INTRODUCTION
Traumatic arteriovenous fistulas (AVFs) of the scalp are rarely encountered by the neurosurgeon. AVF of the scalp is the direct connection between the arterial feeding vessels of the scalp and the draining veins without intervening capillary beds. The draining veins or feeding arteries are often grossly dilated, creating a cosmetic deformity. The symptoms are pulsatile mass, bruit, tinnitus, and headache8). The treatment options include surgical excision1,24,67,811,1214,1516,1722), ligation of feeders, transarterial and transvenous embolization5,910,1323), and injection of sclerosing agent21). We experienced a case of traumatic AVF of scalp, successfully treated by surgical excision.
CASE REPORT
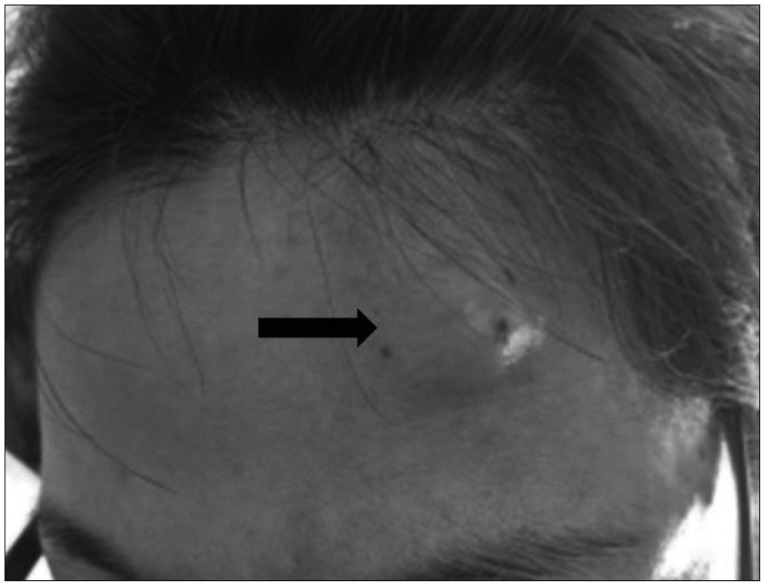
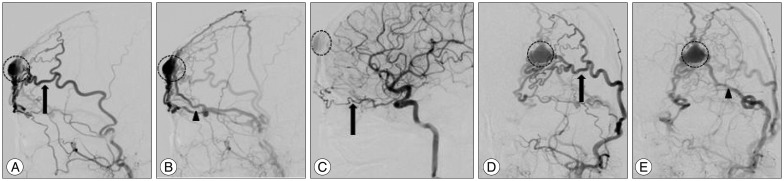
A 42-year-old woman bumped her forehead against the TV about 30 years ago. She noticed the swelling at her left forehead after the trauma; thereafter, a small lesion persisted without any symptoms or size alteration. From 4-5 years ago, "the mass" has gradually increased in size, and showed pulsation. She could hear bruit from the mass when she lay down; the patient also complained about frequent headaches. Physical examination revealed 25├Ś20 mm-sized pulsatile and a round mass on the left forehead (Fig. 1). There was a continuous bruit on auscultation. The pulsation of the mass disappeared with the compression on the proximal portion of the superficial temporal artery (STA). The presumptive diagnosis of AVF was confirmed by selective internal and external carotid digital subtraction angiography (Fig. 2). The main arterial supply was from the left STA, and other feeders were the left deep temporal artery and the ethmoid branch of the left ophthalmic artery. Drainage was seen preferentially into the superficial temporal vein, as well as into the left frontal cortical veins and left superior ophthalmic vein.
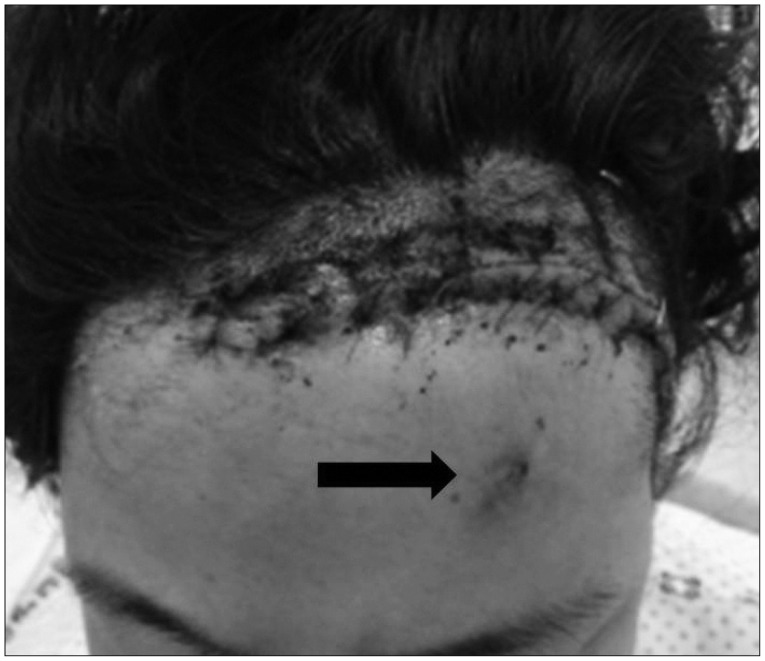
The operation was performed under general anesthesia. A curvilinear 10 cm skin incision was made on the inner part of hairline because of a cosmetic problem. The right STA and AVF were gently dissected from the adjacent subcutaneous tissue. The largest feeder was from the STA and was controlled with a hemoclip. Other vessels were all coagulated and cut. After operation, all the symptoms and signs disappeared, and no other complications developed (Fig. 3). The pathologic report confirmed consistent AVF.
DISCUSSION
The AVF of the scalp has been previously named cirsoid aneurysm, rasemose aneurysm, plexiform angioma, pulsating anigoma, aneurysmal varix, arteriovenous aneurysm, and arteriovenous malformation8,17). The location of this lesion is roughly evenly distributed among the frontal, temporal, parietal, and occipital regions6). The etiology of the AVF of the scalp is still controversial, however, it may be either of congenital or traumatic origin. Among 64 patients with the AVF of the scalp reported in previous research1,23,45,67,89,1011,1213,1415,1617,1821,2223), 36 patients had the traumatic origin. Traumatic origin splits into incidental injury (28 patients) and iatrogenic injury (8 patients). Iatrogenic injury included hair transplantation3,45), craniotomy1,16), and temporomandibular joint arthroscopy5). Theories about pathogenesis of the congenital AVF include persistence of primitive AVFs, as a sequel to vascular hamartomas, and formation at a site of arteriovenous crossing8). On the other hand, there are two theories about pathogenesis of the traumatic AVFs. One is a disruption of the arterial wall and its vasa vasorum with endothelial proliferation to adjacent veins2). The other is simultaneous lacerations of the artery and the accompanying vein result in a single fistula20).
Management of scalp AVF is difficult because of its high shunt flow, complex vascular anatomy, and associated cosmetic problems. The indication of treatment includes cosmetic relief of the pulsatile mass, prevention of hemorrhage, as well as other symptoms such as headache and tinnitus8). In the majority of cases1,24,67,811,1214,1516,1722), radical surgical excision has been the most common treatment method. Complete excision of the fistula with ligation of all feeding vessels is necessary, as there is a high propensity of these lesions to recur. Incomplete treatment can also cause scalp necrosis and bleeding. Additionally, primary scalp vascular malformation can be excised entirely without significant blood loss and scalp necrosis. However, excision of secondary scalp venous dilatation without treatment of the intracranial component can be life-threatening19). Other therapeutic methods, such as ligation of feeding vessels, transarterial and transvenous embolization5,910,1323), and injection of sclerosing agent21) have been used to treat AVF. In the reported case, we choose the surgical method because of the cosmetic issue and the probability of recurrence with other methods. We applied a hemoclip on the largest feeder (STA), and sacrificed the other vessels with coagulation. No complications were observed, and the patient was satisfied with the outcome.
CONCLUSION
Traumatic AVF of the scalp must be considered if the patient had a trauma and has a palpable thrill and/or pulsatile mass lesion, disappeared after proximal STA compression. There are many different methods to treat these lesions. In the present study, surgical excision under general anesthesia was chosen.