5% within 7 days postoperation; however, this rate decreased to 67% after delayed remission rates and recurrences 56 months postoperation were considered [12]. The long-term remission rate obtained over a median period of 3 years was 82% in our series. The increased long-term remission rate was attributed to reoperations, additional medical therapies, and the use of STRS in those who did not show remission initially.
Of the 96 procedures, 79 were performed for the first time. The medium-term remission rate after first operations was 78%. Recent studies have reported remission rates of 74-82% after first operations [12,34]. The recurrence rates reported previously varied between 3% and 66% [5,12,34]. However, the duration of follow-up differed among the studies. Dai et al. [12] and Brady et al. [5] reported recurrence rates of 12% and 3%, respectively, after a follow-up period of 2 years. In contrast, Serban et al. [34] reported a recurrence rate of 17% after a longer followup duration of 6 years. In this series, after a median follow-up period of 3 years, the overall recurrence rate was 2.5%. Residual tumors were observed in five cases (6%), and the reoperation rate after the first operation was 13%. Including the eight patients admitted for reoperation after having undergone their first surgery in another center, 17 cases involved reoperations in our center. Of these cases, 71% (n=12) showed remission between 3-6 months postoperation, while none showed recurrence; thus, the long-term remission rate was 77%. Residual tumors were detected in three cases (18%), and the disease persisted in four (24%) of these 17 reoperated cases. Previous studies have reported remission rates of 22-75% after repeated surgery in CD [5,12,34,38]. Although the success rates after reoperations were lower than those in first-time operations in some studies [38], the remission rates after the first and reoperations did not differ significantly in our study.
Tumor size has been reported to contribute to the success of transsphenoidal surgery [12,34], with microadenomas showing a higher success rate after surgery [5,12,34]. Our remission rates for micro- and macroadenomas were similar to those reported by Dai et al. [12] : 81% for adenomas <10 mm and 68% for adenomas ≥10 mm. However, the statistical significance of our study differed from that in the series presented by Dai et al. [12] (p=0.2 vs. p=0.002). This may be due to the large difference in the number of cases included in the two studies and the differences in size scales for tumors ≥10 mm. In our series, when the tumors were stratified further by the tumor size, the medium-term remission rate further decreased to 36% for tumors ≥20 mm in size, although the remission rates for other groups <20 mm were all above 75% (p=0.003). Sharifi et al. [35] classified pituitary MRI scans in CD showing a tumor size <6 mm as “inconclusive” because incidentalomas are frequent among tumors in this size range, and this size is not indicative of CD. Previously published series reported that the rate of inconclusive MRI scans in CD was 36-64%, and the remission rates varied between 50% and 71% for those with an inconclusive MRI scan [10,24,27,32,33]. In our series, 54% of the preoperative MRI scans were inconclusive. In the series presented by Sharifi et al. [35] and some other series [8,12,32,36], no significant difference was observed between the remission rates of CD cases with and without a conclusive MRI.This finding is controversial since other studies showed decreased remission rates with preoperative inconclusive MRIs [13,40]. Similar to the results reported by Sharifi et al. [35], we did not find a statistically significant difference between the remission rates of tumors <6 mm and those between 6-20 mm. However, a significant difference was observed between tumors <6 mm and those ≥20 mm. Residual tumors were more frequent after operating tumors >20 mm compared to those <20 mm, but the number of reoperations did not differ among the groups. Additionally, tumors >20 mm were primarily Knosp 4 (64%), probably contributing to lower remission rates in this group. Interestingly, two Knosp 3 cases had postoperative remission within 3-6 months without additional intervention. In these two cases, the surgical team explored the cavernous sinus and could resect the tumor. However, complete excision was not feasible with Knosp 4 tumors, where there is a complete encasement of the intracavernous internal carotid artery. Thus, a tumor size of 20 mm may be supportive data in predicting non-remission in the presence of complete cavernous sinus infiltration.
Cavernous sinus invasion, determined by the Knosp classification, and sellar invasion and/or suprasellar extension, determined by the Hardy-Wilson classification, indicate the radiologic status of local invasion in cases of pituitary tumors [20,22,39]. Invasion to surrounding structures and tissues may be a limiting factor for postoperative remission of pituitary tumors. In the series presented by Dai et al. [12], remission rates of corticotropinomas with Knosp grade 4 (definitive cavernous sinus invasion) dropped to 53% from a remission rate of 77% for corticotropinomas with less likely or no cavernous sinus invasion (p<0.001). Similarly, our results showed that both medium- and long-term remission rates for Knosp grade 4 tumors decreased to 13% and 50%, respectively, and were lower than the remission rates in other grades (p<0.001 and p=0.01, respectively). While remission rates in Knosp group 3 were not inferior to noninvasive tumors, remission rates in Knosp group 4 were lower than all the other groups. In this regard, the extent of invasion may be more determinative. In contrast, in our series, the modified Hardy classification did not show a significant effect on postoperative remission rates in medium- and long-term follow-up assessments. Araujo-Castro et al. [3] had previously shown that for pituitary adenomas, the Hardy-Wilson classification lacked utility in predicting postoperative remission compared to the Knosp classification. The difference in the utility of these classifications for predicting postoperative remission may be due to differences in accessing tissues during surgery.
In the present series, 74% (n=71) of tissues were histologically proven to be corticotropinomas, while 26% (n=25) did not show histologic confirmation. Medium- and long-term remission rates did not differ between histologically proven and unproven CD cases (medium-term remission rates, 82% vs. 64%, p=0.07; long-term remission rates, 85% vs. 76%, p=0.3). A conclusive finding of an adenoma on MRI increased the rate of histologic proof of corticotropinoma in our series, implying that adenomas showing a ≥6-mm lesion on MRI more frequently stained positive for ACTH. In previous studies 12-53% of CD did not have postoperative pathologic identification and the rate increased in those with a preoperative inconclusive MRI [25,31,38]. However, this did not have a significant influence on our remission rates. The remission rates did not decrease even for CD cases that were not conclusively detected on MRI and could not be histologically proven. On the other hand, in previous studies, ACTH positivity was higher, and the lack of proof for a corticotropinoma decreased the remission rates [1,12,31,32,34]. The higher remission rates despite reduced localization with MRI and/or lower rates of histologic confirmation in our series may be explained by the successful preoperative IPSS lateralization, surgical exploration, and hemi-hypophysectomy procedure. Furthermore, tumor tissues might have been aspirated along with blood and other materials through the suction tube, potentially resulting in less histological confirmation despite postoperative remission of CD.
Additionally, tumor tissues might have been aspirated along with blood and other materials through the suction tube, potentially resulting in less histological confirmation despite postoperative remission of CD.
The total rate of complications in this series was 20%, and the most frequent complication was diabetes insipidus (DI; 8%, both permanent and temporary). The incidence of hypopituitarism was relatively lower (4%), mainly involving hypocortisolism and hypothyroidism. Recent studies have shown postoperative DI rates of 25-66% and hypothyroidism rates of 11-23% [5,34]. Although our neurosurgical team was experienced in conducting pituitary surgeries, other factors may have resulted in these differences. Since not all the cases were postoperatively followed in our center, with some patients lost to follow-up, there may be missing data.
Comparing cases with and without remission in the medium term, cases of remission frequently involved adenomas >20 mm and less cavernous sinus invasion. Additionally, cases that achieved medium-term remission showed long-term remission more frequently. In the long term, those showing remission had less cavernous sinus invasion and residual tumors compared to those without remission. Therefore, we may conclude that a tumor size of 20 mm may predict medium-term remission, while the absence of/less cavernous sinus invasion, early remission, and absence of residual tumor may predict long-term remission.
This study had limitations. First, the retrospective nature of the study and the limited number of cases, which was inevitable due to the low incidence of CD, may have distorted our results. Although the same neurosurgical team operated on all patients, they were followed up pre and postoperatively at different endocrinology centers, causing difficulty in obtaining the full postoperative data of certain cases. Lastly, some patients recently underwent ETSS; thus, they had a shorter follow-up period. However, we intend to present the longer-term outcomes of all patients in a separate study.
Although ETSS is the first-line treatment for CD, previous studies on the use of ETSS for CD have reported a wide range of remission and recurrence rates, which can be primarily attributed to differences in the surgical experience levels among centers. This trend highlights the need for additional data from experienced centers to resolve the discrepancies in the existing data. Therefore, we present medium- and long-term follow-up data from 96 operations for CD conducted in a center with a high level of experience for ETSS. We believe our study makes a significant contribution to the literature because the findings reconfirm the usefulness of ETSS for the treatment of CD and highlight the importance of the size of the adenoma and presence/absence of cavernous sinus invasion on preoperative MRI in predicting long-term remission postoperatively.
CONCLUSION
ETSS is a safe and effective method for the treatment of CD. Some characteristics of adenomas, such as size, cavernous sinus invasion, and postoperative residue, may predict long-term remission. A tumor size of 2 cm may be a supporting criterion for predicting remission status in the presence of complete cavernous sinus infiltration. Further studies with larger patient populations are necessary to support this finding.