INTRODUCTION
The recent introduction of stents has led to the increased use of stent-assisted coil embolization (SAC) for various types of intracranial aneurysms. Deploying the stent across the aneurysmal neck creates a mechanical barrier to prevent coil protrusion into the parent artery and helps to achieve compact coil packing. In addition, stent placement can reduce the recanalization rates by inducing stable thrombosis within the aneurysmal sac, modulating hemodynamic factors and improving neo-endothelialization [1,17]. However, because of the thrombogenicity of stents, thromboembolic complications are major concerns for patients undergoing this procedure, so periprocedural dual antiplatelet therapy with aspirin and clopidogrel is necessary to eradicate these concerns. Gradually, over time, thrombogenicity decreases because of intrinsic fibrinolytic activity of the endothelium and neo-endothelium covering the stent surface [8]. Accordingly, most clinicians perform dual antiplatelet therapy within 6 months after SAC and switch to mono antiplatelet therapy (daily aspirin) to avoid the risks associated with dual antiplatelet therapy [5,14].
Although Matsumoto et al. [9] reported that thromboembolic events after the procedure are most likely to occur within 40 days after SAC even if patients receive dual antiplatelet therapy, previous studies reported that delayed thromboembolic complications can occur after 40 days [3,11,12,15]. These studies commonly found that an insufficient duration of dual antiplatelet therapy was associated with delayed thromboembolic events, which indicates the need for an extended duration of dual antiplatelet therapy. On the other hand, another study showed that long-term use of dual antiplatelet therapy after SAC increased the frequency of delayed hemorrhagic events [14]. Clinicians varied the duration of dual antiplatelet therapy after SAC, which was consistent with similar studies. The currently used antiplatelet therapy protocol for SAC is based on the guidelines for coronary intervention. However, since cerebral aneurysm is anatomically and pathologically different from cardiovascular diseases, it is unclear whether the antiplatelet therapy protocol used for coronary intervention is safe or effective in patients undergoing SAC for unruptured intracranial aneurysms (UIAs). In addition, no randomized study regarding neuroendovascular treatment has been performed to address this issue.
Therefore, the aim of this study is to assess the effect and safety of long-term (12 months) dual antiplatelet therapy in patients with UIAs after undergoing SAC by evaluating the occurrence of delayed thromboembolic and hemorrhagic events compared with the short-term (6 months) dual antiplatelet therapy.
MATERIALS AND METHODS
Design
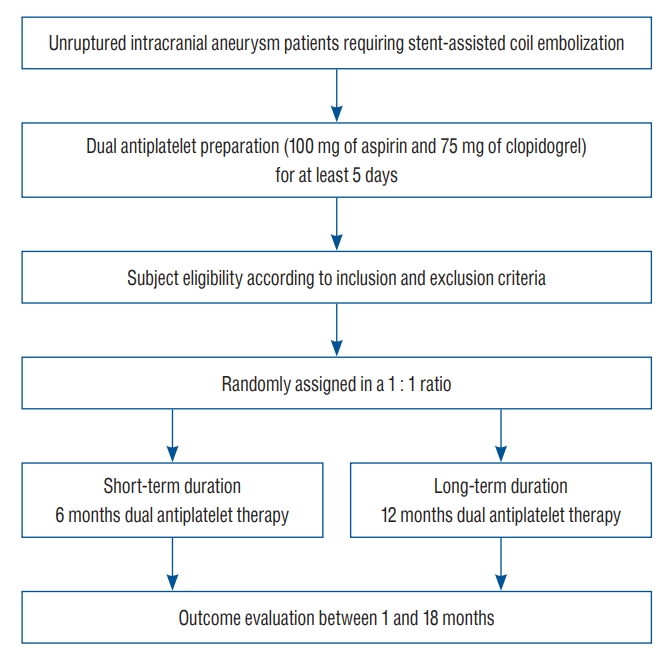
This is a prospective, multicenter (14 institutions), randomized, controlled trial designed that aims to compare the effect and safety of long-term (12 months) dual antiplatelet therapy with short-term (6 months) dual antiplatelet therapy in patients with UIAs after undergoing SAC. Participants will be randomly assigned, 1 : 1, to a short-term duration group or a long-term duration group. The study flowchart is shown in Fig. 1.
Study population
The study population will enroll 528 subjects with UIAs, who are age ≥19 years and eligible for SAC (as confirmed by digital subtraction angiography [DSA]). All enrolled subjects will receive 100 mg of aspirin plus 75 mg of clopidogrel for at least 5 days before SAC. One day prior to SAC, the aspirin reaction unit (ARU) and P2Y12 reaction unit (PRU) will be measured using VerifyNow (Accumetrics, San Diego, CA, USA). Previous studies found that thromboembolic events during the periprocedural and follow-up periods were more likely to occur in patients with low responsiveness to antiplatelet therapy, so this study will include only patients with an adequate response to antiplatelet agents [2,6,18]. In this study, in reference to several studies, the appropriate range of response to antiplatelet agents will be determined as ARU <550 and PRU 85-219, considering the hemorrhagic and thromboembolic risks [4,16]. Detailed inclusion and exclusion criteria of this study are described in Table 1. This study will be performed after approval from the institutional review board at each participating institution. Each subject will be asked to provide written informed consent prior to undergoing SAC for UIAs.
Randomization
After confirming that the subject meets all study eligibility criteria and signing the informed consent, each subject will be randomized in a 1 : 1 fashion to a short-term or long-term dual antiplatelet therapy group using a computer-generated randomized sequence. Central randomization will be performed, and a random number will be given by trial online process registration. Allocation will be known to all involved in this study.
Treatment
The SAC procedures will be performed under general or local anesthesia according to the protocol of each institution. Systemic heparinization will be performed after the femoral introducer sheath is placed, and heparin will be later infused at an hourly booster dose of 1000 IU with monitoring of the activated clotting time. Rotational angiography for three-dimensional (3D) image reconstruction will be performed before SAC. Based on the 3D images, at least two working projections that provide the best image of the aneurysmal neck will be determined.
After placing a microcatheter into the aneurysmal sac for coil delivery, the stent will be deployed using another microcatheter to sufficiently cover the aneurysmal neck. Like this, the jailing technique will be given priority for SAC, but a trans-stenting technique will also be allowed depending on the situation. Selection of detachable bare platinum coils, type of stents, length of stents and diameter of stents will be determined by the endovascular neurosurgeons at each participating institution. The aneurysm will be packed using bare metal coils until proper occlusion will be achieved or further coiling will be deemed dangerous. Finally, the procedure will be terminated after confirming the aneurysmal occlusion grade in DSA and detecting any procedural complications.
For subjects assigned to the short-term dual antiplatelet group, aspirin at a dose of 100 mg once daily plus clopidogrel at a dose of 75 mg once daily will be prescribed for 6 months after the procedure; after 6 months, this therapy will be exchanged for daily oral treatment with 100 mg of aspirin. For subjects assigned to the long-term dual antiplatelet group, aspirin at a dose of 100 mg once daily plus clopidogrel at a dose of 75 mg once daily will be prescribed for 12 months after the procedure; after 12 months, this therapy will be exchanged for aspirin at a dose of 100 mg once daily.
Primary and secondary endpoints
The primary endpoint will be delayed thromboembolic events, which are defined as a transient ischemic attack or ischemic stroke with evidence of infarction on diffusion weighted imaging, which occur in a vascular territory consistent with the stented vessel location between 1 and 18 months after SAC. The secondary endpoint of the study will include the following : 1) bleeding events according to current updated thrombolysis in myocardial infarction bleeding criteria between 1 and 18 months after SAC [10]; 2) periprocedural complications including thromboembolic and hemorrhagic events within 1 month after SAC; 3) neurological outcomes as measured by the modified Rankin Scale scores at inclusion in the study and at 1, 6, 12, and 18 months after SAC; 4) ARU and PRU at 6 months after SAC; 5) aneurysm obliteration grades as described by the Roy-Raymond occlusion classification at immediate procedure and at 18 months after SAC [13]; and 6) morbidity and mortality between the 1- and 18-month follow-up after SAC. Table 2 shows the schedule of study visits.
Data safety monitoring board (DSMB)
The DSMB will be composed of three research-related neurosurgeons including the principal investigator, one contract research organization staff member, and three non-research-related neurosurgeons. The DSMB will review the data and monitor the safety while maintaining the scientific integrity of the trial. Based on the safety data, the DSMB will determine the reporting practice and recommend modifications to the protocol, suspension or termination of the trial.
Sample size
Recent studies showed that delayed thromboembolic complication rates ranged from 3.5% to 7.9% [3,7,15]. Based on the results of these studies, the rate of delayed thromboembolic complications was estimated to be 5.4% in the short-term dual antiplatelet therapy group within 18 months after SAC. Assuming that a delayed thromboembolic complication rate would be reduced to 1% in the long-term dual antiplatelet therapy group after SAC (rate difference, 4.4%), taking into account a two-sided significance level of 0.05 with 80% power, the calculated sample size would be 250 subjects per group. Considering a 5% loss to follow-up, this study will require 528 subjects (264 subjects in each group).
Statistical analyses
An intention-to-treat analysis will be used in all analyses. Categorical data will be presented with numbers, including percentages, and continuous data will be presented with means, including standard deviations. The Wilcoxon rank sum test will be used for continuous variables, and chi-square or Fisher’s exact tests will be used for nominal factors in comparisons of baseline characteristics. The percentage of subjects with delayed thromboembolic events between 1 and 18 months after SAC will be calculated in each of the two groups. The cumulative rate of the primary endpoint in each of the two groups will be analyzed by using Kaplan-Meier estimates. Cox proportional hazard analysis will be used to analyze the primary outcome, adjusted for covariables with 95% confidence intervals (CIs). For the secondary endpoint of binary data and, as measured at a single endpoint, Cox proportional hazard analysis will be used, adjusted covariables with 95% CIs. Subgroup analysis will be performed to evaluate treatment effect modification. The primary outcome will be compared in the predefined subgroups, predefined by aneurysm size (≤10 mm or >10 mm), aneurysm neck size (≤4 mm or >4 mm), stent type (laser-cut versus braided), stent length (≤20 mm or >20 mm), and aneurysm obliteration grade at 18 months (Roy-Raymond occlusion classification of 1 or ≥2). The significance of possible differences between subgroups in treatment effectiveness will be evaluated with the interaction terms.
RESULTS
The trial will begin enrollment in 2022, and clinical data will be available after enrollment and follow-up.
DISCUSSION
The aim of this study is to provide definitive information on the effect and safety of long-term dual antiplatelet therapy in comparison to short-term dual antiplatelet therapy in patients with UIAs after undergoing SAC.
Previously, several studies have published delayed thromboembolic complications according to the duration of dual antiplatelet therapy [3,7,15]. In particular, Hwang et al. [3] analyzed 403 aneurysms in 395 patients treated with SAC and reported that long-term use of dual antiplatelet therapy reduced the delayed thromboembolic event rate without increasing bleeding risk. However, these studies were retrospective, single-center studies. To date, no prospective and randomized comparative study to determine the optimal duration of dual antiplatelet therapy in patients with UIAs after undergoing SAC has been conducted. Also, guidelines for the optimal duration of dual antiplatelet therapy after SAC has not been established. This study is the first prospective, randomized and multicenter trial to conduct a direct comparison of long-term dual antiplatelet therapy versus short-term dual antiplatelet therapy in patients with UIAs after undergoing SAC. The randomized design of this study has a minimal risk of bias regarding the selection of patients for the long-term and short-term dual antiplatelet therapy groups. In addition, this study minimizes bias by excluding patients who, after undergoing platelet function test before SAC, are at high risk of thromboembolic or hemorrhagic complications during or after the procedure (ARU ≥550, PRU <85, and PRU ≥220) [4,16].
CONCLUSION
This paper details the design and aim of a prospective, randomized and multicenter trial that will determine the optimal duration of dual antiplatelet therapy in patients with UIAs after undergoing SAC. This study will provide evidence and novel insight into the optimal dual antiplatelet therapy duration for UIA patients undergoing SAC.