INTRODUCTION
Stroke is a condition that is not only of medical importance but also a major social and economic burden in Korea. Strokes are broadly divided into two types : ischemic and hemorrhagic strokes. According to stroke statistics in Korea, ischemic stroke accounts for approximately 70%, and hemorrhagic stroke accounts for 30% [23]. Interest in ischemic stroke treatment has increased over the past 30 years because ischemic stroke occurs more often and because of the dedicated efforts of neurologists. In 1995, the National Institute of Neurological Disorders and Stroke reported the usefulness of tissue-type plasminogen activator (tPA) and a ŌĆ£goldenŌĆØ treatment time in ischemic stroke [44]. However, extending the golden time of tPA and keeping the treatment within the golden time are major issues. Thus, the specific parameters of diagnosis, treatment, and management of ischemic stroke have been mainly investigated in analyses of acute stroke adequacy assessments. In the wake of the death of a nurse at a large hospital in Seoul in 2022, interest in the appropriate treatment for severe hemorrhagic stroke has increased in the medical community, as well as in the government. Hemorrhagic stroke has a lower incidence than ischemic stroke, but the 30-day mortality rate is about 2.41 times higher, and the average hospitalization cost is estimated to be about two times higher [23]. Thus, stroke treatments and support policies should focus on hemorrhagic stroke in consideration of its neurological severity. While achievements have been made in treating ischemic stroke, few efforts have been made to quickly and appropriately diagnose and treat patients with hemorrhagic stroke in Korea, in particular, those who live in rural and medically underserved areas, resulting in high mortality and morbidity. Hemorrhagic stroke can be classified based on the cause and location of occurrence, but it is generally divided into three types, including hypertensive intracerebral hemorrhage (ICH), subarachnoid hemorrhage (SAH), and other types of bleeding (e.g., arteriovenous malformation, hemorrhagic Moyamoya disease, and arteriovenous fistular bleeding). ICH and SAH have different treatment strategies. Thus, separate telemedicine protocols should be established. Since the incidence of ICH is 1.53-1.85 times higher than that of SAH in Korea [23], we decided to develop a telemedicine protocol for ICH in the rural and underserved areas in Gangwon state.
The incidence of ICH itself has tended to decrease, but mortality has still been high during the past decade [12,34]. Approximately 40% of ICH patients die within 30 days after ictus, and only 20% live independently at 6 months [1,24,27,38]. Therefore, rapid diagnosis and immediate, appropriate treatment are critical. Hematoma expansion is a well-known modifiable and independent risk factor for poor neurological outcomes. Because hematoma expansion usually occurs within the first 6-24 hours [7,33], properly inhibiting hematoma expansion in the acute phase is very important [35]. However, it is almost impossible to properly treat acute ICH patients in the emergency rooms of local hospitals in rural and underserved areas. Differences in regional medical infrastructures have resulted in clear regional disparities in cardiovascular mortality in Korea [25,29]. We previously reported the development of a system entitled ŌĆ£Cloud-based telemedicine platform exclusively for acute ICH patients in rural and underserved areas in Gangwon stateŌĆØ intended to reduce regional disparities in ICH treatment outcomes [27]. The core of the system is emergent, remote, non-face-to-face consultations with a neurosurgeon for doctors with less ICH expertise at local hospitals in rural and underserved areas. It is difficult to find emergency room doctors in Gangwon state. Under these circumstances, general doctors who lack ICH expertise have no choice but to take charge of patients with ICH. Accordingly, it is necessary to develop a telemedicine protocol for ICH exclusively for those doctors to enhance the quality of ICH treatment.
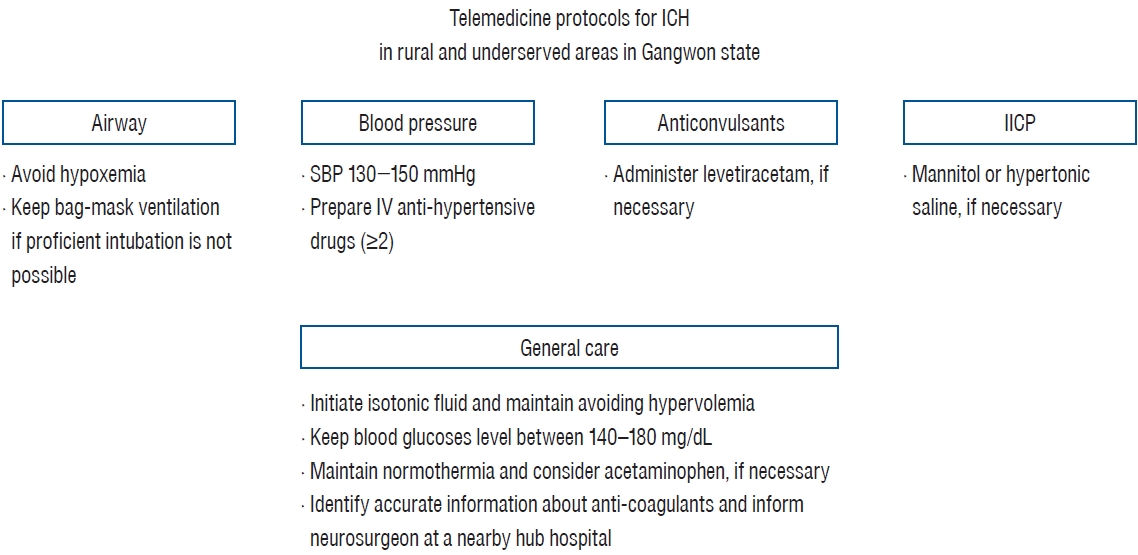
Clinical practice guidelines for ICH in Korea were reported after an intensive review of major published guidelines and literature [30]. Guidelines for the management of ICH were also released by the American Heart Association/American Stroke Association (AHA/ASA) in 2010 and 2022 [19]. These guidelines are generally applicable in circumstances where ICH patients can be treated by stroke specialists. However, doctors who are not familiar with these guidelines would probably treat these patients in rural and medically underserved area. In addition to the concept of treating ICH patients based on the cloud computing system that we reported previously [27], we aimed to establish a telemedicine protocol for ICH management exclusively for doctors with less ICH expertise in emergency rooms in rural and medically underserved areas. Four neurosurgeons (J.H.S., Y.K., K.J., and J.J.P.) working at university hospitals in Gangwon state reviewed important published ICH guidelines [19,30,49], and then suggested treatment protocols for real situations. We presented summaries of existing guidelines for ICH management and recommendations as simply as possible for issues involving airway management, blood pressure (BP) reduction, antiepileptic drugs (AEDs), increased intracranial pressure (IICP) management, and general care (Fig. 1). Anti-coagulation reversal is presented in the general care section of this protocol since the procedures are thought to be difficult to apply in rural and underserved areas, even though the 2022 ICH guidelines emphasized the use of anti-coagulation reversal [19].
AIRWAY MANAGEMENT
The first step of treatment is to observe and evaluate whether the airway and ventilation are working properly [9,10,47,48,57]. Patients with ICH often have breathing difficulties due to decreased consciousness caused by IICP. When IICP increases and autoregulation is damaged, hypoxemia develops, worsening cerebral edema. Accordingly, adequate oxygenation and ventilation are crucial in the acute period following ICH. How to manage airways and when to perform intubation are major concerns in emergency rooms in rural and medically underserved areas when ICH patients show decreased oxygen saturation levels. Proper airway managements in patients with ICH includes : 1) evaluating airway and ventilation properly while checking airway obstruction signs such as Cheyne-Stroke respiration; 2) ensuring adequate patient position. Patients are advised to keep their heads between 30 and 45 degrees to optimize venous outflow and reduce ICP, as well as to minimize the risk of aspiration. 3) Monitoring oxygenation and ventilation continuously. Once the airway is secured, oxygen saturation should be continuously monitored. If possible, checking end-tidal carbon dioxide is recommended for patients who received endotracheal tube placement [58]. 4) Maintaining adequate oxygenation with oxygen supplementation via a nasal cannula or face mask while avoiding hypoxemia, which is usually defined as arterial hemoglobin oxygen saturation (SaO2) of <90% or partial arterial oxygen pressure (PaO2) of <60 mmHg. And 5) considering endotracheal intubation if appropriate oxygen saturation cannot be maintained and proper ventilation is difficult due to reduced consciousness and oral secretions while transferring a patient with ICH to a nearby hub hospital with stroke specialists. Patients with Glasgow coma scale (GCS) scores of <8, unstable BP, or status epilepticus are likely to have airway compromise. Endotracheal intubation should be performed by an experienced doctor skillfully and quickly. The procedure sometimes requires rapid sequence intubation (RSI) with appropriate sedation and neuromuscular blockade [9,37,48,50,53]. If possible, an ultra-short-acting opioid such as fentanyl, alfentanil, or sufentanil, is considered to blunt the sudden ICP rise by adverse responses during RSI. Fentanyl given intravenously (IV) at a dose of 3 mcg/kg over 30 to 60 seconds can mitigate a sudden ICP rise without hypoventilation or respiratory depression. We suggest etomidate (0.3 mg/kg IV) as an induction agent for RSI, which is especially reasonable for patients with hypotensive conditions or risk for hypotension. Ketamine (1 to 2 mg/kg IV) can also be considered for normotensive or hypotensive patients. Succinylcholine (1.5 mg/kg IV), a neuromuscular blocking agent, can be used due to its rapid onset, consistent and reliable effects, and short duration of action. The abovementioned drugs are easily available at any local hospital in Gangwon state.
Few studies have investigated airway management exclusively for patients with spontaneous ICH compared to those with traumatic brain injury (TBI). Gravesteijn et al. [18] reported that in-hospital intubation led to better functional outcomes for TBI patients with GCS scores of Ōēż10 in an international pan-European cohort study. In contrast, the survival rate of TBI patients with GCS scores less than 9 and who received advanced life support did not differ significantly from those with basic life support (60.0% in advanced life support vs. 50.9% in basic life support; p=0.02) [50]. These conflicting results suggest that airway management by inexperienced doctors might be harmful to ICH patients with IICP. Thus, we recommend airway management for patients with ICH in rural and underserved areas as follows : 1) avoid hypoxemia to prevent further brain damage and aggravation of IICP and 2) if physicians at local hospitals lack the confidence to perform endotracheal intubation, bag-mask ventilation, which adequately oxygenates and ventilates, should be applied for most patients during transportation.
BP REDUCTION
Approximately 20-40% of patients were reported to experience hematoma expansion, which was closely associated with poor neurological outcomes [7,33,36]. Doctors tend to focus on lowering BP to prevent hematoma expansion in the acute period. When autoregulation is intact, cerebral perfusion pressure (CPP) is maintained by a mean arterial pressure (MAP) between 60 and 160 mmHg. When autoregulation is damaged due to IICP, lowered BP can worsen cerebral edema. Thus, CPP, ICP, and MAP parameters should be monitored for managing ICH adequately rather than relying only on BP monitoring. However, realistically, it is difficult to obtain data on such parameters in emergency rooms in rural and underserved areas. Thus, treatment goals are inevitably set around BP control. We reviewed three representative guidelines dealing with BP lowering for patients with ICH [19,30,49]. The most important principle is to reduce BP variability and maintain smooth and sustained control for mild-to-moderate ICH to prevent hematoma expansion and better functional outcomes (class of recommendation [COR], 2a; level of evidence [LOE], B-NR) (Supplementary Table 1). Specific recommendations for BP reduction differ slightly among the guidelines. For example, European Stroke Organization guidelines report that intensive BP reduction targeting a systolic pressure of <140 mmHg within 1 hour is safe and may be superior to targeting a systolic BP of <180 mmHg. However, the quality of the evidence was moderate, and the strength of the recommendation was weak [49]. Korean version of the guidelines, which is mainly based on those of the AHA/ASA [40], state that if the SBP is >200 mmHg or the MAP is >150 mmHg, then consider aggressive BP reduction with continuous intravenous infusion of drugs and frequent BP monitoring every 5 minutes [30]. And, if the SBP is >180 mmHg or MAP is >130 mmHg and there is any possibility of IICP, consider ICP monitoring and reducing BP using intermittent or continuous intravenous infusion while maintaining a CPP (MAP-ICP) of 50-70 mmHg [30]. Contrary to common belief, a sudden lowering of BP below 130 mmHg is potentially harmful to patients with mild-to-moderate ICH presenting with an SBP of >150 mmHg [19]. These differences in recommendations among the guidelines make it difficult for doctors with less ICH expertise working in rural and underserved areas to apply them properly. The goal of BP control is to balance the maintenance of adequate cerebral perfusion while minimizing the risk of hematoma expansion and further bleeding. Thus, we recommend : 1) achieving an SBP of 130-150 mmHg as soon as possible in the emergency room and 2) preparing two or more anti-hypertensive intravenous medications and using them appropriately based on the patientŌĆÖs clinical condition and degree of BP lowering. According to our telephone survey, labetalol, nicardipine, and hydralazine are available in emergency rooms at local hospitals in rural and underserved areas in Gangwon state. The appropriate dosage for each medication is as follows [30] : 1) labetalol : bolus dose of 5-20 mg every 15 minutes with an infusion rate of 2 mg/min (up to 300 mg/day); 2) nicardipine : bolus dose, no indication and an infusion rate of 5-15 mg/h; and 3) hydralazine : bolus dose of 5-20 mg, every 30 minutes and an infusion rate of 25-300 ┬Ąg/kg per minute.
AEDS USE
No large, prospective randomized controlled trials have been conducted on AED efficacy for post-ICH seizure, and there is a lack of established protocols. Several studies failed to prove any clinical benefit of AEDs for post-ICH seizures [15,41,45]. The 2022 ICH management guidelines recommend [19] : 1) that AEDs should be administered to reduce morbidity for ICH patients with impaired consciousness and confirmed electrographic seizures (COR, 1; LOE, C); 2) the use of AEDs to improve functional outcomes and prevent brain injury from prolonged recurrent seizures (COR, 1; LOE, C); 3) continuous monitoring with electroencephalography (EEG) (Ōēź24 hours) to diagnose electrographic seizures and epileptiform discharges for ICH patients with unexplained abnormal or fluctuating mental status or suspicion of seizures (COR, 2a; LOE, C); and 4) that prophylactic AEDs are not used to improve functional outcomes, long-term seizure control, or mortality (COR, 3; LOE, B). Continuous EEG monitoring for at least 24 hours is reasonable when ICH patients are suspected of having a seizure, are unconscious, or have consciousness fluctuations. Post-ICH seizures are classified into two groups : early and late seizures. Early seizures are related to direct structural brain damage by ICH with metabolic homeostasis and transient depolarization. Late seizures are thought to develop from neuronal reorganization with epileptogenic formation, which requires secondary prophylaxis [4,20,28]. About 28% of electrographic seizures were detected by at least 24 hours of continuous EEG monitoring [13]. Accordingly, AEDs are recommended to prevent repeated seizures, which lead to persistent brain injury and subsequent neurological outcomes in ICH patients with EEG evidence. Due to the conflicting results of the therapeutic effectiveness of prophylactic AEDs [43,54], they are not yet routinely recommended. Haapaniemi et al. [20] proposed a CAVE scoring system (0-4 points) based on cortical involvement (1 point), age younger less than 65 years (1 point), initial ICH volume more than 10 mL (1 point), and early seizures within 7 days after ICH (1 point) to predict the risk of late seizures following ICH. The rate of seizure risk was 0.6% for 0 points, 3.6% for 1 point, 9.8% for 2 points, 34.8% for 3 points, and 46.2% for 4 points. Thus, the risk predictions can be performed using CAVE scores to identify ICH patients who are likely to have late seizures. Limited centers in Gangwon state are equipped with 24-hour continuous EEG monitoring in the emergency room and have few specialists qualified in interpreting EEGs. Consequently, the administration of AEDs based on EEG monitoring is practically impossible. Our recommendations for using AEDs for ICH consider the potential risks and benefits of not using them in emergency rooms in rural and underserved areas. They are 1) ICH patient with deteriorated or fluctuations in consciousness levels; 2) computed tomography findings with evidence of herniation or imminent herniation and hematoma located within 1 mm from the cortex; and 3) an initial CAVE score of at least 2 points. The additional use and termination of AEDs are decided based on EEG monitoring at the transferred hub hospital. Finally, it is about which AED can be used in the clinical setting. The use of phenytoin is challenging since it requires periodic drug concentration analysis and subsequent dosage adjustments. Given the limited access to medical care in Gangwon state, using levetiracetam, which offers a predictable therapeutic range, can be more appropriate than phenytoin. Moreover, levetiracetam has the advantage of fewer drug interactions and allergic reactions, making it a safer option. The recommended dosing regimen is an initial loading dose of 1500-4000 mg over 15 minutes, followed by a bid dose of 500-750 mg.
IICP MANAGEMENT
Perihematomal edema tends to increase 24 to 72 hours after ICH, resulting in the aggravation of IICP. Thus, the timely administration of mannitol or hypertonic saline is perceived as critical by doctors [3,42,59]. Mannitol or hypertonic saline is considered the first-line therapy for managing IICP. Mannitol functions as an osmotic diuretic, effectively mitigating edema and reducing ICP by promoting water excretion by the kidneys. The administration of a 23.4% hypertonic saline bolus resulted in rapid ICP reduction [31], and the continuous infusion of 3% hypertonic saline while maintaining serum sodium levels of 145-150 mmol/L showed benefits in reducing cerebral edema and IICP [56]. The published guidelines suggest managing IICP by [19] 1) ventricular drainage for patients with ICH, intraventricular hemorrhage (IVH), and hydrocephalus that is contributing to decreased consciousness (COR, 1; LOE, B); 2) ICP monitoring and treatment might be considered for patients with moderate-to-severe ICH or IVH with reduced consciousness to decrease mortality and improve outcomes (COR, 2b; LOE, B); 3) the early use of prophylactic hyperosmolar agents for improving outcomes is not well established (COR, 2b; LOE, B); 4) bolus hyperosmolar therapy may be considered for transiently reducing ICP (COR, 2b; LOE, C); 5) corticosteroids should not be used for IICP control (COR, 3; LOE, B); 6) minimally invasive hematoma evacuation with endoscopic or stereotactic aspiration with or without thrombolytic use can help to reduce mortality from supratentorial ICH with volumes >20 to 30 mL and GCS scores of 5-12 (COR, 2a; LOE, B) compared to medical management alone; 7) decompressive craniectomy with or without hematoma evacuation may be considered to reduce mortality for patients with supratentorial ICH who are in a coma, have large hematomas with a significant midline shift, or significant IICP refractory to medical management (COR, 2b; LOE, C); 8) craniotomy for hematoma evacuation might be considered as a lifesaving measure for patients with supratentorial ICH who are deteriorating (COR, 2b; LOE, A); and 9) immediate surgical removal of the hematoma with or without extraventricular drainage is recommended over medical management alone to reduce mortality in patients with cerebellar ICHs with neurological deterioration, brainstem compression and/or hydrocephalus from ventricular obstruction, or a cerebellar ICH volume of Ōēź15 mL (COR, 1; LOE, B). Surgical treatments are impossible in emergency rooms in rural and underserved areas. Thus, it is important to know more about mannitol and hypertonic saline use. A recent meta-analysis reported that hypertonic saline exhibited significantly lower treatment failure and better ICP reduction and CPP maintenance 30-60 minutes after infusion in patients with TBI [11]. However, there were no significant differences in good neurological outcomes, mortality, or ICP and CPP 90-120 minutes after infusion [11]. Nevertheless, doctors still consider which agent is reasonable to control IICP in an emergent situation. We think that the choice should be made in consideration of the patientŌĆÖs medical history and potential risk of side effects. For instance, the bolus administration of mannitol or hypertonic saline is preferred to avoid volume overload in patients with congestive heart failure. Conversely, the continuous infusion of 3% hypertonic saline may be appropriate for dehydrated patients with ICH. Similarly, mannitol is relatively contraindicated for patients with chronic kidney disease due to its potential renal toxicity, rendering hypertonic saline a safer alternative [14]. The required volume of mannitol can be calculated using the following equation: total dosage of mannitol (mL of 20% mannitol) = (x + 31.17900 ├Ś y - 3.39853 ├Ś z - 244.47590) / 0.00752, where x is pretreatment ICP (mmH2O), y is the hematoma location (supratentorial ICH : y=0; infratentorial ICH : y=1), and z is the hematoma volume (mL) [52]. Typically, mannitol is administered as a bolus at a dosage ranging from 0.25 g/kg to 1 g/kg of body weight at intervals from 6 to 12 hours [51]. ICP reduction is observed within 1-5 minutes after administration and reaches a peak effect between 20 to 60 minutes [46]. Thus, we recommend administering mannitol or hypertonic saline for ICH patients with decreased consciousness and evidence of IICP.
GENERAL CARES
General care refers to issues, such as intravenous fluid selection, glucose control, body temperature maintenance, and the reversal of anti-coagulation. In particular, the 2022 ICH guidelines updated and highlighted recommendations for anti-coagulation reversal [19]. However, appropriate reversal is almost impossible in emergency rooms in rural and underserved areas. Thus, the relevant materials are explained at the bottom of this section. We tried to summarize general care in previous guidelines with as high evidence levels as possible [19]. Then, we suggest recommendations with some modifications exclusively for ICH patients visiting emergency rooms in rural and undeserved areas.
Fluid choices usually deal with fluid volume, type of fluid, and the tonicity of maintenance fluids in neurocritical care settings [55]. Fluids for ICH patients in rural and underserved areas have received little attention. The selection and maintenance of fluid is quite complex and requires many considerations. Fluid administration itself can affect tonicity and volume status, possibly resulting in a degree of cerebral edema, cerebral blood flow, and oxygenation via complex responses with blood-brain barrier disruption, cerebrospinal fluid circulation, inflammation, venous impedance, and systemic circulation [55]. Contemporary recommendations for fluid management were derived from patients with SAH, not ICH. The maintenance of euvolemia and normal circulating volume is recommended to prevent delayed cerebral ischemia in SAH (COR, 2a; LOE, B-NR) [22]. Isotonic fluid is usually used for maintenance, while colloids are not routinely recommended [55]. However, these findings only address fluid maintenance in the intensive care unit, not optimal fluid maintenance in the emergency room. Since our protocol is for ICH patients in rural and underserved areas, isotonic saline should be used and maintained without establishing hypervolemia (e.g., 0.9% normal saline at a rate of approximately 1 mL/kg/h) in the emergency room before transferring the patient to a nearby hub hospital. After transfer, volume status, electrolyte imbalance, and serum osmolality should be assessed altogether to determine fluid and infusion rates.
A previous study did not demonstrate an association between admission glucose levels and neurological outcomes after adjusting for age, neurological scores, and hematoma volume [32]. However, a meta-analysis revealed a harmful effect of high glucose levels on neurological outcomes following ICH [60]. The recommendation for glucose control are as follows : 1) monitoring serum glucose levels to avoid hyperglycemia and hypoglycemia in patients with ICH and 2) treating hypoglycemia in patients with glucose levels less than 40-60 mg/ dL or 2.2-3.3 mmol/L to reduce mortality after ICH (COR, 1; LOE, B-R) [19]. Fever is common following ICH, and about 20% of the patients experienced systemic inflammatory response syndrome during hospitalization [6]. In the ICU setting, pharmacologically treating an elevated temperature may improve functional outcomes (COR, 2b; LOE, C-LD). However, therapeutic hypothermia targeting less than 35┬░C or 95┬░F to decrease peri-hematoma edema (COR, 2b; LOE, C-LD) is not routinely recommended.
ICH patients who received anti-coagulation therapy showed high mortality and morbidity. Fernando et al. [17] reported that oral anti-coagulation significantly increased the risk of in-hospital mortality (adjusted odds ratio, 1.37; 95% confidence interval [CI], 1.26-1.49) and 1-year mortality (hazard ratio, 1.18; 95% CI, 1.12-1.25) in adult patients. The 2002 ICH guidelines highlighted the use of prothrombin complex concentrate for the reversal of vitamin K antagonists, such as warfarin; idarucizumab for the reversal of the thrombin inhibitor dabigatran, and andexanet alfa for the reversal of factor Xa inhibitors, such as rivaroxaban, apixaban, and edoxaban [19]. More specifically, 4-factor prothrombin complex concentrate is recommended for patients with vitamin K antagonist-associated ICH and an international normalized ratio (INR) >2.0, rather than fresh-frozen plasma for rapid INR correction and the prevention of hematoma expansion (COR, 1; LOE, B-R). Andexanet-alfa is suitable to mitigate factor Xa inhibitors-associated anti-coagulant effect (COR, 2a; LOE, B-NR). Also, the administration of idarucizumab to offset the anti-coagulant effect by dabigatran is reasonable for dabigatran-associated ICH (COR, 2a; LOE, B-NR). Intravenous protamine is reasonable to offset the anti-coagulant effect (COR, 2a; LOE, C-LD) of unfractionated heparin-associated ICH [19]. However, as described above, anti-coagulation reversal is almost impossible in emergency rooms in rural and underserved areas. Rather, it is important to obtain exact information on which anti-coagulant was taken and deliver it to the stroke specialist in the nearby hub hospital to which the patient is transferred. We recommend general care for ICH patients as follows : 1) initiate isotonic fluid and maintain avoiding hypervolemia; 2) maintain blood glucose levels between 140-180 mg/dL [19]; 3) maintain normothermia and consider acetaminophen, if necessary [19]; and 4) identify accurate information on anti-coagulants and inform specialists at hospitals receiving transferred patients.
DISCUSSION
ICH requires timely diagnosis and treatment to mitigate brain damage. However, these procedures are inevitably delayed in patients with ICHs visiting emergency rooms in rural and medically underserved areas, particularly at night or early in the morning. Even if the diagnosis is made quickly, appropriate responses to prevent hematoma expansion, IICP control, and more are realistically difficult for doctors in charge of these local emergency rooms. The number of assistive devices using artificial intelligence (AI) for ICH diagnosis is increasing. However, their clinical value for timely early diagnosis is reduced unless AI is linked to timely and appropriate treatment. We believe that the only way to organically link diagnosis and treatment for ICH patients is through cloud-based remote consultation with neurosurgeons from nearby hub hospitals as a kind of telemedicine. Angileri et al. [2] reported on the rapid diagnosis of ICH patients using telemedicine-based neurosurgical consultation (38 minutes with telemedicine vs. 160 minutes without telemedicine). Thus, a cloud-based remote consultation system allows neurosurgeons to intervene appropriately right after ICH occurrence.
Having worked as doctors treating ICH for over 20 years, we realized that a cloud-based consultation system requires an organized treatment protocol exclusively for ICH patients in local emergency rooms in rural and underserved areas. Although the consultation is carried out by ICH experts, there may be some differences depending on each neurosurgeonŌĆÖs knowledge and experience. Thus, it was necessary to develop a standardized common protocol based on clinical evidence and apply the standardized protocol in real clinical practice for the critical management of ICH.
Our protocols should include tailored modification to provide more specific recommendations based on hemorrhagic characteristics because ICH and SAH have different features, such as anatomical location of bleeding, cause, and prognosis. Thus, we plan to develop additional standardized protocols for SAH patients in the near future. Additionally, we plan to upgrade the current ICH protocols, including the amount of hemorrhage, location, IICP degree, and choice of treatment method (surgery vs. conservative). It is not necessary to transfer all patients with ICH to nearby hub hospitals for efficient medical delivery and use of medical resources. Accordingly, more specific recommendations for classifying ICH severity based on requirements for surgical treatment or intensive care management should be included.
With advances in wireless communication technologies, the combination of telemedicine and cloud computing has been increasingly used in the medical field [26]. Our ICH protocols are designed for application in cloud-based remote consultations covering various hospitals across the Gangwon state. Currently, electronic health records (EHRs) are usually implemented in a centralized server cluster in each hospital. Thus, building separate EHR connections between local servers and the centralized datacenters of nearby hub hospitals requires substantial funds [26]. Sharing patient information can be possible with cloud computing at a relatively low cost since there is no need to build separate connections between the participating hospitals. Also, the system can be operated regardless of the location of doctors as it is accessed via a web application. However, cloud-based telemedicine systems can be frequent targets for hackers seeking to illegally access personal and medical information. Accordingly, security technologies should be strengthened and upgraded along with the development of an ICH management protocol. Each telemedicine system must have a secure module to encrypt patient treatment information and transmit the encrypted information using secure data transmission protocols. Hospitals involved in cloud-based telemedicine systems can form a safe cluster using effective security technologies, such as blockchain and safely manage patient treatment information together in the future.
AED use is frequently performed in actual medical settings, regardless of the ICH guidelines. Post-stroke seizures, including ICH, have led to increased mortality and longer hospitalization [8,16]. About 12% of patients were estimated to experience seizures after ICH [39]. However, the therapeutic effect of AEDs on post-ICH seizures is still somewhat controversial [15,41,45]. A current meta-analysis and guidelines since 2015 [15] recommended against the routine use of prophylactic AEDs. However, about 40% of patients receive AED prophylactically. Our protocol is aimed at treating ICH patients at local emergency rooms in rural and medically underserved areas and mainly minimizes complications until they are transferred to a nearby hub hospital with a stroke specialist. Thus, we recommend using the AED levetiracetam, considering the potential benefits and harms in such circumstances.
Although we propose a telemedicine protocol for acute ICH in rural and underserved areas for the first time, two important things should be kept in mind. One is CPP and the other is neurological examination. Maintaining BP well is ultimately to maintain CPP at an appropriate level. When mannitol or hypertonic saline is administered to decrease ICP in patients with low CPP or impaired autoregulation, it may cause hypovolemic status of circulating volume, resulting in aggravation of ischemic damage. Accordingly, the patientŌĆÖs current volume status should be monitored to maintain appropriate BP and CPP. Neurological examination is an important factor in predicting the degree of ICP and evaluating brain damage in addition to imaging information. Detection of papilledema and 6th cranial nerve palsy can be used as reliable parameters to assess IICP at local emergency rooms. Since brainstem is prone to primary and secondary injuries, characterization of brainstem reflex can reveal the extent of brain dysfunction and damage [5]. The brainstem reflex includes pupillary light, cilio-spinal, fronto-orbicular, oculo-cephalic, oculo-vestibular, corneal, cough, gag and oculo-cardiac responses. In the emergent care setting, examination of cranial nerves III, V, VII, and IX using pupillary light reflex, corneal reflex, and cough reflex seems to be used more frequently. Nevertheless, future discussions are needed on which of these various reflexes to use initially at local emergency rooms in rural and underserved areas. Also, there is a need to discuss specific methods to accurately determine the hemodynamic status of patients with ICH mentioned above. This protocol will first be carried out in collaboration with neurosurgeons from four university hospitals in Gangwon state, and if necessary, video calls linked to the cloud system will be used. Therefore, we plan to discuss useful methods for evaluating the neurological and hemodynamic status of patients while operating the system based on the protocol we propose.
The medical infrastructure in Gangwon state is poor, and there are clear regional differences. According to the Health Insurance Review and Assessment Service [21], most medical institutions are located in the three cities of Wonju (n=665), Chuncheon (n=495), and Gangneung (n=359). Goseong and Yangyang do not have medical institutions with inpatient beds. Hwacheon, Pyeongchang, and Inje have fewer than 50 inpatient beds per 10000 people, indicating a shortage of inpatient beds per resident. We believe that our proposed telemedicine protocols will be helpful in managing patients with acute ICH across the Gangwon state. The cloud-based ICH management system, which we are currently developing, should not be limited to simple diagnosis and treatment. It should be linked to risk prediction (e.g., high probability of poor neurological outcomes and medical complications) and chronic management. To achieve these goals, first, a biobank of patient blood samples must be constructed, and simultaneously, human clinical research and basic in vivo and in vitro research studies must be conducted. Then, the research results should be used for the early diagnosis of at-risk patients in real neurocritical care units. In addition to this, when post-ICH survivors return to their area of residence, metabolic diseases, including risk factors for stroke, should be managed to prevent ICH recurrence, improve cognitive function and achieve rehabilitation through various web applications. The establishment of these integrated systems will ultimately become the cornerstone of improving the quality of medical care and life for ICH patients in Gangwon state.
CONCLUSION
Our protocol aims to provide guidelines for ICH management exclusively for doctors at local emergency rooms in rural and underserved areas, allowing doctors with less ICH expertise to treat ICH with more certainty. The Gangwon State Neurosurgery Consortium has been developing a cloud-based telemedicine platform for patients with acute ICH. The protocols we developed will be embedded into this system and applied in clinical use soon. The dedication of neurosurgeons in using the telemedicine protocols will ultimately improve the quality of ICH treatment across Gangwon state.