INTRODUCTION
Post-stroke shoulder pain (PSSP) is a common complication found in stroke patients and is a major cause of disability after stroke [1]. PSSP causes severe pain and hinders post stroke patientsŌĆÖ rehabilitation and quality of life (QoL) [2]. Therefore, effective control of PSSP is important when considering the prognosis in stroke patients. However, the treatment of PSSP is limited, even though treatment modalities have improved. Several treatment modalities, such as slings, positioning, strapping, functional electrical stimulation (FES), and nerve blocks have been suggested in the literature; however, evidence of evaluating their effectiveness in preventing or managing PSSP is still lacking [5].
Pulsed radiofrequency (PRF) is a novel therapeutic modality with potential applications in pain management. Several studies have reported favorable outcomes of PRF neuromodulation for chronic shoulder pain [7]. However, few studies have reported the clinical efficacy of PRF neuromodulation for PSSP patients. Our study aimed to evaluate the clinical efficacy of PRF neuromodulation on the suprascapular nerve in patients with PSSP after hemorrhagic stroke, with a minimum follow-up period of 12 months.
MATERIALS AND METHODS
The Institutional Review Board (IRB) of Chuncheon Sacred Heart Hospital approved this study (IRB No. 2021-06-006), and written informed consent was obtained from all patients. All experiments in this study were performed following the tenants of the Declaration of Helsinki.
Patient selection criteria
From March 2013 to March 2021, 2825 patients were diagnosed with a hemorrhagic stroke at our institute. Among them, 693 patients were diagnosed with PSSP based on the criteria shown in Table 1 [29].
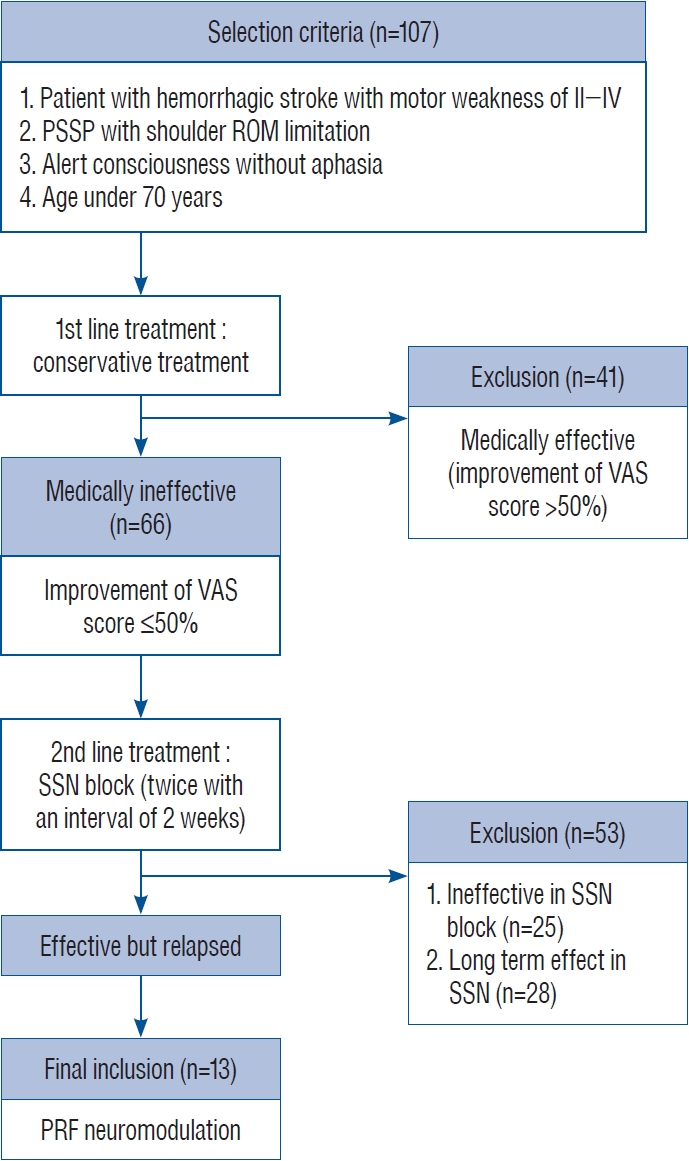
Patients were recruited for the study and PRF neuromodulation based on the selection criteria outlined in Fig. 1. All selected patients had a history of hemorrhagic stroke with motor weakness of grade II-IV, VAS of Ōēź6 points, shoulder range of motion (ROM) limitation, and alert consciousness without aphasia, and age under 70 years. Prior to PRF neuromodulation, all patients underwent conservative treatment, including medication (e.g., nonsteroidal anti-inflammatory drugs) and physical therapy. A nerve block, using 1.0% lidocaine and dexamethasone, was performed twice at a 2-week interval. A positive response to the nerve block indicated an improvement in the shoulder ROM or reduction of pain by more than 50%. Among those eligible for suprascapular nerve block, PRF neuromodulation was performed for patients whose symptoms worsened again within 2 weeks. Thirteen patients with hemorrhagic stroke with PSSP underwent PRF neuromodulation on the suprascapular nerve.
PRF procedure
Patients received either ultrasonography-guided or fluoroscopy-guided PRF stimulation. The procedure was conducted arbitrarily according to the condition of the equipment at that time. Among the 13 patients, eight received ultrasonography-guided PRF and five were treated with fluoroscopy-guided PRF. To locate the spine of the scapula, a line was drawn from the acromion tip to the medial border of the scapula. The center of the line was identified, and a perpendicular line parallel to the vertebral column was drawn through it. The entry point was marked 2 cm cranial and 2 cm medial to the spine of the scapula. The superior border of the scapula was aseptically draped.
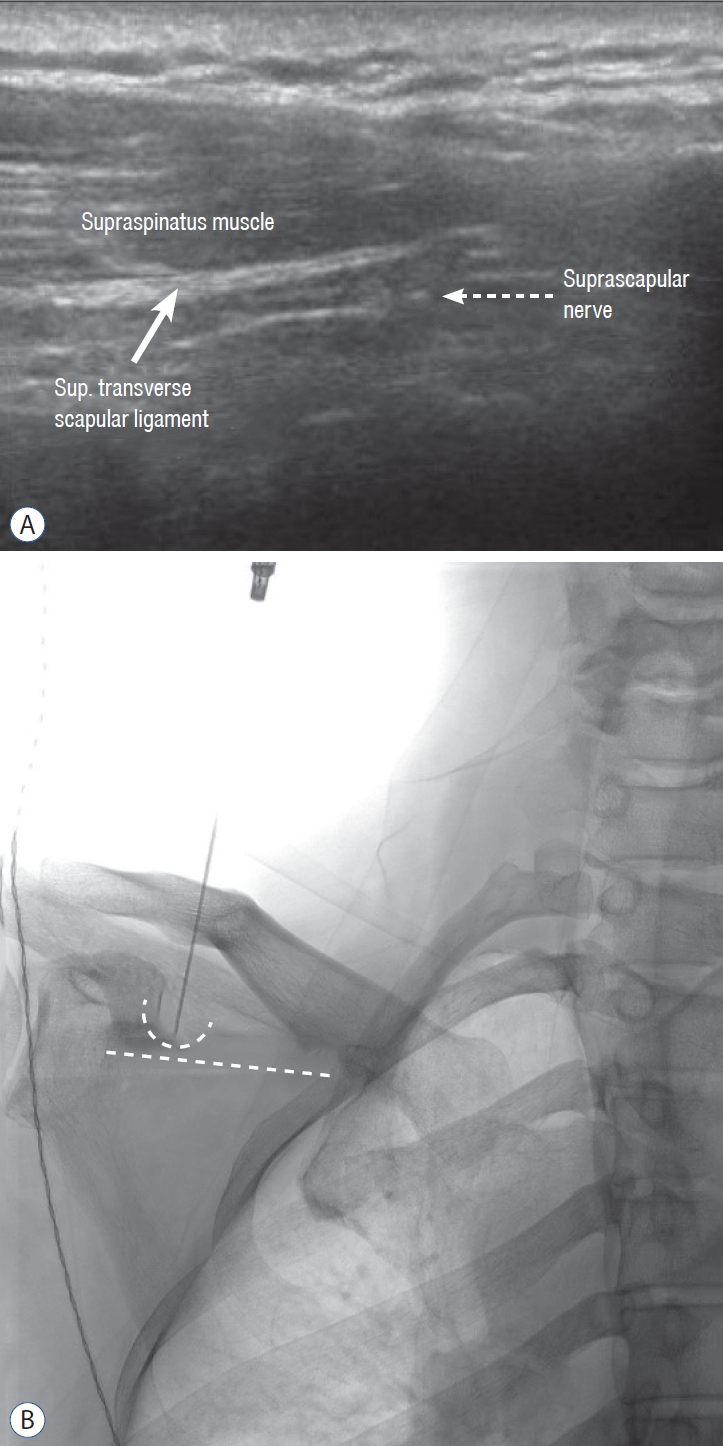
For ultrasonography-guided PRF the suprascapular notch, situated just medial to the base of the coracoid process and representing the superior border of the scapula, was identified using ultrasonography (Fig. 2A). The needle was inserted following the out-of-plane technique. In the case of fluoroscopy-guided PRF, fluoroscopy was angled caudal and oblique by approximately 10┬░ to 20┬░, and the position of the needle tip was adjusted by comparing it with the suprascapular notch (Fig. 2B).
PRF neuromodulation was performed using a Cosman G4 radiofrequency generator (Cosman Inc., Burlington, MA, USA) in the neurointervention room. A radiofrequency cannula (disposable 22-gauge) with an active tip (5-mm) was used. After inserting the radiofrequency cannula, the stylet was removed, and the RF electrode (Diros OWL RF cannula; Diros Technology, Inc., Markham, Canada) was inserted. Once the cannula tip was positioned on the suprascapular notch, sensory stimulation at 50 Hz was conducted. Temporary paresthesia in the shoulder joint was observed at stimulation below 0.3 volts (V). Motor stimulation was performed at 2 Hz. Abduction and external rotation (supraspinatus and infraspinatus muscles) appeared at a stimulation below 0.4 V. After a positive stimulation, PRF neuromodulation was conducted for 240 pulses at 45 V, keeping the needle temperature below 42┬░C. After PRF stimulation, the local anesthetic (4 mL of 1% lidocaine) was administered through the cannula to alleviate procedure-related pain. Patients were discharged if no complications such as pneumothorax and bleeding, occurred.
Outcome evaluation
Primary outcome
The same physician assessed the pain before PRF neuromodulation, immediately after PRF neuromodulation, and every 3 months after until the last follow-up visit. The primary outcome measurement was the Visual analog scale (VAS) score (0, no pain; 10, worst possible pain imaginable).
Secondary outcome
Secondary outcome measurements included shoulder ROM, Disability assessment scale (DAS), modified Ashworth scale (mAS), modified Rankin scale (mRS), and EuroQol-5 dimension-3L questionnaire (EQ-5D-3L) scores. The same physician assessed shoulder flexion, extension, and abduction ROM. DAS evaluated functional disability in areas such as patient hygiene, dressing, limb position, and pain [6]. The mAS measured shoulder adductor muscle tone. This 5-point score grades resistance to rapid passive stretch from 0 (no muscle tone increase) to 4 (rigid joint) [23]. The mRS quantified the degree of disability or dependence in the daily activities of individuals with neurological disabilities by seven grades [26]. QoL was evaluated using the EQ-5D-3L from 0 (worst health state) to 100 (best health state) [9].
RESULTS
Six men (mean age, 52 years) and seven women (mean age, 61 years) were enrolled for PRF neuromodulation. The mean age of the entire group was 56 years (range, 37-85), and the mean follow-up period was 54 months. The mean duration of symptoms was 13.69 months. During the follow-up period, the pre-PRF VAS score decreased by more than 50% in comparison to the VAS score at 1 year after PRF in 10 out of 13 patients. Although some patients reported recurrent pain, the overall VAS score showed a decline. Baseline shoulder magnetic resonance imaging and shoulder radiography were conducted for all patients. Among them, five patients had rotator cuff tears, and three patients had adhesive capsulitis. Patient demographics are summarized in Table 2.
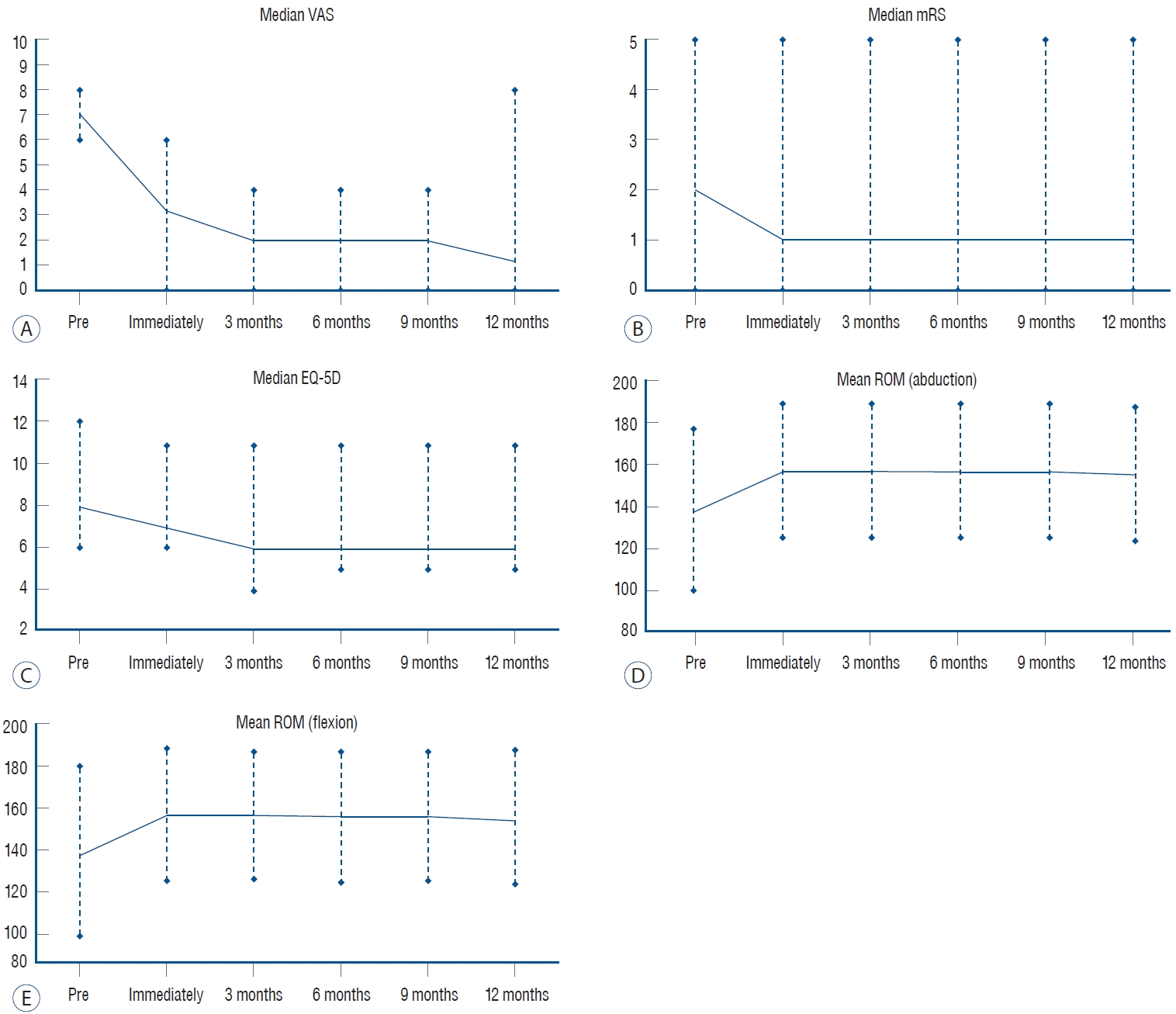
The mean VAS score was 7.08 points before PRF neuromodulation, and significantly decreased to 2.38 points immediately after the procedure (median value 7 to 3). Improvement was observed in the following parameters compared to baseline : VAS (median value, 7 to 3 immediately after PRF, p=0.001; 7 to 1 at 1 year after PRF, p=0.002); mRS (median value, 2 to 1 at 1 year after PRF, p=0.0047); DAS for pain (median value, 2 to 1 immediately after PRF, p=0.002; 2 to 1 at 1 year after PRF, p=0.004); EQ-5D-3L (median value, 8 to 6 immediately after PRF, p=0.002; 8 to 6 at 1 at 1 year after PRF, p=0.003); shoulder ROM for abduction (mean value, 136.92 to 155.38 immediately after PRF, p=0.0352); and flexion (mean value, 137.69 to 156.92 immediately after PRF, p=0.02; 137.69 to 155.38 at 1 year after PRF, p=0.02). The changes in the values of significant statistical differences before and after procedure were plotted over time (Fig. 3). Tables 3-5 provide a summary of comparisons for outcome data and treatment effects at all follow-up time points.
No complications, such as pain, bleeding, pneumothorax, or nerve injury, occurred in any of the patients.
Case illustration
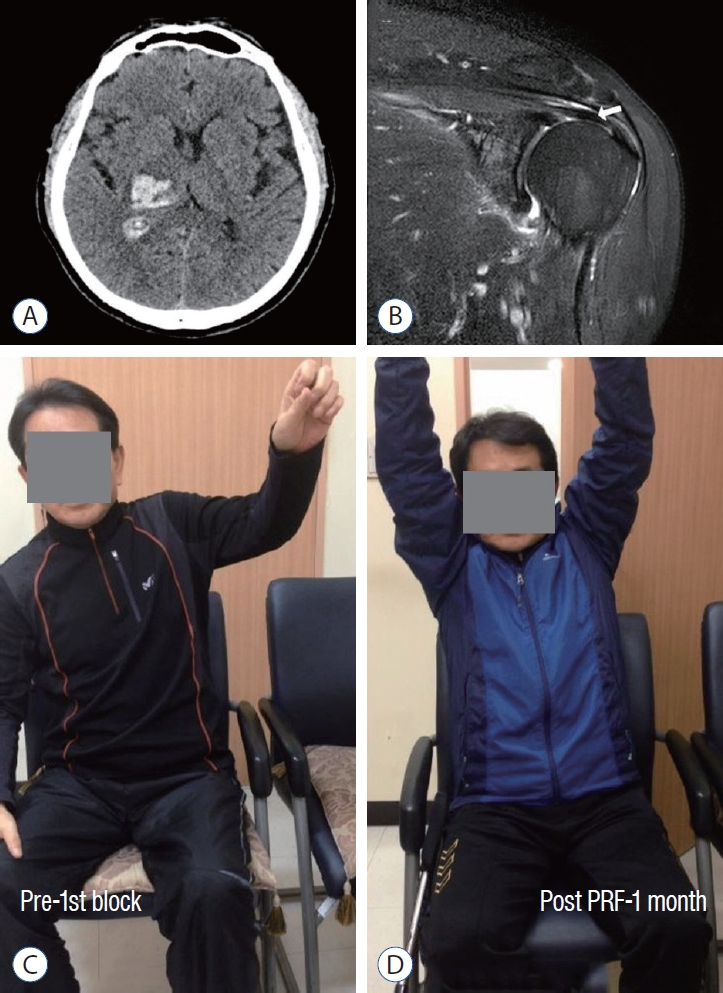
A 40-year-old patient presented to the emergency center in 2013 with left-sided motor weakness. Computed tomography reveled spontaneous intracerebral hemorrhage in the right thalamus (2.3├Ś2.6 cm2) (Fig. 4A). Clinical symptoms improved with conservative treatment, and at discharge, the patientŌĆÖs left upper extremity muscle strength was assessed as Medical Research Council grade 3. In the baseline shoulder imaging study, a focal tear in the supraspinatus tendon was confirmed (Fig. 4B). The patient reported intractable shoulder pain, limited ROM, and numbness. PRF was performed 9 months after intracranial hemorrhage with a diagnosis of PSSP. Pre-block shoulder flexion ROM was confirmed to be 140┬░ (Fig. 4C). Post-PRF shoulder flexion ROM was 180┬░ at 1 month after the procedure (Fig. 4D and Supplementary Videos 1 and 2). The VAS score improved from 8 points at baseline to 4 points at 1 year after PRF. Additionally, the EQ-5D-3L and mAS scores also showed improvement 1 year after PRF.
DISCUSSION
PSSP is commonly used to describe a set of complex problems with unknown causes Various factors have been suggested to explain the pathophysiological mechanisms of PSSP, including chronic regional pain syndrome type I (CRPS-I), altered sensitivity, rotator cuff tears, subluxation, and adhesive capsulitis [27]. Biomechanical factors significantly contribute and may occur in conjunction with changes in tone or neuropathic mechanisms. Ryerson and Levit [21] concluded that glenohumeral subluxation, CRPS-I, and orthopedic conditions (such as spasticity) might be responsible for PSSP. PSSP is one of the major complications and is observed in approximately 5-80% of stroke patients [24]. The loss of muscle strength due to hemiplegia can adversely affect the shoulder complex through three mechanisms : abnormal movement patterns, secondary changes to the surrounding soft tissue, and glenohumeral joint subluxation [5]. Recent studies have suggested that not only a musculoskeletal factor but also a neuropathic pain similar to central sensitization contribute to the disease [16]. Central sensitization modified the pain signal pathway leading to neuroplasticity [15]. Central post-stroke pain is also reported as one of the primary causes of PSSP [11].
Several techniques for the treatment of PSSP, including sling, positioning, strapping, FES, and nerve block are available; however, research evaluating their efficacy is limited [5,10,14,17,20]. Studies on the effects of conservative treatment on PSSP lack quantitative results. According to another study, a low rate of spontaneous pain resolution for PSSP (14% at 12 months) was observed [1]. Procedures such as suprascapular block, FES, and botulinum toxin administration have been reported to improve pain by 50-80%; however, the long-term effects have not been confirmed [3,17,20].
The procedure targeting the suprascapular nerve has been reported to reduce pain and improve the ROM in patients with shoulder pain, including those with rotator cuff lesions and frozen shoulder. The suprascapular nerve innervates the supraspinatus and infraspinatus muscles, providing 70% of the sensory signal of the shoulder joint [25]. Numerous targeted therapeutic procedures focus on the suprascapular nerve. Among these modalities, PRF neuromodulation has been shown to have long-term effects on various pain disorders [7]. PRF neuromodulation for the suprascapular nerve offers pain control without tissue destruction and subsequent sequelae in chronic shoulder pain [13]. Our study investigated the effect of PRF neuromodulation on the suprascapular nerve in patients with PSSP.
One of the crucial mechanisms of PSSP is the central and peripheral sensitization, where the transmission of pain signals in the peripheral and central nervous systems becomes overactive due to persistent shoulder pain [22]. Peripheral sensitization involves an increased sensitivity to afferent nerve signal [8]. Pain induces to the secretion of endogenous substances like serotonin, bradykinin, and potassium ions. These chemical mediators stimulate receptors on nociceptive terminals, affecting the depolarization threshold and modulating the excitability of nociceptor terminals [18]. Central sensitization is characterized by the overactivation of neurons in nociceptive pathways. The sustained pain signal eventually induces neuronal plasticity in the central nervous system, resulting in pain even from minimal sensory input [15]. PSSP is often considered a peripherally limited pain leading to a lack of response to conservative treatment. PRF stimulation is less effective in patients with central and peripheral sensitization. Efficient patient selection is paramount for successful PRF stimulation in PSSP. As presented in Fig. 1, PRF neuromodulation was performed on patients who tested positive for the suprascapular nerve block in our study. This screening block excludes central and peripheral sensitization from the patient population, thereby maximizing the effects of PRF stimulation.
Several other studies investigating PRF neuromodulation for PSSP, despite having different follow-up periods after the procedure (ranging from 16 weeks to 3 months), have consistently confirmed the sustained effect of PRF neuromodulation during the follow-up period [3,19,28]. Compared to previous studies, our study is important in that the follow-up time was at least 1 year which confirmed that PRF neuromodulation effects continued for 1 year.
As mentioned above, the loss of muscle strength contributes to shoulder joint instability, resulting in damage to surrounding connective tissues such as rotator cuff tears, tendinosis, and subluxation [5]. This, in turn, leads to shoulder stiffness, limiting the rehabilitation of the upper extremity. In our study, PRF neuromodulation immediately alleviated pain and improved the limitation in ROM after the procedure. This early relief facilitates prompt rehabilitation, a crucial factor for functional recovery. In our study, 69% of patients with PSSP exhibited a decrease in the mRS score one year after PRF neuromodulation. The mRS score at 1 year after PRF neuromodulation showed a 33% reduction compared to the baseline mRS (mean mRS, 2.31 vs. 1.54 points). In a previous prospective observational cohort study, it was reported that 34% of patients surviving hemorrhagic stroke experienced a 32% decrease in the mRS score between hospital discharge and the follow-up examination after 12 months (mean mRS score, 2 vs. 1.36 points) [12]. Notably, in our study, patients who underwent PRF neuromodulation demonstrated a greater improvement in disability compared to those with hemorrhagic stroke. The enhanced functional impairment through rehabilitation and pain relief appeared to have a significant impact of the QoL [4]. We attribute the favorable outcomes in the mRS in our study to the facilitated rehabilitation after PRF neuromodulation for PSSP.
This study had several limitations. First, it was retrospective and not a randomized controlled study. Second, the sample size was small (n=13). In our center, the neurosurgery department only managed patients with hemorrhage, not infarction. Therefore, only patients with hemorrhage were included in this study. Third, although the improvements in outcomes were maintained for 5 years post-procedure in most patients, statistical analysis on data beyond 1 year was not possible. Despite collecting data on outcome for more than 1 year, the data after 1 year were not consistently obtained. We followed up with patients regularly up to 3, 6, 9, and 12 months after PRF. After the last 12 months of outpatient treatment, the patient was asked to come to the hospital freely. Fourth, inclusion criteria were quite strict. In this study, patients who underwent PRF neuromodulation included a small proportion of patients diagnosed with PSSP. While performing PRF neuromodulation, it is necessary to confirm whether the target nerve has been correctly selected through conversation with the patient. This maximizes the effect of the procedure and reduces the possibility of damage to the surrounding tissues. Therefore, patients with poor communication capabilities due to old age, aphasia, and deterioration of consciousness were excluded. Randomized controlled studies with a larger sample size and longer follow-up period are required to support the clinical efficacy and long-term effect of PRF neuromodulation for PSSP in patients with hemorrhagic stroke.
CONCLUSION
PSSP is one of the major obstacles to the rehabilitation of patients with a hemorrhagic stroke. PRF neuromodulation targeting the suprascapular nerve not only achieves immediate and persistent pain relief, but with proper patient selection, also facilitates rehabilitation, enhances functional conditions and improves QoL. Moreover, it proves to be more efficient and safer than other treatments. The authors suggest that PRF neuromodulation targeting the suprascapular nerve could serve as an efficient modality for treating PSSP in patients with hemorrhagic stroke.