INTRODUCTION
Radiotherapy (RT) for cancer treatment is well known to elicit an antitumor response by inducing the production of some cytokines [5,12,13]. Radiation can activate an interconnected network of several cytokines, which generates proinflammatory signaling [26]. This radiation-induced immune response is also suggested to occur as a result of high-dose irradiation of tumors. Preclinical studies have shown that high-dose irradiation can stimulate antitumor T cell immunity by promoting cross-priming by antigen-specific dendritic cells to increase the number of activated CD8+ T cells [9,11,16].
Of note, Gamma Knife Radiosurgery (GKS) for brain metastases have recently known to enhance the immune response against the tumor, even though brain as “immuneprivilege” [12]. Particularly, natural killer (NK) cells are known to play an important role in antitumor immunity, stimulated by radiation [6]. Activation of NK cells induce target cell apoptosis though cytotoxicity by perforin and granzyme B [7,24] and secretion of proinflammatory cytokines such as tumor necrosis factor-alpha and interferon-gamma (IFNγ) [4,37].
Recently, we measured the activity of NK cells by monitoring the level of IFNγ in serum using the NK Vue kit (NK MAX, Sungnam, Korea). This kit is an in vitro diagnostic test system that can measure NK cell activity (NKA)-IFNγ levels using enzymatic immunoassays. Previous studies have reported that compared to healthy subjects, patients with malignancy have significantly decreased levels of NKA-IFNγ [19,21]. Based on these findings, we investigated the activity of NK cells before and after GKS by evaluating the levels of IFNγ via the NK Vue kit. For evaluating the immunologic changes after GKS, we conducted prospectively preliminary research including brain metastatic patients as well as benign brain tumor patients, such as meningioma and schwannoma.
MATERIALS AND METHODS
An independent Institutional Review Board of Seoul National University Hospital approved (H-1701-075-824).
Study design
This study was an open-label, prospective, cross-sectional clinical performance study for the measurement of NKA in whole blood (NK Vue; NK MAX) from subjects with a brain tumor. Subjects were enrolled between February and August 2018.
Enrollment of patients
Patients were eligible for enrollment if they were male and older than 20 years old. Other eligibility criteria included providing informed consent for participation. Subjects could not participate if they could not understand the consent form or were unable to read it or if they had conditions shown to impact the activity of NK cells. The inclusion criteria were newly diagnosed brain tumor and no prior RT/radiosurgery within a minimum of the preceding three months. The exclusion criteria were high-grade glioma and a Karnofsky performance status lower than 70. The study also excluded patients who were receiving chemotherapy for a condition that could affect NK cell activity. Therefore, only patients who were not exposed to chemotherapy for at least one month were selected.
Blood sampling and NKA-IFNγ assay
All patients received a steroid injection (2 mg dexamethasone intravenously) to reduce peritumoral edema after GKS according to the protocol of the Gamma Knife Center. However, the steroid was only used just before and after GKS and was not used thereafter. Of the included patients, 10 patients had blood sampling performed before steroid injection and were used as a control group, and the remaining patients had sampling performed after a steroid injection and immediately before GKS. All patients completed follow-up magnetic resonance imaging of the brain between 1 and 3 months after GKS, and blood sampling was conducted simultaneously. Therefore, the patients had two blood samples drawn, one before and one after GKS, to measure the level of NKA-IFNγ. Of note, the steroid was not used at the time of the blood sampling conducted after GKS, and there were no effects of NKAIFNγ levels by pre-GKS steroid injection.
NKA-IFNγ levels were determined by enzymatic immunoassay using the NK Vue kit (NK MAX), as described previously [21]. This method stimulates whole blood (1 mL) with Promoca, and engineered recombinant cytokines that activate NK cells explicitly, and then measures IFNγ levels released from activated NK cells. After incubation for 20-24 hours at 37°C, the levels of IFNγ were measured with an ELISA. The detectable range was 0.1-4000 pg/mL, and the total imprecision of two levels of controls was less than 15% coefficients of variation. Unlike traditional methods for measuring of NK cell activity, this assay is simple and standardized. As it analyzes the distribution of lymphocytes in the IFNγ expressing subset, this assay has become applicable in the clinical setting as an estimate of NK cell activity. Therefore, it has been demonstrated in several papers that the activity of NK cells measured in this particular way is reliable [27,28].
Statistical analysis
Statistical analyses were performed using IBM SPSS version 23 (IBM SPSS, Armonk, NY, USA) and GraphPad Prism 5 (GraphPad Inc., La Jolla, CA, USA) was used to create figures. Categorical data were compared with the chi-square test or Fisher’s exact test, as appropriate. Cox regression analysis was performed to evaluate the hazard ratio and corresponding 95% confidence interval (CI). The correlation between the level of NKA-IFNγ and the reduction in tumor volume rate was evaluated by the Pearson correlation coefficient. All p-values were two-tailed. Statistical significance was considered at p<0.05.
RESULTS
This study included 28 patients with metastatic brain tumors and 10 patients with benign brain tumors, such as schwannomas and meningiomas. Patient characteristics are shown in Table 1. Of the 28 patients with brain metastasis, the most common primary tumor site was the lungs (67.9%). The mean target volume was 7.20 cm3 (range, 0.03-27.46), and the mean GKS dose was 22.94 Gy (range, 15-30). Eight patients underwent fractionated GKS, and 13 patients were previously irradiated via GKS. One patient underwent whole-brain RT before GKS, and two patients underwent craniotomy. Primary tumor control was observed in 20 patients, and systemic tumor control was found in 18 patients at the time of the study. This means that the disease burden of the primary tumor or systemic metastases does not progress.
Clinically, the tumor volume after GKS decreased significantly, and the levels of NKA-IFNγ increased (Table 2). However, no correlation between the two parameters was observed (Pearson sample correlation coefficient, 0.021; p=0.92). Changes from the initial tumor volume and levels of NKA-IFNγ also had no statistically significant correlations (p=0.41).
There were no significant differences in the changes in the levels of NKA-IFNγ up to 3 months after GKS (Table 3). Factors affecting the levels of NKA-IFNγ, the use of chemotherapy pre-GKS or post-GKS, and the presence of primary tumor control, systemic control, or several brain metastases were compared, but no statistically significant factors were identified.
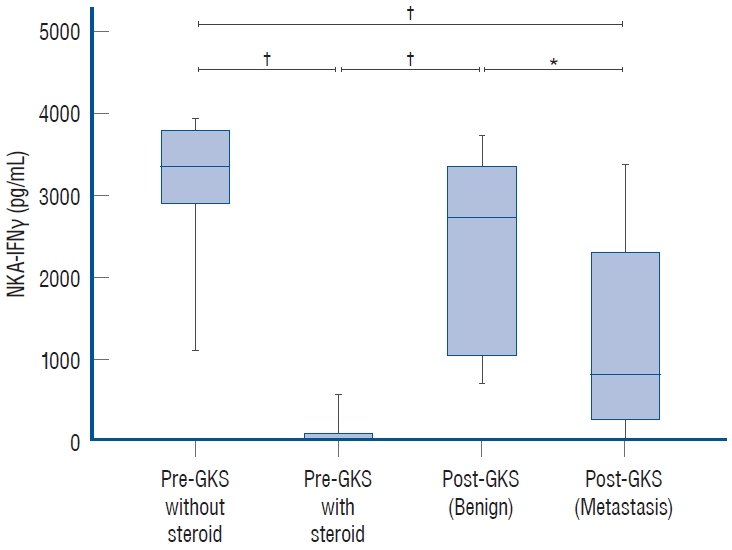
The levels of NKA-IFNγ pre-GKS, post-GKS in brain metastasis patients, and post-GKS in benign brain tumor patients are shown in Fig. 1. The levels of NKA-IFNγ in the patients who were injected with steroids before GKS were zero in all except one patient. Interestingly, the IFNγ levels of the patients with malignant tumors, such as brain metastases, were significantly lower than those of the patients with benign brain tumors.
DISCUSSION
In the present study, we observed changes in serum IFNγ levels in brain tumor patients after GKS. Additionally, it was found that the IFNγ levels of the patients with malignant brain tumors represented as metastatic tumors were lower than those of the patients with benign brain tumors. The results showed that the NKA-IFNγ of patients with malignant brain tumors was more suppressed than that of benign tumor patients. These findings might imply that increasing the activity of NK cells may potentiate immunotherapy for malignant brain tumors.
Several studies have investigated the immune system in brain tumor patients, mainly in the context of malignant glioma. These studies suggested that brain tumor patients suffer from broad immunosuppression due to lymphopenia, decreased lymphocyte proliferation, increased cytotoxic deficiencies, reduced Major Histocompatibility Complex (MHC) class I expression on monocytes, and predominant anti-inflammatory T-helper 2-type cytokine production [10,30,33]. To overcome extensive immunosuppression, NK cells were studied as an immunotherapeutic target because of the direct cellkilling effect mediated by the innate immune response. NK cells possess the innate ability to detect transformed cells and are thus crucial to cancer immunosurveillance and antitumor immunity without the requirement of prior antigen exposure [8]. They perform cytotoxic activities through granzymeand perforin-mediated apoptosis or expression of death receptor ligands such as FasL and tumor necrosis factor (TNF)- related apoptosis-inducing ligand [38]. However, many tumors evade surveillance by NK cells, resulting in a skewed phenotype and impaired functionality during cancer progression. Therefore, increasing the activation of NK cells has become one of the strategies for brain tumors. Since Stevens et al. [35] showed that NK cells infiltrate the tumor site in gliomas, carcinoma metastases, and meningiomas, functional studies of the antitumor response mediated by NK cells have been attempted. Poli et al. [31] demonstrated that NK cells diminish tumor growth by recruiting macrophages and inducing the overexpression of MHC class II on microglia as well as the elevation of IFNγ and TNF-α levels in the cerebrospinal fluid. Lee et al. [22] also showed that NK cell-mediated immunity is responsible for the suppression of systemic glioblastoma metastasis in mice. However, despite this evidence, the complex nature of the immune system makes NK cell-based therapies far from clinically successful strategies for brain tumor treatment.
Recently, there has been increasing evidence that localized irradiation of a tumor may also modify the tumor microenvironment and generate proinflammatory cytokines [25,26,32,40], which can increase the robustness of the immune response. The effect of radiation is known to be dependent on T cells, and their ability to recognize tumor antigens, primarily via RT-mediated T cell priming, contributes to the activation of host immunity. Even if high-dose irradiation, such as that applied with GKS, is considered and the RT differs in radiobiological aspects, there is ample evidence that radiosurgery also triggers an immune response against tumors [34,39]. Not only is GKS effective with programmed cell death 1 receptor antagonists for brain metastasis [1,29], but more recent evidence has shown that GKS regulates the immune response [12]. This report suggested that GKS for metastatic brain tumor patients are regulated cytokines such as IFNγ and interleukin-2 [12]. The results showed that the level of IFNγ at 1 hour post-GKS in metastatic brain tumor patients increased and that after 1 week was lower than that at 1 hour, but still increased before GKS. However, our results were discrepant, as IFNγ levels declined after GKS. In aprevious study, IFNγ levels decreased over time [12], and our findings were measured at least 1 month after GKS. These discrepancies are considered to need to be investigated later with more subjects and immune profiles. Overall, the IFNγ level after GKS is increased for at least 1 week, but it could be decreased when 1 month has passed. Interestingly, the IFNγ level after GKS for benign tumor patients was higher than that for metastatic brain tumor patients, representing the immunosuppressive status of metastatic brain tumor patients. Therefore, it is likely that improving the immunosuppressive status of metastatic brain tumor patients can be a basis for treatment.
Moreover, no correlations between the interval after GKS or the rate of reduction in tumor volume and changes in serum IFNγ levels were found. This means that the more IFNγ levels was measured, the less the size of tumor volume was reduced. This lack of correlation was probably because this study is based on prospective clinical data with a relatively small number of patients. Although our results did not show that GKS stimulates the immune response, it has been demonstrated in the literature that GKS stimulates a cellular immune response involving NK cells against brain metastases [36]. A previous study performed histopathological and immunohistochemical evaluations of 11 tumor tissue samples obtained by craniotomy from patients who received GKS. However, this study only produced cytological observations, demonstrating GKSreactive cells but not showing changes in the immune response. On the other hand, our results provided evidence that it could cause changes in the immune system after GKS. These findings have consistency with another previously mentioned study [12].
In this study, we measured IFNγ released from stimulated NK cells in 1 mL of fresh whole blood. This modern method of measuring NK cell activity is standardized and straightforward compared to flow cytometric assays [27]. This test has already been verified, and it has been used to investigate possible prognostic markers [2,14,15,20]. However, no studies have been performed to determine the activity of NK cells after GKS in brain tumor patients. Interestingly, the levels of NKA-IFNγ in patients treated with steroids were low. Considering that steroids inhibit NK cell activity, this test might be reliable.
Recent studies have shown that the systemic immune status does not differ from the brain’s immune status. The traditional concept that the blood-brain barrier makes the brain immune system different from the systemic immune system has been completely changed due to the discovery of brain lymphatic vessels by Kipnis and colleagues [18,23]. In parallel with these discoveries, recent studies have demonstrated the presence of microglia and other immune cells within the brain that have been shown to respond to systemic cytokines [3,17,18]. These findings provide supporting evidence that the brain is not as ‘immunoprivileged’ as previously accepted. These findings imply that the systemic immune status reflects the brain’s immune response. In other words, serum levels of NKA-IFNγ could indicate the brain’s immune status. Serum levels of NKA-IFNγ could also be used as a therapeutic or diagnostic marker as they are significantly decreased in malignant brain tumors relative to benign brain tumors. Additionally, we expect that it will serve as a basis for use as a predictive marker in reducing the clinical confusion that occurs after GKS, such as radiation-necrosis, pseudo-progression, and recurrence.
This study has several limitations because of its relatively small sample size and lack of evaluation of other immunological factors, such as interleukins, chemokines, and tumor necrosis factor. The heterogeneity of the small sample size was the reason why the unclear results become. The most significant limitation is that there are no additional cytokine data to comprehensively evaluate the post-GKS immune system for brain tumors. Moreover, our study has a crucial limitation as no consecutive data. Because only the pre- and pos-GKS NKA-IFNγ were measured without baseline NKA-IFNγ, there is a potent confusion about the immune effects of GKS. Additionally, even if IFNγ is a potent immunomodulator and reflects the activity of NK cells, questions remain as to whether the levels of NKA-IFNγ can represent the immune status of brain tumor patients. Finally, our results did not provide the level of NKA-IFNγ in healthy people. Although previous studies have identified the values of the normal range [2,14,15,20], the incomplete results make relative comparisons difficult and potentially confusing.
CONCLUSION
Despite these limitations, our study has the novelty of being a valuable investigation to evaluate the immune response in brain tumor patients after GKS. Because the levels of NKAIFNγ after GKS were significantly lower in malignant tumors than in benign tumors, NKA-IFNγ might have diagnostic value as a prognostic marker. Additionally, these results indicate that evaluating the activation of NK cells is a promising strategy for estimating the immune status of patients with brain tumors as well as their immune conditions before and after brain tumor treatment. Although further clinical studies with larger populations are required to confirm the immunological changes after GKS in patients with brain tumors, our results suggest that GKS might modulate the immune response in patients with brain tumors.