INTRODUCTION
Entrapment of the sciatic nerve at its exit from the greater sciatic foramen has long been known by the elusive name of “piriformis syndrome”. Piriformis syndrome is defined simply as a non-discogenic cause of sciatica due to sciatic nerve impingement through or around the piriformis muscle [5,9]. Although first described in 1928 and coined in 1947 [27,37], the precise pathophysiology of piriformis syndrome is still not defined. It is still regarded as a controversial but potentially common [4,13], underdiagnosed cause of buttock pain and non-discogenic cause of sciatica [7,10,14,22,24,28], and even a cause of failed back surgery syndrome [6,15,30].
The diagnosis of so-called piriformis syndrome is complicated by multiple differential diagnoses of low back and buttock pain with many diagnoses associated with overlapping symptoms [25]. Its existence has even been questioned due to the lack of objective testing, reliable effective treatment, or reasonable pathophysiology associated with the condition [29]. However, sciatic nerve entrapment has been consistently emphasized as an extra-spinal cause of sciatica [4,7,10,13,14,22,24,28]. The risk of misdiagnosis is reduced in patients presenting with so-called, lumbar spine magnetic resonance imaging (MRI)-negative sciatica, but it is elevated in cases of MRI-positive sciatica [15,30]. With the increase in the frequency of degenerative lumbar spine disease due to aging, the frequency of spine surgery and the incidence of failed back surgery syndrome are increasing in the general population [6,15,30]. A report by Filler et al. [9] confirmed that 46% of 239 patients in the piriformis syndrome cohort had undergone previously ineffective spinal surgery.
Surgical treatment, open or endoscopic decompression of the sciatic nerve, is recommended for patients with persistent or recurrent symptoms after conservative treatment or for those carrying mass lesions compressing the sciatic nerve [4,9,23,25].The transgluteal approach has been used as a direct strategy for sciatic and pudendal nerve entrapment and several technical modifications have been reported [9,12,16,17,19,20,26,31,34,36]. The transgluteal approach may be similar to division of the gluteal muscle; however, the posterior hip joint approach in the lateral decubitus position has been designated as the transgluteal approach in orthopedic surgery [16,17,19,20,36]. I adopted the concept of minimally invasive transgluteal approach proposed by Filler et al. [9] to reduce the size and morbidity associated with incision [15,30,31,32,34].
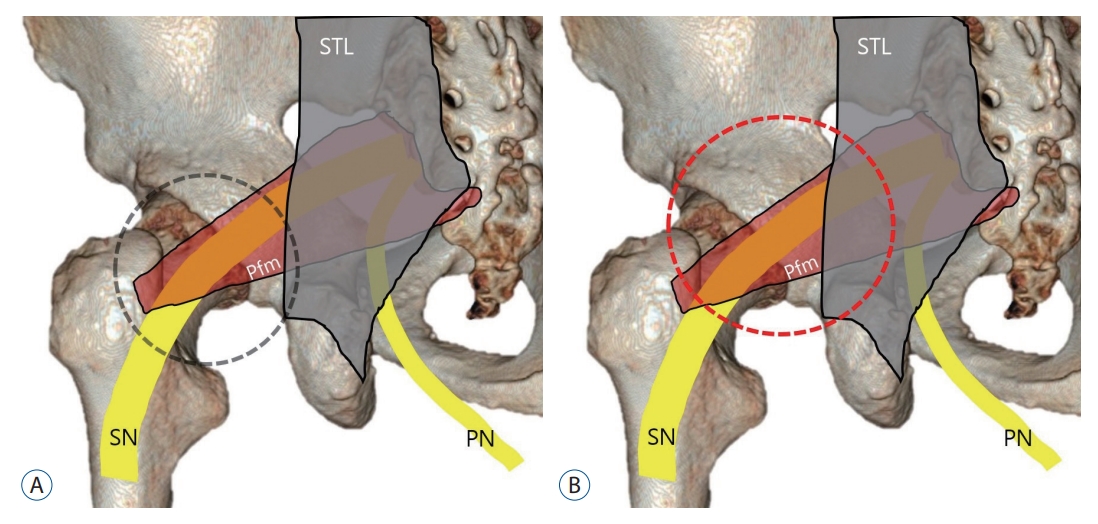
As my experience with the transgluteal approach to sciatic nerve entrapment increased, I also experienced recurrences due to postoperative adhesion and failure. During the revision surgery for postoperative adhesion, further circumferential dissection of the nerve was performed and the importance of the sacrotuberous ligament was realized [34]. During revision surgeries, the sacrotuberous ligament located above the piriformis muscle in the subgluteal space and the stump of the resected piriformis muscle were found to form a kind of compartment around the nerve [34]. Therefore, transgluteal decompression technique performed since 2021 utilized a modified the resection of the piriformis muscle encircling the sciatic nerve via additional opening of the portion of the sacrotuberous ligament attached to the piriformis muscle (Fig. 1) [34].
Accordingly, the factors affecting the pain outcome of transgluteal decompression in sciatic nerve entrapment were analyzed. In particular, the effects of circumferential dissection of the course of the sciatic nerve, including partial resection of the sacrotuberous ligament, were analyzed.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (#2023-1673-0001).
Inclusion criteria
I retrospectively studied the medical records of 104 patients who had undergone sciatic nerve decompression via transgluteal approach to alleviate sciatica of chronic sciatic nerve entrapment over the past 10 years (2013-2022). Sciatic nerve decompression was performed by a single surgeon (B.S.) at a single institute. The results of surgery for pain outcome were confirmed in 85 of these patients by following them for at least 6 months. In this study four of the 85 patients who underwent sciatic nerve decompression, four were excluded because they underwent surgery for weakness of the lower extremities and not for pain due to sciatica.
The demographic data of patients in the current study are summarized in Table 1. My diagnostic criterion for sciatic nerve entrapment was sciatica and absence of lumbar pathology underlying the symptoms in patients with unresolved sciatica. Clinical symptoms included sitting pain or sitting intolerance. Temporary improvement of existing sciatica was confirmed with local anesthetic blockade of the piriformis muscle or sciatic nerve. Patients who had primarily hip and back pain but did not present with sciatica were not diagnosed with sciatic nerve entrapment.
To exclude lumbosacral nerve root lesions causing sciatica, X-rays of the lumbar spine and pelvic bone and computed tomography and MRI of the lumbar spine were performed in all patients suspected with sciatic nerve entrapment. Electromyography and nerve conduction studies were also performed in all patients, but negative and lumbosacral radiculopathy findings were interpreted for reference only. Therefore, my indications for surgery were based on clinical findings, medical intractability, and response to piriformis and sciatic nerve blocks. Patients who no longer needed surgical treatment because of symptoms improvement with medication, physical therapy, or piriform muscle injection were excluded. Cases with hip pathology causing pelvic and hip pain, such as sciatic bursitis, calcific tendinitis, degenerative or adhesive arthritis of the hip, and femoral acetabular impingement syndrome, were also excluded.
Decompression of the sciatic nerve was performed if the buttock pain and sciatica was not relieved within 6 months of medical and physical treatment and repeated injections of the piriformis muscle and treatment with sciatic nerve blocks. MRI of the pelvic bone was performed in all patients to investigate the variation between sciatic nerve and piriformis muscle and possible intrapelvic pathologies encroaching the lumbosacral plexus, except for patients with implanted spinal cord stimulators.
Demographics
Of the 81 patients, 47 were females (58.0%) and 34 were males (42.0%). The mean age of the patients with sciatic nerve decompression was 54.4±14.2 years (mean±standard deviation [SD]; n=81; range, 12-78 years) and the duration of sciatica was 68.4±132.31 months (mean±SD; range, 9-192 months). The preoperative numerical rating scale-11 (NRS-11) score was 6.43±0.97 (mean±SD; range, 4-8).
As an anatomical variation of the sciatic nerve and piriformis muscle, types A and B were significantly prevalent (type A : 49 of 81 [60.5%] and type B : 30 of 81 [37.0%], respectively), but type C was rare (two of 81 [2.5%]). Sciatic nerve entrapment was primary in 72 patients (89.0%), and secondary sciatic neuropathy was found in eight patients (11.0%) due to pelvic fracture, traumatic hematoma of the gluteus maximus muscle, and perineural ganglion cysts. Seventy patients (86.4%) had unilateral decompression and 11 patients (13.6%) underwent staged, bilateral surgery. Of the 70 patients who had unilateral surgery, 34 (42.0%) had surgery on the right side, whereas 36 patients (44.4%) had surgery on the left side. Twenty-eight patients (34.6%) presented with refractory sciatica that was not controlled with spinal surgery. During sciatic nerve decompression, the lateral edge of the sacroiliac ligament was additionally resected in 34 cases (42.0%).
All patients were referred for medical intractability as they did not improve for a long time despite medical treatments such as nonsteroidal anti-inflammatory drugs, gabapentinoids, and opioids, physical therapy, repeated epidural and root blocks, and piriform muscle injections. In fact, most of these patients’ sciatica was diagnosed as being caused by degenerative lumbar spine disease and 28 patients (34.6%) visited our clinic for the treatment of failed back surgery syndrome. One patient with sudden-onset, MRI-negative sciatica was referred 3 years after receiving spinal cord stimulation (SCS) with a diagnosis of complex regional pain syndrome type I. The patients’ demographics are summarized in Table 1.
Assessment of outcomes
To determine the overall pain improvement following sciatic nerve decompression, the severity of pain was assessed before surgery and at the 12-month follow-up after surgery, using the NRS-11 (0-10; 0, no pain; 10, the worst pain imaginable). The changes in sciatic pain were measured as percent (%) pain relief; [1 - (NRS-11 score at the 12-month follow-up / NRS-11 score before operation)] × 100. Successful sciatic nerve decompression was defined by a reduction of at least 50% pain measured by NRS-11 during the 12-month follow up. The degree of subjective satisfaction was assessed at the last follow-up using the Likert scale, with a score of 1 reflecting no pain relief at all and a score of 10 suggesting complete relief of target symptoms.
In addition, factors that may influence surgical success were investigated, including age, sex, duration of pain, laterality of pain, bilateral presentation, type of anatomical variations between the sciatic nerve and piriformis muscle, history of spinal surgery before decompression, and an additional sacrotuberous ligament incision directly related to surgical technique. Modification in drug regimens was not controlled during our study.
Statistical analysis
A paired t-test was used to compare the relationship between preoperative and postoperative NRS-11 scores and percent pain relief following sciatic nerve decompression. An independent sample t-test was used to compare the means between the groups with and without sacrotuberous ligament resection. All statistical analyses were performed with SPSS version 22.0 (IBM SPSS Statistics, Chicago, IL, USA). The values were considered statistically significant when p<0.05.
Decompression of the sciatic nerve
My technique of transgluteal decompression of the sciatic nerve has already been reported in detail [30-34]. The surgery was performed under a microscope with the patient in the prone position under general anesthesia. Intraoperative neurophysiologic monitoring was performed in all cases to confirm the localization of the sciatic nerve and its branches and prevent nerve damage [34]. After making a lazy S-shaped incision with a length of about 8 to 10 cm, dissection of the gluteus maximus muscle along with the muscle texture was performed. For circumferential dissection of sciatic nerve at the greater sciatic notch, the lateral edge of the sacrotuberous ligament with attached gluteus maximus muscle was exposed [34]. When the subgluteal space was exposed along with the sacrotuberous ligament overlying the piriformis muscle, inferior gluteal nerve and blood vessels are identified in the subgluteal fat layer [34].
Before the introduction of sacrotuberous ligamentectomy (until 2020), the inferior gluteal nerve was first dissected within the fat layer below the sacrotuberous ligament, followed by the tibial and peroneal divisions of the sciatic nerve. However, after realizing the importance of the sacrotuberous ligament in the piriformis muscle resection, approximately 2 cm of the lateral margin of the sacrotuberous ligament to which the piriformis muscle was attached was first incised (Fig. 1B) [34]. The piriformis muscle compressing the sciatic nerve was exposed proximal to the greater sciatic notch (Fig. 2A and B). The sciatic nerve, identified via intraoperative nerve stimulation, was carefully separated from the piriformis muscle (Fig. 2C). The tibial and peroneal divisions of the sciatic nerve are then isolated from the piriformis muscle and tendon and were confirmed by intraoperative stimulation [34]. The piriformis muscle compressing the sciatic nerve and its division were gradually resected en bloc along the proximal to distal direction, using bipolar coagulation and cutting techniques (Fig. 2D and E). After removing the piriformis muscle and tendon, the inferior aspect of the exposed sciatic nerve was examined for adhesion to the greater sciatic notch (Fig. 2F). A caudal dissection of the tibial and peroneal nerves was performed down to the level of the lesser trochanter of the femur [34]. After securing circumferential dissection of the sciatic nerve and its branches with incision of the sacrtuberous ligament and resection of the piriformis muscle, a polytetrafluoroethylene film (Sepra film®; Baxter International, Chicago, IL, USA) was inserted around the nerve to avoid severe adhesion and scar formation. Meticulous bleeding control was performed. The patients were allowed to walk and sit the day after surgery.
RESULTS
Outcomes of sciatic nerve decompression
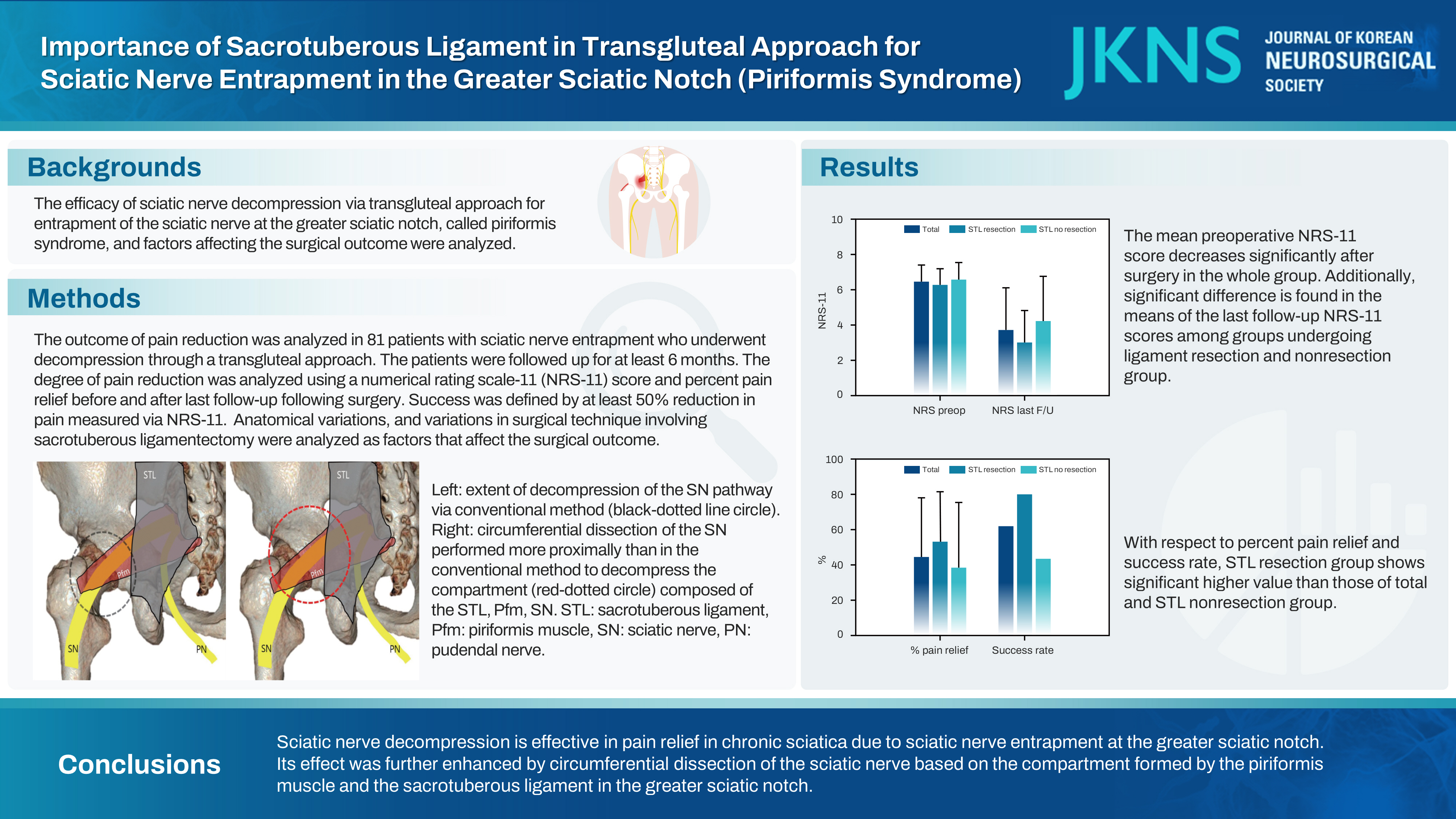
Tables 2 and 3 summarize the outcome of the sciatic nerve decompression and factors affecting the pain prognosis of sciatic nerve decompression. The mean preoperative NRS-11 score decreased significantly after surgery in the whole group (p<0.05, paired t-test; n=81). Percent pain relief was 43.9±34.17 (mean±SD; range, 0-100). According to the criteria for success, defined as 50% improvement in preoperative pain, decompression of the sciatic nerve was successful in 50 of 81 patients (61.7%) at 17.5±12.5 months of follow-up.
Sex, primary or secondary sciatic neuropathy, unilateral or bilateral symptoms, type A or type B variation, previous spinal surgery, prior pain surgery such as SCS or intrathecal morphine pump implantation were not associated with surgical success (p>0.05, chi-square test; Table 3). Age and degree of pain duration were not correlated with post-operative NRS-11 scores (p>0.05, bivariate analysis). No difference in age or duration of pain was detected between groups with long-term success and failure (p>0.05, independent t-test). However, additional resection of the sacrotuberous ligament during piriformis muscle resection was closely related to success (p=0.01, chi-square test). Sciatic nerve decompression was successful in 27 out of 34 patients (79.4%) in the sacroiliac ligament resection group and only 20 out of 47 (42.6%) in the non-resection group. A significant difference was found in the means of the last follow-up NRS-11 scores and percent pain relief among groups undergoing ligament resection and nonresection group (p<0.000, independent t-test; Table 2).
Recurrence and complications following decompression of the sciatic nerve
During the long-term follow-up of 17.5±12.5 months, eight patients (9.9%) underwent reoperation for severe sciatica due to symptom recurrence after initial pain relief. The average time after surgery was 7.25 months (SD, 3.88; range, 4-14) when reoperation was decided. The reoperation rate was in higher in the sacrotuberous ligament non-resection group (17.6%) than in the resection group (4.3%). Repeated sciatic nerve decompression was successful, defined as greater than 50% pain relief, in three of eight patients (37.5%).
No intraoperative nerve damage was found in 100 cases of sciatic nerve decompression including bilateral surgery and reoperation. Intraoperative neurophysiological monitoring revealed no significant alarming events involving the sciatic nerve or its branches. However, peroneal nerve palsy was detected after surgery in one patient (1%) even though no intraoperative nerve loss or intraoperative monitoring event occurred.
DISCUSSION
Sciatic nerve and its variations with piriformis muscle
The sciatic nerve is the largest nerve of the body and carries contributions from L4 to S3. It leaves the pelvis through the greater sciatic foramen inferior to the piriformis muscle, enters and passes through the gluteal region into the posterior compartment of the thigh [34,35]. The sciatic nerve has an intimate relationship with the piriformis muscle along its course from the pelvis to the gluteal region and several structural variations have been defined [3]. Seven anatomical relationships between the sciatic nerve and piriformis muscle were first described by Beaton and Anson [3] in 1937. The conventional and most common relationship, type A, involves an undivided sciatic nerve that courses below the piriformis muscle. The type A sciatic nerve anatomy is prevalent in approximately 80-90% based on a cadaver study [31]. The type B sciatic nerve is the most common variant, with a prevalence of 10-15%, in which one division of the sciatic nerve passes through and the other below the piriformis muscle [21].
The sciatic nerve variation was once thought to be associated with piriformis syndrome [28]. However, it is now considered to be a normal variant of uncertain clinical significance [2]. No difference was found in the prevalence of variant anomaly in the sciatic nerve and piriformis between cadavers and the reported surgical cases series [28]. Piriformis syndrome can affect patients with normal or variant sciatic anatomy and patients with variant anatomy are generally asymptomatic [28]. In line with this, there was no difference in results of decompression between type A and type B variations in the current study.
The piriformis muscle attaches proximally to the lateral border of the sacrum, the anterior aspect of the sacrum (S2-S4 segments), the superior margin of the greater sciatic notch, and the sacrotuberous ligament [28]. It then exits the pelvis in the greater sciatic foramen formed by the ileum and attaches to the superior portion of the greater trochanter. Normally, the lumbosacral plexus is formed on the ventral surface of the piriformis muscle. The four nerves (sciatic, pudendal, posterior femoral cutaneous, and inferior gluteal nerve) exit below the piriformis muscle [28]. Thus, the sciatic nerve and the piriformis muscle transition together from the pelvis to the subgluteal space through the greater sciatic foramen; they are closely related to each other and exhibit various anatomical variations.
Piriformis syndrome and sciatic nerve entrapment at the greater sciatic notch
The term “entrapment neuropathy” refers to isolated peripheral nerve injuries that occur at specific locations where a nerve is mechanically constricted in a fibrous or fibro-osseus tunnel or deformed by a fibrous band [8]. Therefore, entrapment of peripheral nerves occurs only in specific fibro-osseus tunnel in the corresponding nerve pathway. Representative examples are carpal tunnel syndrome, which refers to median nerve entrapment at the wrist, and cubital tunnel syndrome, which refers to median nerve entrapment at medial elbow. Brachial plexus entrapment in the interscalene triangle is interpreted as neurogenic thoracic outlet syndrome. Similarly, piriformis syndrome can be interpreted as sciatic nerve entrapment in the greater sciatic notch.
The term “piriformis syndrome” represents the entrapment neuropathy of the sciatic nerve through and around the piriformis muscle at the greater sciatic notch, and is a non-discogenic cause of sciatica [5,9]. The term “piriformis syndrome” is elusive and confusing [25]. Piriformis syndrome is not a disease of the piriformis muscle itself, but a defect involving the sciatic nerve that is compressed by this structure, resulting in sciatica. In addition, it is known that the tendon of the piriformis muscle, together with the muscle mass, compresses the nerve, rather than the piriformis muscle itself being the main structure that compresses the nerve [9]. Therefore, when decompressing the sciatic nerve, not only the bulk of piriformis muscle that contacts the nerve, but also the tendon of the piriformis muscle should be removed (Fig. 2) [9,30-34].
Sacrotuberous ligament and its role in decompression of sciatic nerve
The tunnel through which the sciatic nerve and piriformis muscle passe from the pelvic cavity into the subgluteal space consists of the sciatic notch of the iliac bone below and the sacrotuberous ligament above. The sacrotuberous ligament, located posterior and inferior in the pelvis, is associated morphologically and functionally with the sacroiliac joint [35]. The sacrotuberous ligament spans across the sacrum and the ischial tuberosity and forms the boundaries of the greater and lesser sciatic notches (together with the sacrospinous ligament). It is closely related to the surrounding muscles including gluteus maximus, piriformis, and the long head of biceps femoris [35]. The posterior surface of sacrotuberous ligament is attached to the lower fibers of gluteus maximus muscle. In addition, similar to gluteus maximus, the upper part of the pelvic surface of the sacrotubeous ligament carries a site for attachment to piriformis [8,35]. The sacrotuberous ligament, fused with the piriformis and gluteus maximus muscles, forms a kind of compartment compressing the sciatic nerve from the back. Therefore, a simple resection of the piriformis muscle around the sciatic nerve may be insufficient to decompress the sciatic nerve within this compartment [34]. Accordingly, the group undergoing partial resection of sacrotuberous ligament fused with the piriformis muscle showed significantly better results than the group without sacrotuberous ligament resection.
In addition, the group without ligament resection showed significantly higher rate of symptom recurrence after decompression (12.8% vs. 5.9%) than the group with ligament resection in my study. In fact, the sacrotuberous ligament was reported to have a very large regenerative potential [11]. In one MRI study of the pelvis performed 3 years after surgical division of the sacrotuberous ligament for pudendal nerve decompression [11], the divided sacrotuberous ligament regenerated and became significantly thicker than in normal controls, suggesting sacrotuberous ligament regeneration via remodeling and regrowth [11]. Since the piriformis muscle together with the sacrotuberous ligament constitutes a compartment that entraps the sciatic nerve, piriformis muscle resection alone might be insufficient for complete decompression of the compartment that entraps the nerve. In addition, the possibility of adhesion and symptom recurrence may be high due to adhesion and fibrosis of surrounding structures in a compartment that is not sufficiently decompressed.
Two cases of perineural scar formation and symptom recurrence after piriformis resection were already reported in 2008 [18]. Symptom recurrence occurred relatively quickly as early as 6 weeks after surgery, resulting in long-term pain relief with reoperation with fibrous scar debridement and insertion of polytetrafluoroethylene pledgets around the sciatic nerve to avoid perineural adhesions during repeated surgery [18]. We confirmed that severe fibrous adhesions and scars occurred on the severed piriform muscle stump based on reoperation findings. These adhesions involved sacrotuberous ligament and eventually formed a lump around the sciatic nerve. Therefore, starting in 2021, I resected the piriformis muscle more proximally, including the lateral margin of the sacrotuberous ligament to which the piriformis muscle was attached, in order to reduce postoperative adhesion significantly. In addition, from 2021, the compartment composed of the sacroiliac ligament and the piriformis muscle was opened. Following external neurolysis of the sciatic nerve, a polytetrafluoroethylene film was inserted around the nerve.
Study limitations
Although I could achieve significant pain reduction in 81 patients with piriformis syndrome with my transgluteal approach, the long-term success rate, defined as 50% improvement in preoperative pain, was 61.7%, which was not very high. In fact, I experienced a significant learning curve while performing sciatic nerve decompression. My results indicated a high success rate of 80% for circumferential dissection of the sciatic nerve via resection of the piriformis muscle compartment containing the sacrotuberous ligament from 2021. My transgluteal approach required a longer incision, approximately 10 cm, than the minimally invasive transgluteal approaches reported previously [9]. The authors performed the surgery via transgluteal approach designed for pudendal nerve decompression [12,26], based on the minimally invasive transgluteal approach described by Filler et al. [9]. Pudendal nerve decompression requires dissection of the sacrotuberous ligament, which forms the Alcock’s canal [12,26]. The sacrotuberous ligament forming Alcock’s canal, the site of entrapment of the pudendal nerve, is located only approximately 3 cm away from the site of attachment of the piriformis muscle. The piriformis muscle is not a separate structure from the overlying sacrotuberous ligament [1,21,28]. The piriformis originates from the ventral surface of the sacrum, but also originates from and fuses with the sacral tuberculous ligament [1,21,28]. The findings of reoperation, in which the resected piriformis muscle and sacrotuberous ligament together formed adhesions and scars, raised the need for awareness of the importance of proximal and circumferential dissection of the sciatic nerve in the greater sciatic notches. Even after further circumferential release of the piriformis compartment, including sacrotuberous ligamentectomy, recurrence was still detected, suggesting that either the sciatic nerve decompression may be technically incomplete, or the diagnosis of piriformis syndrome was incorrect.
Although my results suggest the effectiveness of sciatic nerve decompression based on the concept of compartmental release, it is difficult to generalize them. Since study was performed by a single surgeon in a single institute, it is difficult to directly compare the finding with other studies utilizing various approaches in different institutions.
CONCLUSION
Decompression of the sciatic nerve using transgluteal approach was effective in pain relief for sciatic nerve entrapment at the greater sciatic notch, formerly called piriformis syndrome. During transgluteal sciatic nerve decompression, it is important to decompress the sciatic nerve pathway in the compartment formed with the piriformis muscle and its tendon and the sacrotuberous ligament, rather than simply decompressing the sciatic nerve via resection of the piriform muscle.