INTRODUCTION
Advances in anatomical knowledge and surgical techniques have expanded the indications of endoscopic skull base surgery (ESS) in recent decades. The favorable results that have been documented regarding tumor control and neurologic outcomes have contributed to the increased interest in ESS, and ESS is recognized not as an alternative surgical technique but instead as one of surgical approaches that should be considered [36,38,51,55].
The repair of cerebrospinal fluid (CSF) leakage is one of the most pressing concerns, even with the microscopic transsphenoidal approach (TSA). With the significant expansion of the surgical windows with the introduction of ESS, CSF leakage is caused by not only a tear in the diaphragma sellae but also by the wide opening of the basal cisterns or the third ventricle. Therefore, different reconstruction concepts and techniques for high-flow CSF leakage through large skull base defects are required. A grading system was proposed and updated to identify an optimally designed reconstruction strategy, and various reconstruction techniques have been introduced [13,18,32,42,63]. A review on endoscopic skull base reconstruction for large dural defects showed a CSF leakage rate as high as 11.5% [33]. It is evident that the CSF leakage rates dramatically decreased after the introduction of the vascularized flap. Currently, various combinations of reconstruction techniques with a multilayer method have been adopted on an individual basis, and the vascularized mucosal flap continues to be beneficial. However, the vascularized mucosal flap does not provide immediate watertight leakage repair and requires postoperative CSF diversion, such as lumbar drainage, for a better success rate [64]. The more serious concern is that skull base reconstruction can fail even with multilayer reconstruction, including the use of the pedicled flap following CSF diversion, after several days. Lumbar drainage, which is mostly used with CSF diversion after ESS, usually requires the restriction of postoperative ambulation and sometimes causes longer hospital stays and complications, such as deep vein thrombosis (DVT), pulmonary complications, and intracranial events related to intracranial hypotension [8,64].
To our knowledge, there is no surgical technique that achieves an immediate complete repair of high-flow CSF leakage without CSF diversion, except for direct sutures. We introduce a surgical reconstruction technique with artificial materials and a pedicled mucosal flap for immediate watertight skull base reconstruction and retrospectively analyzed the clinical results.
MATERIALS AND METHODS
Patients
This study was approved by the Institutional Review Board of Seoul Natinoal University Hospital, Seoul Natinoal Uniersity Bundang Hospital, and Asan Medical Center (No. H-1910-061-1071) and included patients who underwent multiple onlay reconstruction with fibrin sealant patch (FSP), hydroxyapatite cement (HAC), and pedicled nasoseptal flap (PNF) for grade 3 high flow CSF leakage following ESS for intracranial tumors from October 2012 to October 2018 [13]. Therefore, we excluded patients who had grade 1 or 2 CSF leakage by intradural extraarachnoid tumors, such as usual pituitary adenomas. Clinical data encompassing the preoperative demographic details, pathological results, CSF leakage, and postoperative infection were retrospectively collected and interpreted based on the surgical approaches. Magnetic resonance (MR) images with gadolinium contrast and nasal cavity computed tomography (CT) images were verified in all patients before surgery to elucidate the details of the intracranial anatomy and individual variations of the nasal cavity. Brain CT scans with 1 mm slices were performed immediately after the surgery to identify the state of rigid reconstruction and intracranial hemorrhage, and postoperative MR images were acquired within 48 hours after surgery.
Preoperative neuroendocrinological evaluations were dependent on the presumptive diagnosis by the imaging features and the tumor locations. In parasellar tumors, basal hormones, including serum thyroid-stimulating hormone, free T4, adrenocorticotropic hormone, cortisol, prolactin, growth hormone, insulin-like growth factor-1, luteinizing hormone, follicle-stimulating hormone, estradiol, progesterone, and total testosterone, were measured from the serum sampled in the early morning. A rapid adrenocorticotropic hormone stimulation test was performed in the suspected patients. The visual field defects were evaluated with Goldmann or Humphrey perimetry. The same items of the preoperative evaluation were performed again in the follow-up 3 months after surgery.
Indications
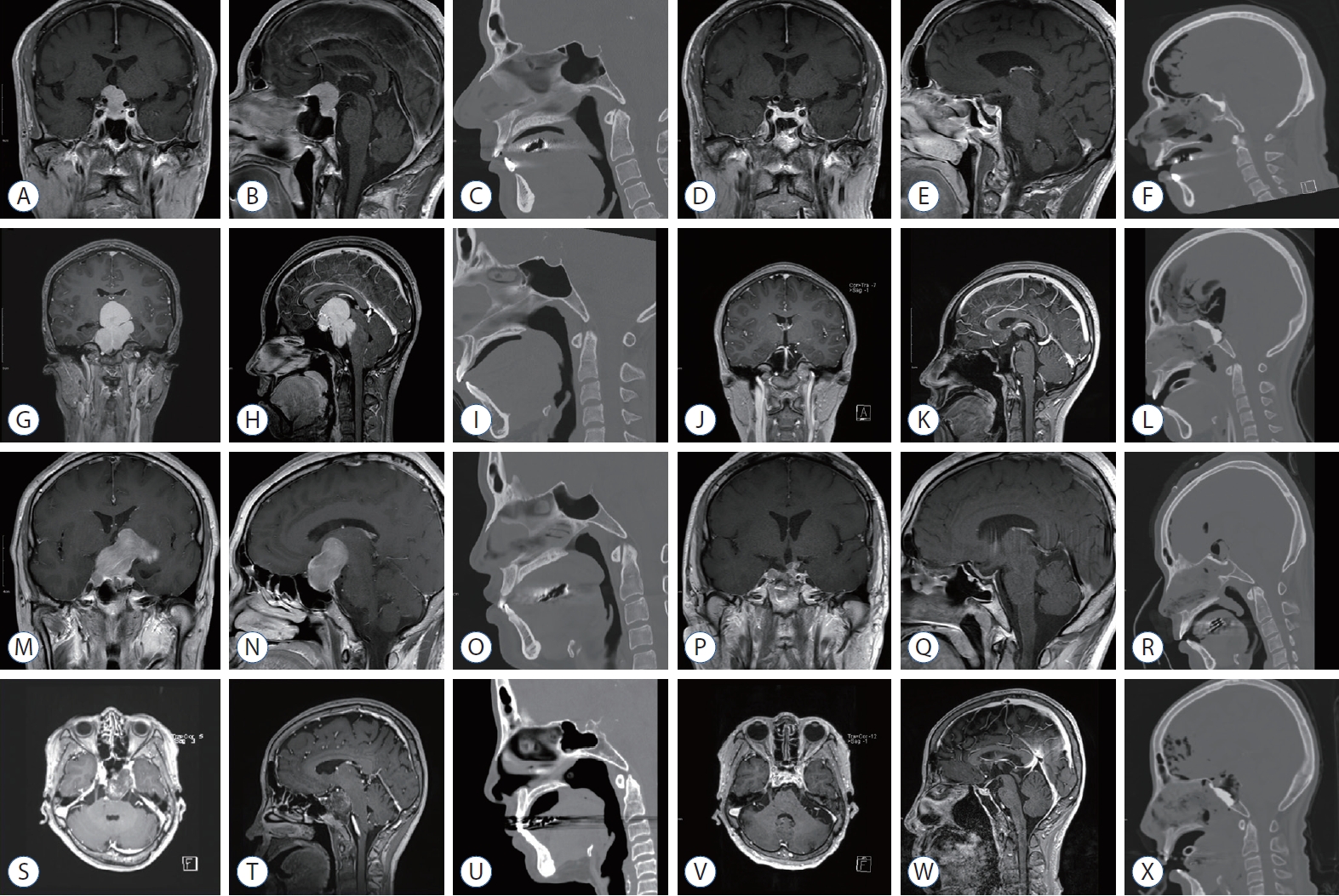
We adapted our multiple onlay watertight reconstruction techniques to reconstruct high-flow CSF leakage (grade 3) after ESS in patients where all boundaries of the surgical window were surrounded by rigid the skull base bone with reliable hardness and a sufficient width to anchor the HCA and graft the PNF reliably [13]. As seen in the lower clivus approach or trans-odontoid approaches, the surgical windows surrounded by any soft tissue, regardless of size, were contraindicated (Fig. 1). An eroded or thin surrounding skull base bone, which is typically observed in pituitary adenomas with sellar enlargement, was also repaired with other reconstruction techniques. We also avoided this technique in patients with excessive bloody or wet surgical environments, as these environments make it difficult to achieve a watertight seal in the attachment of the grafts and might cause a crack in the HAC during the hardening process.
Surgical procedures
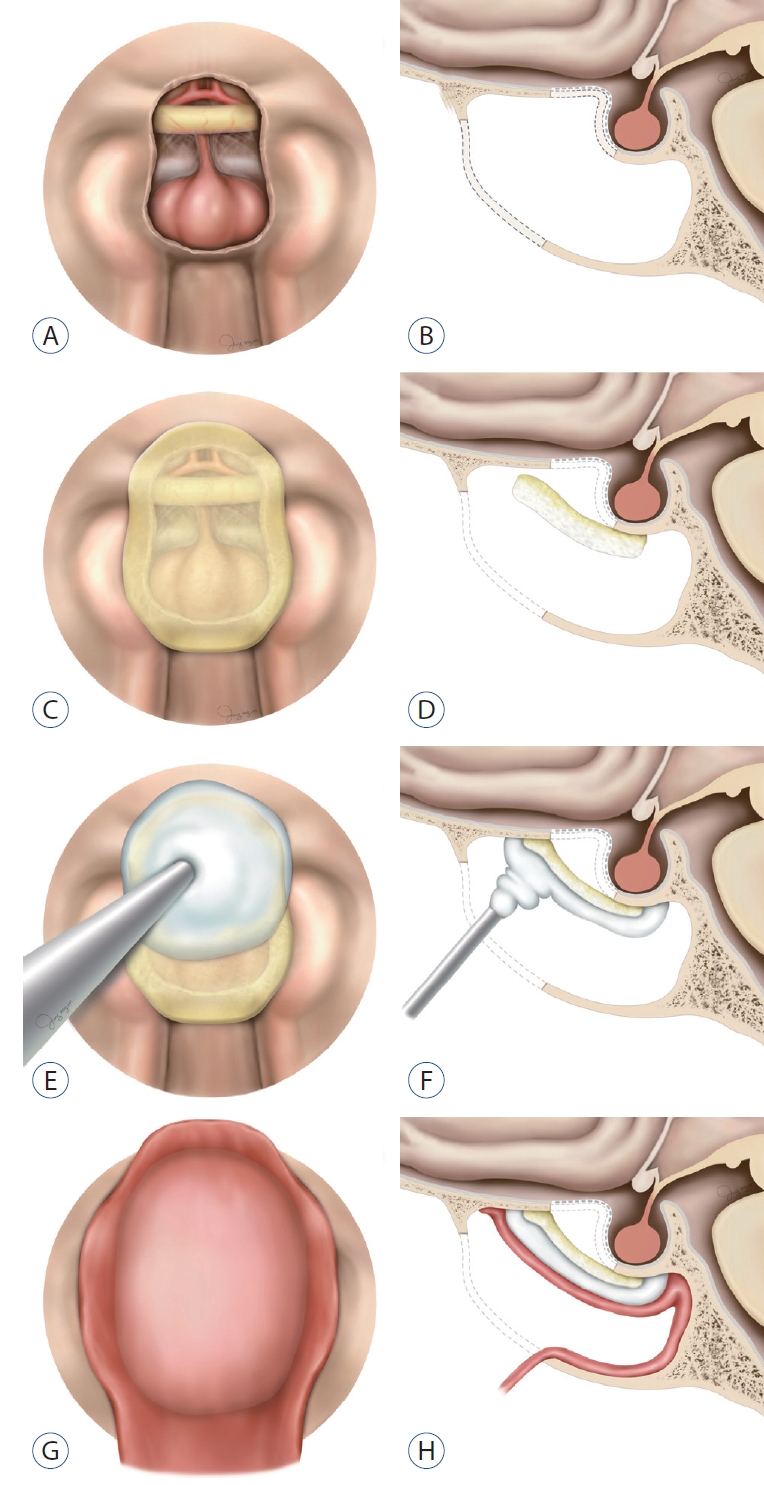
ESS procedures were performed with an image-guided neuronavigation system, and endonasal corridors were adopted [29]. Sufficient sphenoidotomy was performed following storage of the pedicled nasoseptal mucosal flap in the choana. The thin skull base mucosa was removed by approximately 1 cm more than the target skull base bone was, which was drilled to secure a dry grafting site for the multiple onlay grafts achieved by the spontaneous hemostasis of denuded bone during subsequent surgical procedures. Following the individually designed plan for drilling the skull base bone, the midline vertical dural incision was made first, and a bilateral tack-up suture for each dural margin was pulled through each nostril. Then, a horizontal dural incision was made at the end of the vertical incision line and expanded to the lateral end of the exposed dura. The pulled dural window served as a protective barrier for the surgical window from the blood coming from the sphenoid or from between the dural and skull base bone during the operation. The tumor was always dissected and removed with microsurgical techniques, and the details were not different from those in previous reports [14,36,38,54]. The loose approximation of bilateral dura after the removal of the tackup suture was the first step of the reconstruction process. Then, a rectangular shaped FSP (TachoSil┬«; Takeda Pharma, Linz, Austria) measuring 2.5├Ś1.5 cm was attached on the denuded skull base around the bony defect with gentle compression and a cottonoid patty. The additional FSPs slightly overlapped with the previous FSP and were attached to the bony window margin. The sphenoid sinus and nasal corridor were packed with cottonoid patties soaked in 1 : 10000 epinephrine after the complete sealing of the bony defect with FSPs to secure the dry state of the reconstruction site field from the blood coming from the mucosa. After removal of packed cottonoid patties, the FSPs and the exposed skull base bone around the FSPs were completely covered by the injection of HAC paste (HydroSet┬«; Stryker, Kalamazoo, MI, USA) in the dry state. To avoid a defect or dehiscence of the injected HAC from the skull base, we started to inject the HAC from the border of the attached FSPs and then injected it on the FSPs. The packing of diluted epinephrine soaked pledgets with gentle suction over the HAC was helpful in preventing a crack in the HAC during the hardening process by the blood coming from the nasal cavity. The solidification of the HAC paste with sufficient hardness was confirmed by a gentle touch approximately 3 to 5 minutes later. We covered the HAC with PNF and verified that the margin of the PNF was completely grafted on the denuded skull base. Keeping the dry state of the skull base was an important aspect in achieving a completely watertight graft of the multiple onlay materials. We applied oxidized cellulose (Surgicel┬«; Johnson and Johnson, New Brunswick, NJ, USA) and hydrogel sealant (DuraSeal┬«; Confluent Surgical, Inc., Waltham, MA, USA) to prevent the migration of the PNF after surgery. Then, we sutured the thin silastic sheet to the nasal septum to prevent the development of a crust on the flap harvesting site and synechia between the turbinates and septum. The nasal cavity was packed with the absorbable nasal dressing material (Nasopore┬«; Stryker) to prevent epistaxis from the oozed blood and mucosal synechia by mucosal swelling (Fig. 2 and Supplementary Video 1).
Postoperative care and evaluations
There were no limitations in ambulation or coughing after surgery, and we encouraged walking for postoperative lung care and the prevention of DVT. The first endoscopic nasal cavity evaluation was scheduled on the second postoperative day. The packed materials in the nasal cavity that prevented epistaxis from the swelled mucosa were removed, and then the reconstructed skull base was observed with an endoscope to verify the viability of PNF and CSF leakage. We recommended that normal saline mist be pumped frequently into the nasal cavity to prevent a crust from forming on the silastic sheets sutured on the bilateral septal mucosa. We monitored the general medical status, such as fever and serum electrolyte imbalance, which occurs with diabetes insipidus, for at least 5 days and then discharged the patients. Routine nasal cavity examinations were scheduled at 1, 2, 4, and 12 weeks after the surgery. The silastic sheets were usually removed 1 month postoperatively after complete healing of the PNF harvest site was observed. An endoscopic nasal examination was performed promptly to identify CSF leakage in patients with a new-onset headache, febrile sensation or any minor meningeal irritation signs. Then, the lumbar puncture for the CSF examination was performed to determine whether CSF leakage occurred. Meningitis was diagnosed when the cell index was over 4 because a diagnosis in the early stage of infection can be missed due to the surgical debris. Empirical antibiotics were prescribed before the CSF culture results were obtained and then the antibiotics were modified to target the isolated microorganism.
Data analysis
The demographical features, pathological entities, surgical approaches and complications were descriptively analyzed. We attempted to identify the risk factor for postoperative infection using FisherŌĆÖs exact test. We used SPSS software (version 24.0; IBM, Armonk, NY, USA) for data collection and statistical analyses.
RESULTS
Patients
This study enrolled 230 patients who underwent skull base reconstruction with multiple onlay techniques without CSF diversion after EEA from three institutions. The median age and follow-up period were 48.0 years old (range, 14-76) and 25.5 months (range, 1-73), respectively. Craniopharyngiomas were the most common pathologic entity, followed by meningiomas and pituitary adenomas. All pituitary adenomas were giant or supraglandular [54]. Other pathologic entities included germinomas, optic gliomas, epidermoid cysts, gangliogliomas, pilocytic astrocytomas of the hypothalamus, pituicytomas, and atypical teratoid rhabdoid tumors. The goal of surgery was a pathologic diagnosis in cases with germinomas and optic gliomas because of atypical clinical presentations or imaging findings. The demographic data and pathological entities by the surgical approaches are summarized in Table 1.
Preoperative hydrocephalus was found in 36 patients (15.7%), and 44 patients (19.1%) underwent ESS for recurrent tumors. Postoperative steroids were prescribed for more than 1 week in 150 patients (65.2%).
Skull base reconstruction
None of the patients underwent CSF diversion, such as lumbar drainage, after surgery. Postoperative leakage was found in four patients (1.7%) through a pinpoint sized gap between the HAC and skull base. This leakage was caused by an incomplete seal in the margins of the FSPs with HAC. The crack of HAC, caused by the wet state in applying procedure, was found in one case. Flap necrosis also occurred in one of the patients. All defects were removed completely, and the skull base was repaired by the same technique with reuse of the PNF in three patients. Postoperative meningitis was diagnosed in 31 patients (13.5%), and no microorganisms were cultured. The median and mean time to diagnosis of meningitis from surgery was 7.5 and 11.0 days (range, 2-38), respectively. No sequela remained after the management of meningitis. The only risk factor for meningitis was CSF leakage (p<0.001). CSF leakage and postoperative infection are grouped with the clinical factors in Table 2. There were no complications, such as atelectasis or DVT, related to immobilization. All PNFs, except one with flap necrosis, were well engrafted on the onlay HAC and denuded skull base bone, showing complete healing of skull base mucosa.
DISCUSSION
In past decades, ESS has been applied in more in-depth anatomical studies and has involved more advancements in optical and instrumental technologies. It cannot be denied that the introduction of the PNF was one of the most important steps for the popularization of ESS as an innovative solution for skull base reconstruction [24,35]. Currently, multi-layer reconstruction using various materials and techniques with or without PNF has been used in practice because PNFs alone cannot provide complete CSF leakage repair [25,33,37,44,46,53,56]. Various reconstruction methods were made by combining autologous tissues, such as fascia, fat, cartilage, and bone, various allogenic and artificial materials, and CSF leakage was reported ranging from 0 to 25%, comparing with 1.7% of this study [52].
The reconstruction techniques with a multilayer method could be categorized as in- or onlay reconstruction by the relative location of the substitutes to the dura or rigid or nonrigid by the hardness of the substitute. For inlayer reconstruction, a sufficient amount of the free margin dural or bony structures was required to suspend it. Another concern regarding the inlayer technique was the possibility of neural compression by the intradural material because the intraoperative location and shape of neural structures are not normal and are compressed by the tumor or stretched by the intraoperative CSF leakage. There were few reports about neurovascular injury by the packed inlay graft. Still, in many previous studies, it is estimated that the position of inlay graft is stably maintained as the weight of the brain pushes the graft to outward direction after intraoperative CSF leakage and postoperative postural change [21,58]. Therefore, although there has been no report about neurovascular compression by inlay graft yet, in cases of sellar or parasellar locations that is a cluster of microscopic neurovascular structures, neural compression by the reconstruction material can occur with the returning process of neural tissues in the postoperative period, even though it does not occur during the operation. These difficulties of layer reconstruction frequently occur after resection of the tuberculum sellae invading the optic canal. In contrast, onlay reconstruction requires only the free outer dura or bony margin and is associated with a small risk for intradural compression. The need for rigid reconstruction in ESS has been debated because it can be associated with a risk of extrusion of the reconstruction materials, chronic inflammation caused by its avascular feature and mechanical compression of the neural structures in the indented skull base area with the gasket-seal technique [7,18,22]. However, the benefits of rigid reconstruction seem to be evident, as it serves as a protective barrier, preventing postoperative brain herniation regardless of intracranial pressure or brain damage during the manipulation in the nasal cavity [7,17,23].
Regarding the reconstruction materials, autologous grafts have great advantages, such as biocompatibility, resistance to infection, and long-term safety, and they are cost-free [22,27,42,59]. However, the materials can be associated with harvest site complications due to the additional surgical incision, and the resources to be harvested may be limited in terms of number and size [42]. In addition, reconstruction with autologous materials requires a long period of time to achieve completely watertight reconstruction because it is based on the healing process, such as fibrosis, except for when it is performed with direct dural sutures. The most pressing concern is that the CSF leakage rate is as high as 5%, even with CSF diversion, but its beneficial effects have been shown by a prospective, randomized controlled study [8,64]. The use of direct dural sutures with or without substitutes is a unique surgical technique performed to provide immediate CSF leakage repair; however, this technique has been attempted mostly in pituitary surgery, which has relatively large intradural dead space, wide dural margin and bony window due to sellar enlargement, and it requires special surgical instruments, long training procedures and long operation times [2,3,19]. Therefore, the advantages of artificial substitutes, the prevention of complications related to the harvest site, a shorter time to achieve a complete watertight status and the availability of unlimited resources in the amount or design, cannot be overlooked.
Ideal reconstruction materials for ESS should be easy to manipulate in deep surgical fields, compatible with MR images, inert to host reactions, and unlimited to be acquired or designed. Therefore, we adopted the FSP and HAC as the inner and intermediate layer in the multilayer reconstruction, respectively, which are commercially available, safe and widely used in the field of neurosurgical procedures, and covered the HAC with the PNF [1,20,40]. The purpose of each layer resembles the three protective barriers of the brain, which are composed of the dura, skull and scalp. In addition, this concept is the same as that in the layer-by layer reconstruction method of duro-cranioplasty with a rotating scalp flap in transcranial approaches. FSP has been commonly used as a substitute in duroplasty for the prevention of CSF leakage in the transcranial approach and TSA, as it has a reliable repair rate and is safe [11,26,28,31,57,60]. However, it did not provide complete repair of the high-flow CSF leakage. Therefore, we considered it as the first and temporary barrier to CSF and reinforced it with material to achieve watertight reconstruction with HAC. HAC paste has been used for CSF leakage repair with rigid reconstruction for the anterior and lateral skull base [1,5,6,40,41]. The use of HAC in TSA has been attempted with the introduction of injectable HAC because of the deep location of the surgical field with a narrow window. The objectives of using HAC in TSA were to sustain or protect the dura layer with the rigidity of the HAC or to achieve a CSF leakage repair, and these methods showed reliable results [4,12,37]. There is a debate about whether rigid reconstruction is necessary for ESS to prevent brain herniation, but there have been few reports [7]. Eloy et al. [17] succeeded in reconstruction without CSF leakage after anterior skull base tumor resection by ESS in all nine patients using consecutive onlay of autologous fascia lata, acellular dermal allograft, and PNF, nevertheless CSF leakage of the anterior skull base is not high-flow. However, the anterior skull base is not the location where high-flow CSF leakage occurs. For high-flow CSF leakage, it is reasonable to use HAC to make immediately watertight until delayed waterproofing by PNF. However, the neo-mucosalization on the exposed HAC in the nasal cavity has been questioned. Therefore, we added the PNF over the HAC and surrounding skull base bone to prevent a crust from forming on the HAC and CSF leakage. However, we experienced a 1.7% CSF leakage rate due to technical errors from the uncovered skull base bone, as there was a small PNF that did not graft on the whole skull base bone around the HAC. Afterwards, we rechecked the margin of the HAC after hardening.
Another advantage of our reconstruction technique is that it does not require the CSF diversion, such as lumbar drainage. No restriction on position and ambulation was necessary from right after surgery. For the transtuberculum and transplanum approach, the majority of approach in our subjects, many simpler methods than ours have shown good outcomes in terms of CSF leakage [9,16,34,37]. However, CSF diversion was necessary for most of the other methods. There has been still debate that PNF necrosis is increased by HAC, but in most cases, PNF necrosis is thought to be caused by torsion of pedicle or infection [10,43,45]. In the cases of autologous bone graft used for solid support instead of HAC, the lumbar drain is required because it is not immediately watertight, unlike HAC. Therefore, we were able to avoid side effects related with the lumbar drainage or long-time bed rest.
The surgical field of ESS is regarded as a clean contaminated wound, and the risk of infection is inevitably higher than that in clean wounds. High-flow CSF leakage carries a higher risk of infection than low-flow leakage due to the lack of physical barriers, such as diaphragma sellae, and difficulty in reconstruction. There were three atypical clinical features in our results. First, the infection rate of this technique was as high as 13.5%, which was higher than the 1.7% CSF leakage rate and much higher than the 3% infection rate in temporal bone reconstruction using HAC [40]. This finding was different from those in previous studies showing a similar or lower ratio of the infection rate to the CSF leakage rate with ESS and highflow CSF leakage [13,36,39,62]. The second feature was that no microorganism was cultured in the CSF specimens. Of course, we could not verify that the negative culture results always corresponded to aseptic meningitis because the isolation rate of the CSF culture was approximately 33% and perioperative antibiotics influenced the culture results [15,30]. The third one was that the time to infection was longer than 8 days (range, 8-38) after the operation in half of the infected patients, which was longer than that of postcraniotomy meningitis. We speculated that these findings were related to the amount of inoculated microorganisms and the inflammation reaction to the foreign body. The FSP and HAC used in the study had innate defects that were susceptible to infection, such as other allogenic materials, and microbiological contamination of the materials appears inevitable in the clean contaminated passage of the nasal cavity. The amount of microorganisms, not enough to cause the meningitis when using an autologous materials, could manifest the overt meningitis after the incubation period in the avascular allogenic material. Therefore, the different amounts of inoculated microorganisms across individuals in the intracranial space might determine the outbreak and timing of overt presentation, even though the same preparation and preoperative antibiotics were applied. We suppose that a more precise diagnostic method of bacterial meningitis based on molecular biological techniques can verify our presumption [49]. The inflammatory reaction after reconstruction with HAC has been documented in transcranial approaches [5,40,47,61]. A pathohistological study on surgical specimen in complicated cases revealed a foreign body inflammatory reaction showing fibrosis, granulation of the tissue, and the presence of neutrophils, lymphocytes, and plasma cell around the grafted material [48,50]. A large number of plasma cells in the surrounding tissue might indicate not only inflammation but also the immune response to material itself [50]. The development of biologically inert materials for watertight rigid reconstruction is mandatory, and stronger materials than FSP may be required to prevent some materials of HXA from influx into the intracranial space.
This study from three institutions had an inherent limitation, as it is a retrospective study, and the results can be biased by the different surgical experiences of the surgeons. However, we introduced a technique that realizes immediate CSF leakage repair and complete skull base healing with commercially available allogenic materials after EES.
CONCLUSION
Our reconstruction technique was easy to implement and provided immediate watertight skull base reconstruction with a reliable repair rate for high-flow CSF leakage in EES, but it was accompanied by an unavoidable risk of infection. Our results showed that the development of more biologically compatible allogenic material is required.