INTRODUCTION
The etiology of spinal trauma and the nature of the vertebral column involved varies, with cervical fractures representing approximately one-half of all spine fractures [8]. Fracture of C2 accounts for approximately 17-25% of acute cervical fractures [29,33]. C2 vertebral fractures include odontoid fractures and HangmanŌĆÖs fractures. It can be caused by axial compression, hyperflexion, or hyperextension injury. According to a national registry study between 1997 and 2014, the incidence of C2 fractures increased from 3 to 6 per 100000. 51% of them were men, and the average age was 72 [42]. Surgery was more likely to be performed on patients who were male, younger, and had spinal cord injuries. The treatment plan would involve conservative treatments, such as rigid fixation with a cervical collar or halo vest, or surgical fixation [35]. Surgical fixation techniques for C2 fracture are varied and include C1-2 fusion using C1 screws and C2 translaminar, pars or pedicle screw fixation [9,22,24,26], anterior odontoid screw placement [10,37], and occipital plate techniques, among others. Because of the unique anatomical structure and injury type of the C2 vertebra, it is essential to understand the classification of injury and surgical indications when establishing a treatment strategy. Furthermore, understanding the most recent consensus on C2 vertebral fracture could aid in the proper outcome. The purpose of this study is to gain a better understanding of the current treatment concept of C2 vertebral fracture.
ANATOMY OF C2 VERTEBRA
C2 vertebrae are anatomically different from the C1 and subaxial cervical spine (C3-7). The presence of the dens or odontoid process is the axisŌĆÖs most distinctive anatomic feature. The dens result from the axis fusion with the atlas's vertebral body remnant [3,21]. Its primary role is to smooth the transition across the upper and lower cervical spines, which is made possible by its articulating facets. The superior facets are located anterior and lateral, while the inferior facets are located posterior [46]. A catastrophic outcome from high cervical surgery is possible because of iatrogenic neurovascular injury [23,44,52]. Surgeons must identify the anomaly in the C2 vertebrae and make a plan prior to surgery. The most common anatomical variations are high-riding vertebral arteries and narrow pedicle sizes [25]. Tortuosity of the intra-C2 vertebral artery was more significant in the female sex and it also increased with aging. The different courses of the vertebral artery significantly influenced the pedicle diameter [27].
ODONTOID FRACTURE
Classification
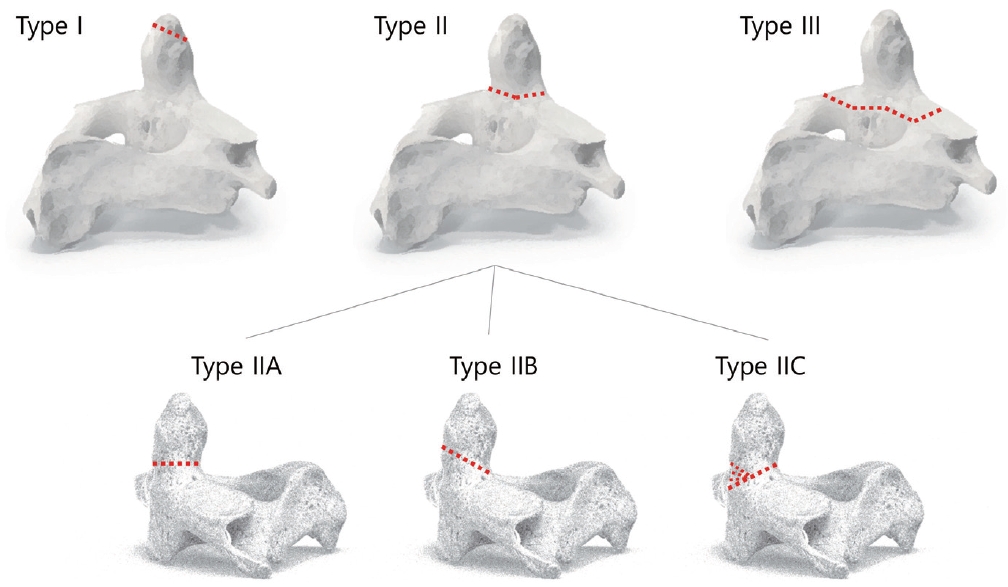
Odontoid fractures account for 9-15% of cervical spine fractures in the adult population, and their incidence increases with the aging population [16,50]. These fractures can occur in young patients in cases of high-kinetic traumatism but often affect the aging population, after minor trauma [40]. The Anderson and DŌĆÖAlonzo classification [4], which identifies the level of the fracture line, is the most widely used classification method. Based on the anatomic location on plain radiographs, they divided these fractures into three categories. Avulsion fractures of the apical ligament are type I fractures that affect the apex of the odontoid. They are uncommon and, unless they are linked to occipital-cervical dislocation, are regarded as safe injuries. Type II fractures, which occur at the intersection of the odontoid and the body of C2, have the highest chance of nonunion because of the weaknesses of the blood supply and bone density associated with the high amount of biomechanical constraints in the dens [19,43]. Type III fractures involve the body of C2, not the odontoid bone, and are not genuine odontoid fractures. Unless they are substantially displaced, these fractures are typically stable.
However, there are still a variety of fracture patterns, particularly in type II fractures, that can lead to unusual treatment situations. In order to address this point, Grauer et al. [17] proposed expanding type II to include subtypes. Minimally shifted or nondisplaced is the definition of type IIA. A fracture of type IIB is one that extends from the anterior-superior to the posterior-inferior or has displaced transverse fractures. An anterior odontoid screw could be used to repair this fracture pattern. A displaced fracture classified as type IIC must either have significant comminution or extend from the anterior-inferior to the posterior-superior (Fig. 1).
Treatment strategy
Treatment options for odontoid fractures are either conservative or surgical. Surgical options include mainly anterior odontoid screw fixation and posterior atlantoaxial arthrodesis. According to the recommendations of a recent international neurosurgical committee survey, general recommendations for odontoid fracture type IIB was suggested anterior screw fixation, and type IIC demands posterior C1-2 fusion [2].
In a systematic review for the efficacy of conservative treatment with halo vest, the effect of conservative treatment on types I and III was quite reliable. Among 660 odontoid fractures, of which 511 were type II, 147 type III, and two type I fractures. Healing was observed in all type I fractures (100% rate of healing). In type II fracture, healing occurred in 71% of patients. In type III fracture, healing occurred in 94% of patients [33].
Type II fractures are clinically challenging as nonunion rates following conservative management range from 24% and 88% [5,18]. The most frequent cervical spine fractures in people aged 70 years or later are type II fractures [38]. The prevalence of these fractures will keep growing because the population is aging [7]. Due to the low probability of successful fusion without stabilization, particularly in elderly patients and cases with significant bony displacement, surgical stabilization at C2 is most usually performed for type II fractures. Anterior odontoid screw fixation is an ideal surgical option to stabilize type II fractures, because it provides a high union rate without limiting neck motion [48]. In a retrospective study including 41 patients with a type II and shallow rostral type III odontoid fracture, anterior odontoid screw fixation resulted in a solid bony union in 33 patients (80.5%), fibrous union in three (7.3%), and nonunion in five (12.2%). The incidence of fusion failure significantly increased when surgery was delayed for more than 1 week and a fracture ŌĆ£gapŌĆØ of 2 mm or more [11].
For anterior odontoid screw fixation, the interval from injury to operation and fracture ŌĆ£gapŌĆØ are significantly associated with fusion failure [2]. Besides this, several recognized anatomical contraindications exist for anterior odontoid screw fixation, including a comminuted fracture at the base of the dens and a disrupted transverse ligament [1,15,28,39]. According to a study by Subach et al. [47], sagittally oblique fractures should be considered a contraindication for this type of fixation. However, contrary to this finding, Cho and Sung [10] concluded that even in cases where the fracture lines of type II and rostral shallow type III fractures are oriented in an anterior oblique direction, anterior odontoid screw fixation may still be a feasible option.
Treatment options are debatable when a type II odontoid fracture coexists with a C1 fracture. Rigid immobilization has an 83% success rate in managing fractures with atlanto-dental interval (ADI) less than 5 mm [34]. In the case of more than 5 mm ADI, early surgical stabilization and fusion (C1-2 fusion) have proved effective in treating fractures [34]. ADI >5 mm indicates the presence of instability in this subtype of fractures, and a high failure probability with external immobilization alone should be considered [2].
HANGMAN'S FRACTURE
Classification
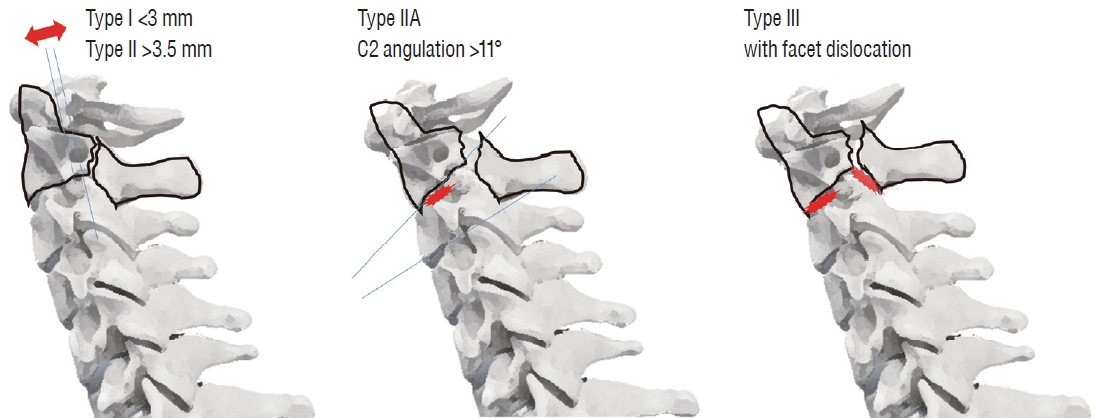
The definition of HangmanŌĆÖs fracture is traumatic spondylolisthesis of the axis due to a bilateral fracture of the C2 pars interarticularis. This fracture type was initially identified in people who were sentenced to death by hanging, but it is now more frequently caused by seatbelt loading in car accidents [51]. Around 15% to 20% of cervical spine injuries are HangmanŌĆÖs fractures. The reported incidence of the neurological deficit caused by HangmanŌĆÖs fractures has varied and ranged from 6.5% to 25% [30]. The classification system for HangmanŌĆÖs Fracture was first described by Effendi et al. [13] and later modified by Levine and Edwards [29]. The classification is based on translation and angulation between C2 and C3 (Fig. 2).
Type I is the most common, and bilateral pars fractures with translation less than 3 mm and without angulation. The discs and ligaments are intact in this type of fracture. Type I fractures are the result of a hyperextension-axial loading force.
Damage to the C2-C3 disc and the posterior longitudinal ligament, as well as anterior C2 displacement on C3 of at least 3.5 mm and angulation with respect to the neural arch, are characteristics of type II HangmanŌĆÖs fractures. In this type, the capsules of the C2-C3 joint are intact. An extension and axial loading followed by a flexion and compression load are assumed to be the combined mechanism resulting in type II fractures. It may lead to neurological deterioration and vertebral artery injury.
Especially in type IIA, the C2 body is more than 11 degrees out of alignment with the C2 neural arch and the C2 is anteriorly displaced on the C3. In contrast to the conventional type II, the fracture line tends to be more horizontally oriented or in the axial plane, and the disc space behaves with angular deformity and lacks translation. This specific type of fracture, which generally occurs by a flexion force applied to the C2 vertebrae, results in a more unstable injury pattern.
Severe neurological damage is frequently related to type III. Type III fractures result in a fracture of the neural arch in addition to the dislocation of the bilateral facets and an unstable injury pattern. Destruction of the C2-C3 disc causes the complete dislocation of C2 on C3. Due to injury to the posterior capsule, the neural arch is totally unrestrained. A primary flexion force causes type IIA and type III fractures. Especially, it was suggested that type III injuries are caused by flexion compression.
Concomitant lesions may be seen on the computed tomography (CT) scan, particularly at the C1 and C1-C2 junctions. In order to correctly diagnose injury to all tissues, including the ligaments and discs, the current suggestion is to conduct a magnetic resonance imaging scan additionally [51]. In addition, a CT-angiography is advised to check for concurrent damage to the vertebral arteries if the fracture line passes through the transverse foramen or if the anterior displacement of C2 reaches 3.5 mm [14,20,45].
Treatment strategy
It is still debatable what the best treatment option is for a HangmanŌĆÖs fracture. According to EffendiŌĆÖs and Levine and EdwardsŌĆÖ modified classification of fractures, treatment decisions are based in part on the type of fracture. Conservative treatment should be reserved for stable type I fractures in patients with no neurological deficit. Conservative treatment has resulted in favorable outcomes with high bone healing rates in this indication. The plenty of blood supply and predominantly cancellous nature of C2 lateral mass may explain the success of non-operative treatment [41,51].
According to a systematic review by Li et al. [31], the healing rate of type I fractures was reported to be 100% without surgical intervention. The authors concluded that most hangmanŌĆÖs fractures could be effectively managed through the application of traction and external immobilization, particularly in cases classified as type I. Furthermore, for specific stable type I and type II fractures, non-rigid external fixation was considered adequate as a standalone treatment option [31].
There are numerous methods for external immobilizing these fractures, including the hard collar, Minerva jacket, sternal occipital mandibular immobilizer brace, and halo vest. No studies have discovered any differences between using a rigid collar and the halo vest to immobilize these fractures [36,49]. According to a recent international neurosurgical committee survey, halo vest should not be used as a conservative therapy for HangmanŌĆÖs fracture due to its possible complications. Instead, use a rigid collar. All of them agreed on this point completely [2].
Unstable type II HangmanŌĆÖs fractures (type IIA) and type III patterns are indications for surgery, and both anterior and posterior approaches have been used. The advantage of the anterior approach (C2-C3 discectomy, interbody fusion, and plate fixation) is technically simple and a relatively short fusion construct. However, the anterior approach does not treat the disconnected posterior arch of C2, and instability persists during flexion and extension. For this reason, it is considered that C2-3 posterior screw fixation and fusion are more biomechanically robust than the anterior approach [6,12]. A cadaveric study reported that the biomechanical comparison of stabilization techniques on HangmanŌĆÖs fracture and posterior C2-C3 screw and rod construction was found to be more effective in stabilizing HangmanŌĆÖs fracture than anterior cervical plating and C2 pars screwing [12].
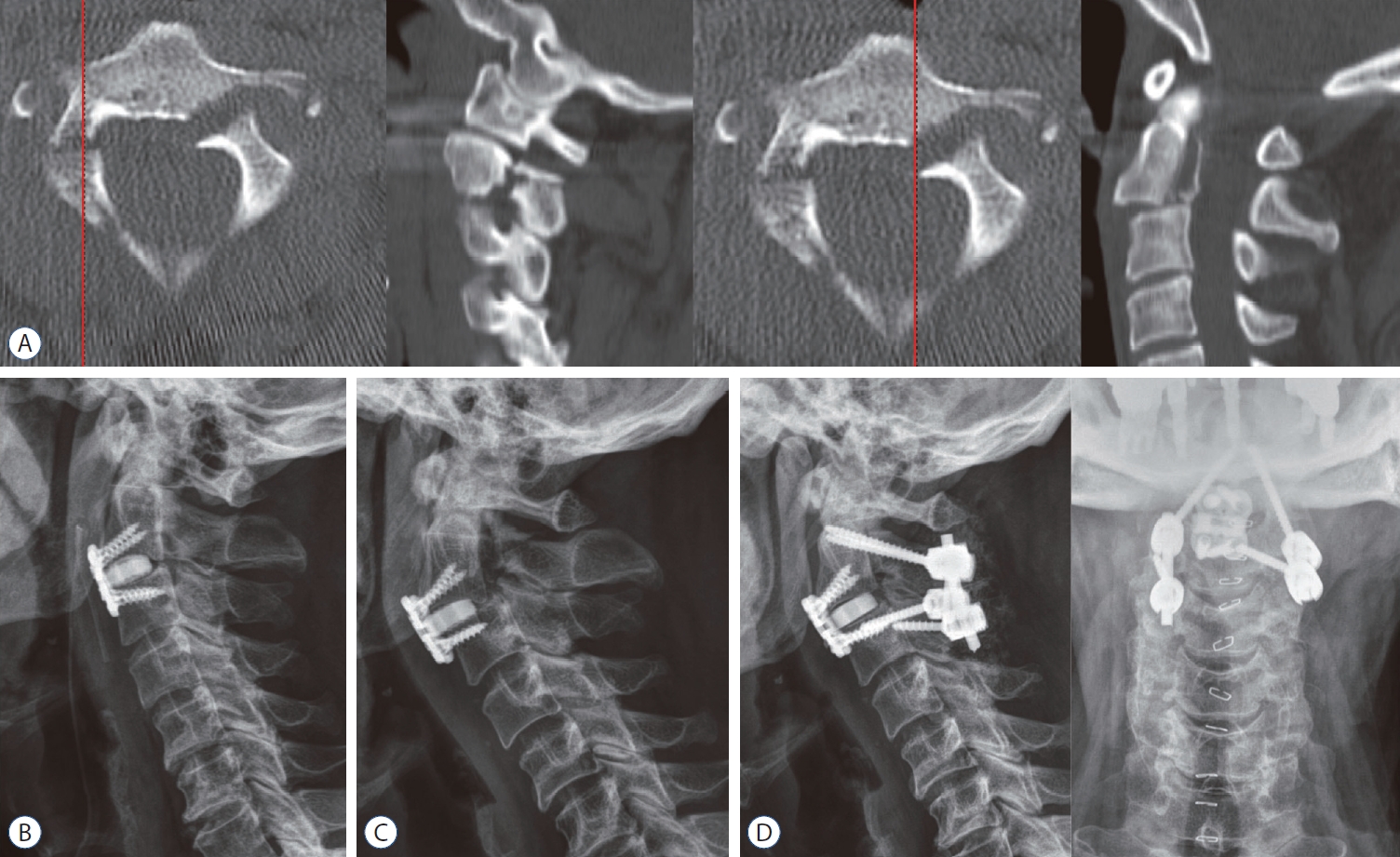
In a systemic review of 417 patients who underwent surgery for a HangmanŌĆÖs fracture, 200 had an anterior approach, 193 had a posterior approach, and 24 had a combination of both approaches. They reported no significant differences in mortality, complications, treatment failure, or fusion rates between surgical approaches [36]. In the literature, authors advocate for an isolated C2 pedicle construct or a posterior C2-C3 fusion if the fracture can be lagged together. If a transpedicular lag screw is not possible, they then advocate for an ACDF in a young patient and a C1-C3 posterior fusion in an elderly patient [36,49]. The literature has also described the use of an anterior-posterior combination technique for C2-C3 fusion. Although type II, IIA, and type III fractures could be treated with this method, it is typically only used for fractures with considerable displacement and a dislocated C2 vertebral body anterior to the C3 vertebra (Fig. 3) [32]. In a recent international neurosurgical committee survey, anterior-posterior combination surgery may be necessary for type III fracture (89% agreed) [2]. Meanwhile, in some cases of C2-3 disc was intact, direct repair of the pars fracture with only C2 screw across the fracture line has the advantage of preserving the motion of the axis. Naturally, instability at the C2-C3 level is not addressed successfully.
CONCLUSIONS
Despite widespread interest among spinal neurosurgeons in treatments for C2 fracture, optimal treatment remains a point of argument. Particularly in the delicate surgical decision of complex high cervical injuries that are sometimes encountered, and older patients with comorbidities and low bone quality. However, there was broad agreement that surgical stabilization and fusion should be considered in cases of type 2 odontoid fractures involving C1-2 segment injury with an ADI of more than 5 mm, HangmanŌĆÖs fracture with a C2-3 angulation of more than 11┬░, or failure of external immobilization. Recognition and proper management of cervical fractures are necessary, given the high rate of morbidity in this critical segment. Randomized controlled trial trials are also required to address the controversial management of fractures.