INTRODUCTION
Carotid endarterectomy (CEA) is the gold standard for treating carotid stenosis. CEA has a low incidence of stroke and mortality but confers a high risk of morbidity, including myocardial infarction and cranial nerve injury. Carotid artery stenting (CAS) is rapidly becoming a popular alternative to CEA for treating carotid stenosis, and many reports suggest that it is more effective for treating high-risk CEA cases6,16).
However, the occurrence of intraprocedural embolization is a serious obstacle to more widespread CAS, which has a higher periprocedural stroke risk than CEA. Many studies have reported that embolic showers can occasionally cause permanent neurological deterioration7,1215). Preventative embolic protection devices (EPDs) have significantly improved neurological prognosis3,910,11).
There are 2 general types of EPDs. Proximal balloon occlusion devices cause cessation of blood flow during the stenting procedure via simultaneous balloon occlusion of the external and common carotid artery7,17). Distal filter protection devices capture debris with a filter that is placed in an artery distal to the lesion. However, no definite conclusion has been reached as to which device produces superior outcomes.
MATERIALS AND METHODS
This retrospective, single-center study included patients with symptomatic and asymptomatic carotid stenosis who had been treated with CAS with either of 2 EPDs : a proximal balloon occlusion device or a distal filter protection device.
From January 2011 to March 2015, 61 patients with severe carotid lesions (symptomatic and asymptomatic) were selected for CAS with either Spider-FXв„ў (Covidien, Mansfield, MA, USA) or Mo.Ma Ultra (Medtronic, Santa Rosa, CA, USA) as the distal filter protection device or proximal balloon occlusion device, respectively. The inclusion and exclusion criteria and their adaptation for CAS were designed in accordance with the North American Symptomatic Carotid Endarterectomy Trial standards. Symptomatic carotid artery stenosis exceeded 50% and asymptomatic cases exceeded 70% of carotid stenosis rate1). Passing the instrument through lesions was impossible in three patients, resulting in technical failure in, 1 patient in the distal filter protection device group and 2 patients in the proximal balloon occlusion device group.
We used three different types of carotid artery stents : the ProtГ©gГ© EverFlexв„ў (ev3 Inc., Plymouth, MN, USA) as the open-cell type; Wallstent (Boston Scientific Corp., Natick, MA, USA) as the closed-cell type; and Cristallo Ideale (Invatec, Roncadelle, Italy) as the mixed-cell type.
All patients were premedicated with clopidogrel 75 mg/day and aspirin 100 mg/day for at least 3 days before the intervention. Clopidogrel was continued for at least 1 month after CAS, and aspirin was continued indefinitely. Beta blockers were discontinued at least 24 hours before the procedure, and other medications were continued at the discretion of the referring physician.
Postprocedure MRI was performed in all patients. When neurological symptoms occurred after a procedure, MRI was performed immediately. Otherwise, MRI was performed on the first postprocedure day to confirm any new cerebral ischemic lesions, even if patients were asymptomatic.
Fluid-attenuated inversion recovery (FLAIR) and DW-MRI images were captured using a 3.0T machine (Magnetom Skyra, Siemens, Germany). DW-MRI images were obtained with the following parameters : b values of 1000 s/mm2; repetition time (TR)/echo time (TE)/excitation, 5150 ms/64 ms/1; matrix 150Г—150; field of view (FOV) 220Г—220 mm; section thickness 5 mm; interslice gap 1.0 mm; and total acquisition time, 2 minutes 19 seconds. The FLAIR images were obtained as follows : TR/TE/excitation, 6510 ms/190 ms/1; inversion time 2127 ms; matrix 512Г—251; FOV 220Г—220 mm; section thickness 5 mm; intersection gap 1.0 mm; and total acquisition time 2 minutes 49 seconds. FLAIR images, DW-MRI, and apparent diffusion coefficient maps were used to identify new cerebral ischemic lesions. The number of isolated lesions was counted. All imaging was performed at the our hospital and analyzed by the neurosurgeon who performed the CAS procedure.
Neurologic events were divided into the following categories : transient ischemic attack (TIA) (symptoms of neurologic deficit improving within 24 hours); minor stroke [symptoms of neurological deficit continuing after 24 h, National Institute of Health Stroke Scale (NIHSS) score вүӨ4]; and major stroke (symptoms of neurological deficit continuing after 24 hours, NIHSS score вүҘ5)8).
Student's t-test, Pearson's chi-squared test, and Fisher's exact test were used to analyze and compare the clinical characteristics of the 2 groups. Fisher's exact test was used to examine embolization-related complications, and Pearson's chi-squared test and the Mann-Whitney U test were used to examine the rate and amount of positive results as seen on postprocedure DW-MRI. Two-way analysis of variance with the post hoc Tukey method was used for statistical analysis of stent influence. A p value<0.05 was considered statistically significant.
RESULTS
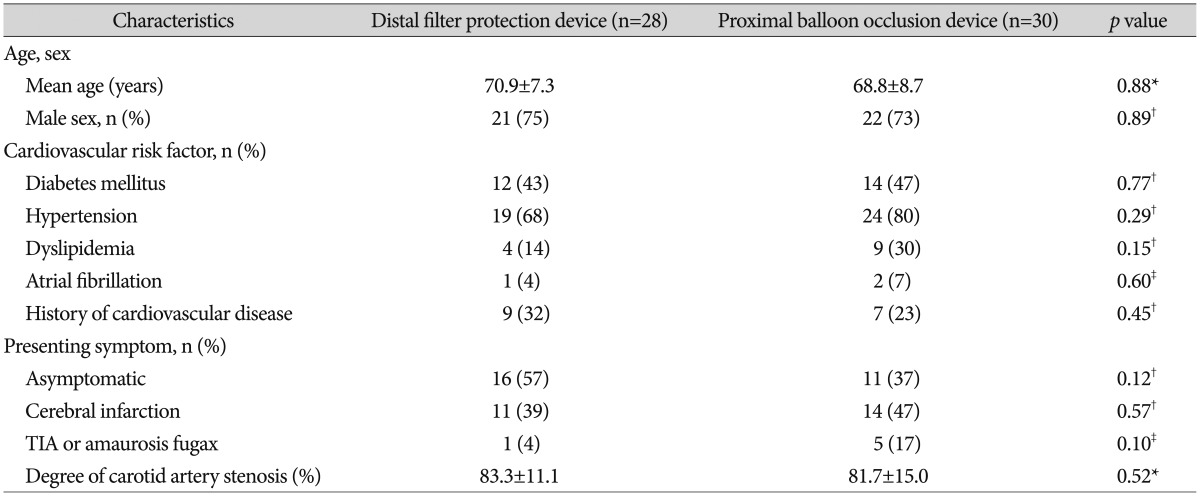
The clinical characteristics of patients in both groups are summarized in Table 1. No significant differences were found between the groups with regard to patient demographics (age, sex); cardiovascular risk factors (diabetes mellitus, hypertension, dyslipidemia, atrial fibrillation, and history of cardiovascular disease); presenting symptoms (including cerebral infarction, TIA or amaurosis fugax, or asymptomatic); or degree of carotids artery stenosis (83Вұ11% vs. 81Вұ15%, p=0.52). In the distal filter protection device and proximal balloon occlusion device groups, clinical and procedural success was achieved in 96.6% and 93.8% of patients, respectively, and instruments failed to pass through lesions in 3 patients (1 in the distal filter protection device group and 2 in the proximal balloon occlusion device group).
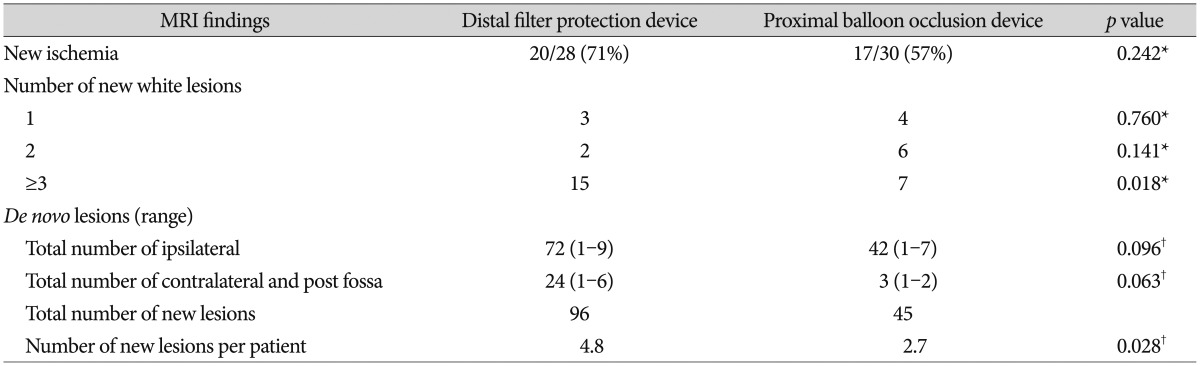
Postprocedure lesions were observed on DW-MRI in 20 patients (71%) in the distal filter protection device group and 17 (57%) in the proximal balloon occlusion device group, with no significant difference between groups (p=0.242). The number of patients who had 1, 2, and вүҘ3 DWI-positive lesions was 3 (10.1%), 2 (7.2%), and 15 (53.6%) in the distal filter protection device group and 4 (13.3%), 6 (20.0%), and 7 (23.3%) in the proximal balloon occlusion device group, respectively, with no significant difference between the 1 or 2 lesion group (p=0.760 and p=0.141, respectively). However, in the вүҘ3-lesion group, the number of patients was significantly lower in the proximal balloon occlusion device group (p=0.018). The number of ischemic lesions per CAS patient was significantly lower in the proximal balloon occlusion device group than in the distal filter protection device group (4.8 vs. 2.7, respectively, p=0.028). In the ipsilateral subgroup, the number of lesions was lower in the proximal balloon occlusion device group, but not significantly (p=0.096). In the contralateral and posterior fossa subgroups, the number of lesions was lower in the proximal balloon occlusion device group, but not significantly (p=0.063) (Table 2).
Ischemic neurologic events were observed in 2 patients (3.6%) in the entire study population. One patient in the distal filter protection device group experienced a major middle cerebral artery infarction with aphasia and hemiparesis the day after the procedure. One patient in the proximal balloon occlusion device group had a TIA. No other significant intergroup differences in the incidence of ischemic neurologic events were observed (p=1.00) (Table 3).
Table 4 shows the number of new postprocedural lesions per patient, as seen on DW-MRI, using 3 types of stents : open cell, closed cell, and mixed type. No interaction between CAS and EPD was found (p=0.206), and postprocedural number of new lesions had no statistically significant relation to type of carotid artery stent used (p=0.588). However, EPD type significantly affected the number of postprocedural lesions observed (p=0.030, Tukey method).
DISCUSSION
In a study by Kastrup et al.10) comparing the outcomes of CAS with and without an EPD, the incidence of both minor and major stroke was significantly lower when an EPD was used. The authors concluded that embolization-related complications rates were reduced (to 5%) by using an EPD during CAS after a prospective protocol. Our study found a lower stroke rate using both a distal filter protection device and a proximal balloon occlusion device [3.5% (1/28 patients) vs. 3.3% (1/30 patients), respectively].
The recent Prevention of Cerebral Embolization by Proximal Balloon Occlusion Compared to Filter Protection During Carotid Artery Stenting (PROFI) study reported by Bijuklic et al.3) randomly compared distal filter protection device with proximal balloon occlusion devices and found that incidence of new cerebral ischemic lesions was significantly different between devices (87.1% vs. 45.2%, respectively)4). Our study showed a higher incidence of new cerebral ischemic lesions in the distal filter protection device group than in the proximal balloon occlusion device group (71% vs. 57%, respectively), but this difference was not statistically significant. However, the number of lesions per patient was significantly higher in the distal filter protection device group than in the proximal balloon occlusion device group (p=0.028). In addition, in the distal filter protection device group, the proportion of patients who developed вүҘ3 lesions as seen on DW-MRI reached 54% (15/28 patients), significantly greater than that in the proximal balloon occlusion device group (23%, 7/30 patients) (p=0.018).
Stabile et al.17) have reported the superior efficacy of the proximal balloon occlusion device for embolic protection. The proximal balloon occlusion device provides neuroprotection through all phases of the CAS procedure, including initial lesion crossing, whereas distal filter protection devices provide neuroprotection after crossing the lesion or allow particles smaller than their pore size to pass through. In addition, a proximal balloon occlusion device can capture particulate debris with higher efficiency. Furthermore, Bijuklic et al.3) reported that distal filter protection device can become overloaded with debris, thus posing the risk of spilling the contents of the filter during retrieval, which can occasionally be difficult.
In an in vitro study, MГјller-HГјlsbeck et al.14) reported that the closed-cell stent design resists particle penetration not only because of its smaller cell size, which does not allow penetration of embolic particles, but also because it has a highly conformable supporting structure. However, no studies have documented an association between stent type and the number of periprocedural embolic events in vivo. Our study clinically showed that the type of stent used does not significantly affect the average number of postprocedural lesions observed per patient.
In 2011, Voeks et al.20) reported that especially age and sex are important risk factors for postprocedural stroke after CAS. In our study, there was no significant difference in age (p=0.88) or sex (p=0.89) as risk factors; in addition, similar demographic data, preprocedure symptomatology, and degree of stenosis were observed, without statistical difference (Table 1). Thus, the frequency of periprocedural adverse events was compared between the 2 embolic protection groups under similar conditions.
Study limitations include the fact that this was not a randomized study. The initial series of patients was treated with the distal filter protection device from January 2011 to July 2013, and the subsequent series of patients was treated with the proximal balloon occlusion device from August 2013 to March 2015, following favorable initial outcomes with the latter device. Therefore, statistical error including selection bias and generalizability may be expected.
Another limitation of this study was that plaque characteristics were not investigated or reported because carotid ultrasonography and/or cervical MRI were not performed. The high-risk group such as patients with unstable, ulcerative, or heterogeneous plaque or those with intraplaque hemorrhage or intraluminal thrombus have a high prevalence of stroke after CAS2,19). Therefore, plaque characteristics should be considered in both groups. These limitations need to be addressed in future investigations.
Major advances in the field of CAS include the introduction of appropriate dedicated stents, better patient selection, improvement in physician expertise, and new cerebral protection devices. Although EPDs have significantly contributed to progress in carotid artery interventions, CAS still carries the inherent risk of stroke. Further studies on EPDs are required.
CONCLUSION
The number of postprocedure ischemic lesions per patient and the incidence of ischemic lesions as seen on DW-MRI were lower in a patients treated with CAS using proximal balloon occlusion device. Compared with distal filter protection device, proximal balloon occlusion device might be more effective in reducing cerebral embolism during CAS.