INTRODUCTION
Neurilemmoma is defined as "a neoplasm that arises from Schwann cells of the cranial, peripheral, and autonomic nerves". Clinically, these tumors may present as cranial neuropathy, abdominal or soft tissue mass, intracranial lesion, or spinal cord compression. The terminology regarding neurilemmoma may be confusing with neurinoma, neurocytoma, peripheral glioma, perineurial fibroblastoma and schwannoma. Today, neurilemoma and schwannoma are the most frequently used terms in the literature11). They are the most common type of peripheral nerve sheath tumor (PNST), but they are rarely found in deep peroneal nerve sensory branch9,1216,17). We report an interesting case of neurilemmoma of deep peroneal nerve sensory branch that triggered sensory change with compression test on lower leg and induced changes on pre- and post-operative infrared (IR) thermographic images. IR thermography was taken at 23вДГ. It is the first to document a case of thermal change arising from neurilemmoma with compression test. The clinical courses and findings of this case are presented and discussed.
CASE REPORT
A 52-year-old woman had complained of pain at lower back and right leg for 9 months. A local clinician made a diagnosis of herniated lumbar disc (HLD) and performed a pain block on the patient's spine. The symptoms persisted, however, and a mass sized approximately 2 cm by 2 cm was palpated on the lateral side of leg, between right side of tibia and fibula, about 3.5 cm proximal to lateral malleolus. She was subsequently referred to our hospital.
Upon visiting our hospital, she initially presented with sensory change on the dorsal side of the right foot, particularly the big toe. The mass was palpable and soft. Percussion of the mass caused severe pain at fibular area, dorsal side of the right foot, and the big toe. No neurologic signs were examined except for sensory change with compression test and mild numbness at the fibula and dorsal area of foot.
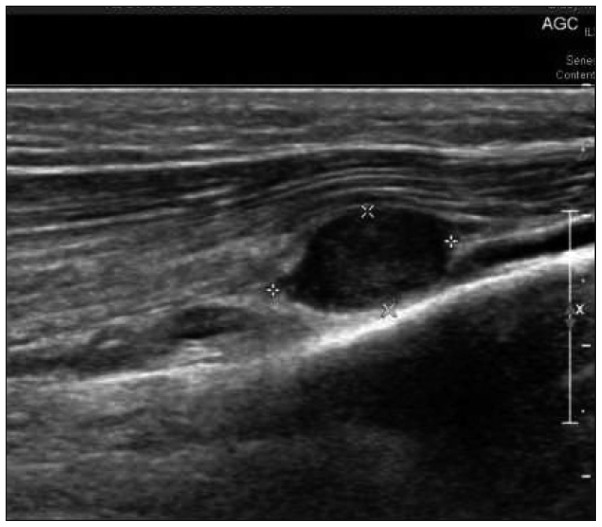
Ultrasonography of the lower extremity discovered an oval-shaped mass sized 1.42 cm by 0.77 cm by 1.12 cm, considered as probably benign PNST arising from the right deep peroneal nerve sensory branch (Fig. 1).
After 1 month, the low back pain was relieved by medication, but right leg pain remained, and an excision of the mass was planned.
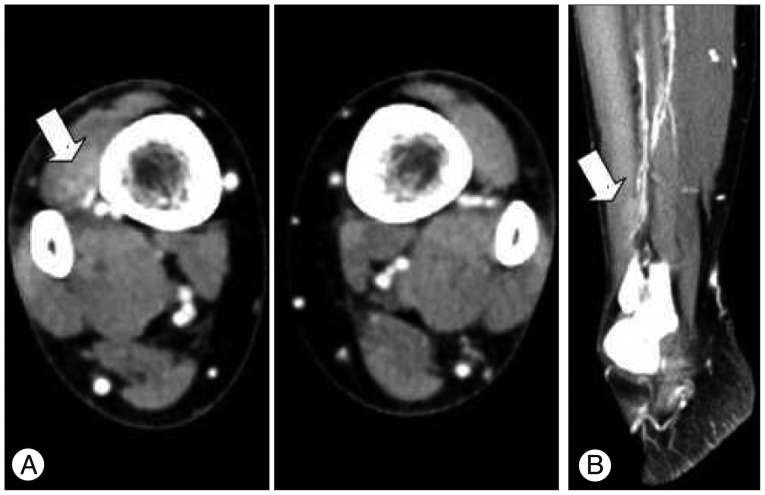
A computed tomography (CT) scan with contrast of the both lower extremities was taken, which revealed a soft tissue mass within the sensory branch of right deep peroneal nerve (Fig. 2).
IR thermography of both legs was performed. Temperature was 31.08вДГ at fibular area, 31.06вДГ at dorsal area. When the palpable mass was compressed, the patient complained of sensory change, severe pain on fibula (upward from mass to below the knee) and dorsal area of foot, especially on fibular area and big toe. At that time, a thermal change was found on IR thermograpy, 31.83вДГ at fibular area, 31.45вДГ at dorsal area : specifically, the temperature of the fibular area was elevated by 0.75вДГ and dorsal area was decreased by 0.15вДГ (Fig. 3) (Table 1). It is similar to area of pain, sensory change with compression test.
A vertical skin incision was made under spinal anesthesia, and sharp and blunt dissection was used to expose the mass. An encapsulated, solitary soft tumor was found on deep peroneal nerve sensory branch. Gross identification demonstrated a mass sized 1.4 cm by 1.2 cm and shaped like a pigeon egg (Fig. 4). The tumor capsule was incised parallel to the running direction of nerve, and totally enucleated, with special attention paid to deep peroneal nerve sensory branch in order to avoid damaging the nerve. The wound was sufficiently irrigated, and compressive sterile dressing was applied. The diagnosis of schwannoma was confirmed by pathologist.
The patient complained of mild sensory change on dorsum of foot, which was relieved partially over 1 month and completely over 2 months of period. IR thermograpy of both legs was performed at one month after operation. Temperature was 31.43вДГ at fibular area, 31.40вДГ at dorsal area. When the excision site was compressed, temperature was 31.49вДГ at fibular area, 31.32вДГ at dorsal area (Table 1). There is no severe sensory change, except mild op wound pain, and thermal elevation like pre-op status. The temperatures at dorsal foot area do not show any significant difference in pre- and post-op status.
DISCUSSION
Neurilemoma, also known as schwannoma, is a common benign tumor of the peripheral nerve11,19). Neurilemmomas usually arise at the intracranial cavity but may be found on other sites of the body. However, its involvement in the leg is unusual5). Odom et al.14) reviewed previous literature and reported that schwannoma of the leg comprise about 7.09% of all cases.
The initial impression of our case was herniated lumbar disc (HLD), which was ultimately found to be incorrect. There has been a previous case where a patient with schwannoma of the peroneal nerve presented with sciatica, which was initially misdiagnosed as HLD13). This patient's perceived sciatic pain or L5 dermatomal pain could have lead to the misdiagnosis. In our case, the patient underwent several sessions of pain block in a local hospital, and there was no clear sign of improvement of low back pain.
Causes of nerve irritational symptom include HLD, ischialgia, piriform muscle syndrome, polyneuropathy, pernoneal nerve trauma, pressure upon peroneal nerve due to wearing immobilization, fracture or expansive process in the region of tibial head, lipoma, ganglioma, synovial cysts from popliteal region, anatomic variability, and others14), and differential diagnosis should be made after considering the innervation of the deep peroneal nerve.
The diagnostic modalities available for the differential diagnosis include CT scan, ultrasonography, magnetic resonance imaging, and electromyography, among other3,1420). Simple radiographs are not of much value when a patient presents with neurologic symptoms. Ultrasonography has been considered as a useful screening tool3), but it is difficult to perform such costly examination from the onset.
Our department has used IR thermograpy examination as one useful alternative method. This examination measures the change in temperature radiating from the body resulting from alteration of subcutaneous capillary blood flow. Thus, for the precise examination, it is important to maintain a constant temperature and environment in thermography laboratory. The thermography result according to changes in the environment can cause errors. This was first used by Lawson in 1956 for the diagnosis of breast cancer8) and is now being used as a novel method objectively quantifying the subjective sense of pain2).
In order to minimize the errors, our thermography lab maintains temperature at 23вДГ, we use difference between temperature of before and after compression of the lesion. The IR thermograpy demonstrated thermographic changes when the neurilemoma induced sensory change with compression test on the fibular area, dorsal side of foot, and the big toe. The area of thermographic change was found to be related to the path of deep peroneal nerve sensory branch.
In HLD accompanied by leg pain, hyperthermic regions resulting from local dilation arise on the posterior lumbar skin that correlates to anatomic site of the compressed nerve due to antidromic stimulation. The information is transmitted to the recurrent meningeal nerve, or sinuvertebral nerve, located at the spinal cord, and consequently, the autonomic output caused by the reflex arc leads to local vasoconstriction and hypothermia2,8).
In our case, however, there was greater blood flow at the pain site, which further increased upon inducing sensory change with compression test, resulting in hyperthermia (Fig. 3). Such results obtained from IR thermograpy was of great assistance in diagnosing the disease.
While the degree of pain intensified in accordance with compression test, vasodilation and increased temperature of the skin was observed, rather than hypothermia and vasoconstriction caused by sympathetic nerves as seen in HLD. This may be explained by autonomic dysfunction following nerve injury (in this case, tumor growth on peroneal nerve sensory branch), including changes of the sympathetic tone and norepinephrine synthesis1).
Sympathetic nervous system usually induces vasoconstriction by secretion of adrenaline, but sometimes, the cholinergic fibers within the sympathetic nerves releases acetylcholine, which may cause vasodilation and diaphoresis10,15). The former may be more significant in HLD, whereas in our case, the latter may have been the stronger factor.
Vasodilation resulting from the stimulation of the dorsal root, which is thought to be a separate entity from sympathetic nervous system, has been discovered. This arises from spinal gray matters, and the preganglionic fibers passes the dorsal root and dorsal root ganglions, changing postganglionic fiber and ultimately, peripheral ganglions and skin temperature21). Furthermore, parasympathetic nerves are also involved in regulation of skin temperature, which may be a clue explaining the rise in temperature at fibular area and cutaneous blood flow following sensory change with compression test.
Interestingly the temperatures at dorsal foot area do not show any significant changes and were elevated more than fibular area.
The study performed by Zhang et al.21) presents thermal data of the upper body measured indoor at 23вДГ. In this case, the mean temperatures of upper body sectors are distributed from 29вДГ to 32вДГ. This study demonstrates lower extremity temperature of our case, being maintained at 31.08вДГ to 31.83вДГ regardless of compression. In other words, our case of IR thermography data follows the temperature distribution pattern obtained at 23вДГ indoor.
The magnitude temperature of difference between left and right side of the same anatomic location was 0.1, 0.2, 0.3, and 0.4вДГ regardless of indoor temperature (20вДГ or 23вДГ), in both 1995 and 1999 study21).
Therefore, the thermal symmetry of the superficial skin is maintained in our case. The elevated temperature of the foot dorsum compared to the fibula before the surgery (Table 1) may be attributed to tumor effect. The situation where the temperature of dorsum was 0.58вДГ higher instead of 0.3вДГ was determined as abnormal6).
This is also well demonstrated in Uematsu, where carpal tunnel syndrome was correlated with electromyography (EMG)18). The degree of median nerve lesion was classified as mild, moderate, or severe according to EMG findings, and mild and moderate compression group demonstrated thermal elevation while in severe compression group, both thermal elevation and depression was observed. In other words, palmar temperature rises as the severity of median nerve compression increases and then drops as thenar muscle atrophy develops as the result of chronic severe carpal tunnel syndrome.
Since peripheral nerves include sympathetic nerves involved in vasoconstriction of the anatomic area, the tumor located at sensory branch of the deep peroneal nerve may have suppressed the vasoconstriction of the surround area, resulting in vasodilation and the following hyperthermia of the right dorsum and toe compared to the left side.
There are numerous other factors influencing skin temperature, including emotional stress and depression, which can affect autonomic dysfunction4), as well as the circadian rhythm, which results in diurnal variation of body temperature7).
IR thermographic change seems to be specific or non-specific. It shows temperature change according to autonomic nervous system tone or change in circulation caused by various etiologies. Therefore, although it shows temperature changes, it does not clarify what the nature of the causative lesion is. Considering these variables, future studies and analyses controlling for these factors may be needed.
CONCLUSION
When the mass, PNST, was compressed, there is a IR thermographic-thermal elevation at PNST proximal part with subjective pain. Mass excision relieves the patient's symptom, and there is no definite thermal change at post-operative IR thermograpy. Those are unique findings of this case.
Differential diagnosis of PNST from HLD is to be made first by clinical findings. However, tumors that occurred in peroneal nerve have a similar symptoms with HLD, or symptoms caused by nerve irritation or compression. Although, IR thermographic findings are not specific, as discussed previously, there are differences in IR thermography, and it is useful and supportive in our case.
Therefore, there are possible usefulness of IR thermography in evaluating symptoms caused by nerve irritation or compression, and possible limitation from various etiologies. Further study will be needed to clarify which range of temperature change can be interpreted as significant result and to get specific result without numerous other factors influencing skin temperature.