INTRODUCTION
Parkinson's disease (PD) is a progressive neurodegenerative disorder associated with various motor and non-motor features that adversely affect function to varying degrees depending on the patient7). PD typically affects patients in the seventh decade, and the cardinal signs of PD include resting tremor, rigidity, bradykinesia, and postural instability. In addition, a stooped posture and masked facies are other significant findings in patients with PD. Several spinal deformities including camptocormia or bent spine syndrome, anterocollis, scoliosis, myopathy-induced postural deformity, and Pisa syndrome are also associated with PD1,2). The frequency of kyphoscoliosis in patients with PD is approximately 7%, which is much higher than that of scoliosis in an age-matched population without PD12).
The therapeutic options for PD range from medical treatment to neurosurgical treatment, including deep brain stimulation of the subthalamic nucleus and intramuscular botox injections. Surgical correction of these deformities should be considered for patients who have reached a severe stage in order to correct the deformity and restore mobility and functions3). Spinal surgery in patients with PD is very challenging, and is associated with a high rate of postoperative complication and surgical revisions due to instrument failure. Here, we report a case of PD with a fixed spinal deformity that was treated with a relatively short segment fixation and corrective fusion surgery.
CASE REPORT
History and examination
A 70-year-old female patient presented with complaints of stooping associated with severe back pain radiating to the left lower limb for a period of 3.5 years. The patient was unable to lie on her back comfortably and reported severe depression due to her condition. She had previously received a diagnosis of PD, for which she had taken regular oral medications for the past 10 years. The patient had a history of multiple spinal surgeries (total of 4) due to instrument-related failures for neurogenic intermittent claudication and stooping; however, none of the surgical interventions had improved her pain or stooping posture. The patient had significant kyphoscoliosis on examination, but the straight leg raise test, Patrick's sign, and sciatic nerve compression tests were all negative. Detailed motor and sensory examinations were conducted, which showed that her left ankle dorsiflexion was weaker than that of the right (Grade 3/5 and 4/5 respectively); similar results were seen for big toe dorsiflexion (Grade 3/5 and 4/5 respectively). The patient had hypoesthesia in the Lt L5 dermatome, and deep tendon reflexes were bilaterally hypoactive.
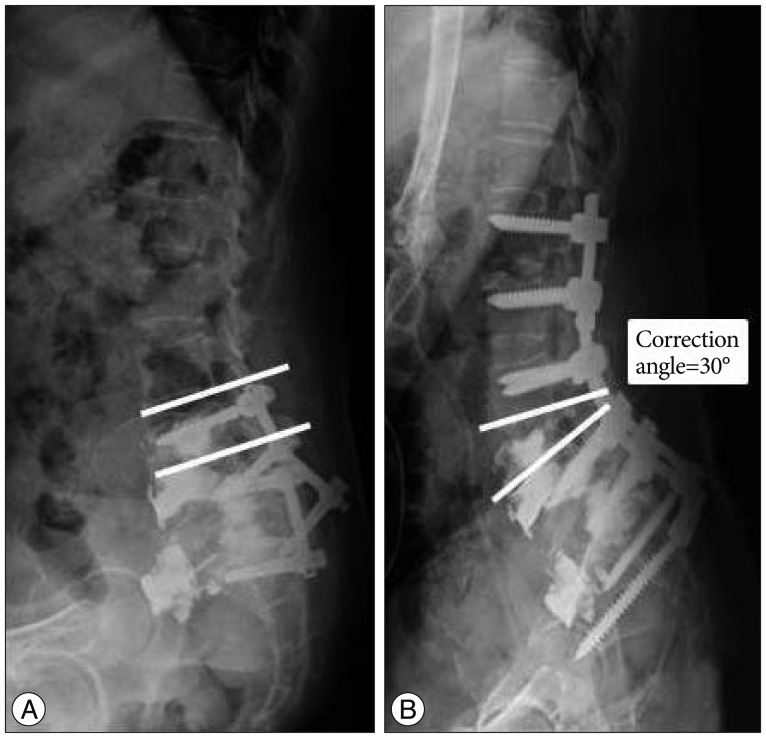
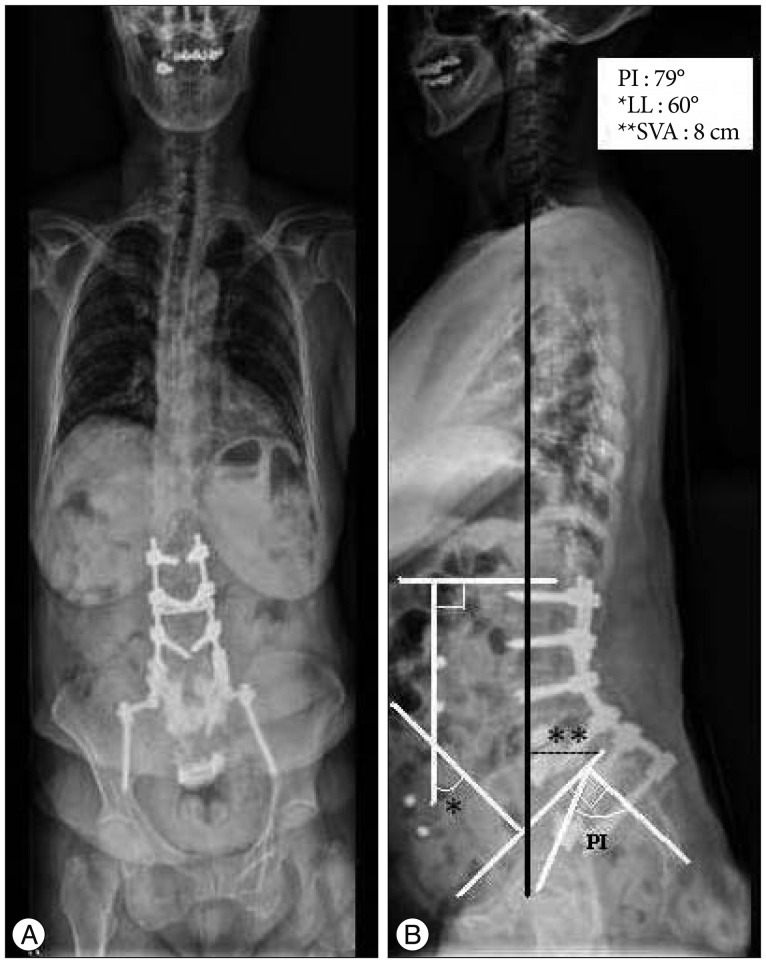
Preoperative X-rays (Fig. 1) showed generalized osteoporotic changes with pulling out of the L5 screws and rods and marked sagittal imbalance. X-ray also revealed compensatoryreactive thoracic straightening and cervical hyperextension, which was apparent from the patient's photograph. Pelvic and spinal sagittal parameters were calculated, which clearly revealed the degree of sagittal imbalance present in the patient.
Operative procedure & postoperative course
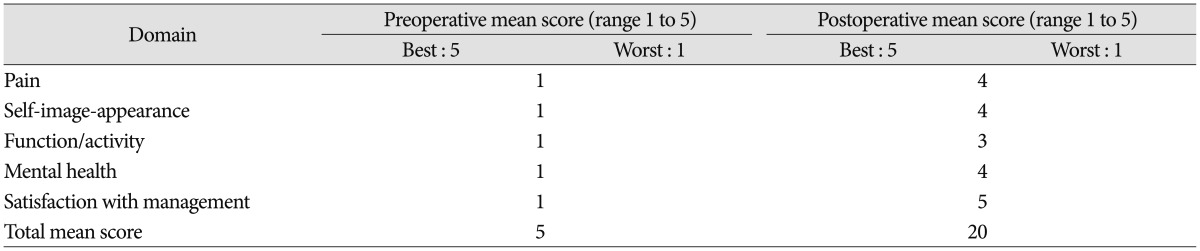
Considering the patient's degree of deformity and pain, we elected to perform revision surgery. Pedicle screws and rods were reinserted from the L1to S1 levels with iliac screws after performing a partial pedicle subtraction osteotomy (PPSO) at the L4 level with removal of the intervertebral discs at the level of L3-4 (Fig. 2). The patient's intraoperative and postoperative periods were uneventful, and she was able to walk with a straight back without any support a few days postoperatively. Follow-up X-rays obtainedapproximately 18 months after surgery (Fig. 3) showed significant improvement in her spinal parameters and kyphoscoliosis. Pre and postoperative surgical outcomes were measured with Modified Scoliosis Research Society-23 Outcome Instrument scoring system (Table 1). A mean postoperative score of 20 out of 25 indicated a satisfactory outcome.
DISCUSSION
Surgical management of fixed spinal deformities in patients with PD is challenging. Indeed, due to disease progression itself and ongoing osteoporosis, both the treating surgeon and patient need to be aware of the increased risk of recurrent kyphosis and instrument failure, which can necessitate multiple revision surgeries. The literature on this topic is relatively sparse, and there is no established consensus regarding standard management of fixed spinal deformities in patients with PD. However, Upadhyaya et al.15) suggested a treatment algorithm for patients with PD and spinal deformities, in which they advocated performing deep brain stimulation surgery (DBS) first for PD patients followed by a short-segment spinal decompression for myelopathy or radiculopathy. However, they indicated that if patients do not meet the standard criteria for DBS surgery, then a short-segment spinal decompression and fusion alone can be performed. They further emphasized the importance of performing long-segment spinal deformity correction and decompression only in those patients with minimal co-morbidities and with high motivation. Unfortunately, long-segment spinal fixation in camptocormic patients is associated with a complication rate of nearly 100%15).
In the present case, our patient had already undergone four spinal surgeries prior to visiting our center. The patient initially underwent an anterior lumbar inter body fusion (ALIF) of the L3 to S1 level followed by posterior decompression and pedicle screw fixation (PSF). Unfortunately, the screws and cage pulled out and she underwent an anterior augmented pedicle screw and cage insertion surgery. Following augmentation surgery she complained of leg pain due to L4 root irritation. Thus, a revision surgery involving removal of the L4 pedicle screw was performed. Since all of these procedures were performed outside of our center, no proper surgical records or clinical radiographs could be obtained during the patient's first visit to our center. The lumbosacral X-rays taken at our center clearly showed the presence of instrument failure with loosening of the S1 screws and displaced rods, which led to our diagnosis of iatrogenic flat back syndrome.
The previous ALIF and PSF surgeries in our patient had been performed well, and the initial presentation of the patient was attributed to spinal stenosis. The patient had obvious osteoporosis and was in a progressive state of PD, and thus there was no proper fusion of the inter body cage which led to loosening of the screws. As a result, the patient had previously undergone bone cement augmentation cage placement with screw fixation in order to resolve instrument failure. Many studies have been performed for the use of bone cement as an augmentation technique during spinal fusion surgeries of osteoporotic bones5,610,17). However, augmentation alone is not sufficient for preventing construct failures. In the patient described in this report, we could have corrected both construct failure and sagittal imbalance via a transperitoneal approach; however, this involves manipulation of several vascular structures and other anatomical structures around the retroperitoneum. As our patient had a history of multiple anterior surgeries, the likelihood of intraoperative and postoperative complications was considered high, and thus an anterior approach was avoided. In addition, stooping was not the primary complaint in our case. Specifically, the patient had stooping as a result of compensatory thoracic straightening with further cervical hyperextension to maintain the vertical gaze, and through interviews and physical examinations we were able to associate her symptoms to spinal stenosis. Based on this diagnosis, we performed a Grade IV osteotomy13) at the L4 level (PPSO with L3-4 disc removal). Bilateral iliac screws were inserted along with the pedicle screws from L1 to S1 for improved and maximum stability of her spine. Bony fusion was also carried out with autografts.
Spinal surgery in patients with PD is prone to complications for a number of reasons9). The factors contributing to these complications include old age and prevalence of severe osteoporosis, which markedly decreases the fusion rate. Surgical outcomes are further worsened by the pulling out of screws and deteriorating motor function. On the other hand, radiological evidence of good fusion rates among patients treated surgically led Moon et al.9) to conclude that short-segment fusion confined to the lumbar region generally achieves good results. In our institution we categorize such patients under one of the two categories including sagittal imbalance disease and sagittal imbalance syndrome. And in this particular case, although the patient had degenerative flat back, we categorized the patient under the sagittal imbalance syndrome group as she had complaints of mild discomfort related to self-image, pain and functions. In such cases we often perform relatively short level fusion especially in lumbar vertebras even if lumbar lordosis (LL) would not have been restored in accordance with pelvic incidence (PI). Had the patient complained of moderate to severe discomfort, we would have categorized under the sagittal imbalance disease category and a relatively long level (thoracic included) fusion with resultant LL exceeding the PI value would have been considered. In our case, the patient's major complaints were related to claudication without any complaints related to camptocormia hence we considered relatively short level fusion surgery is justifiable.
In a case series of 14 patients, Babat et al.2) reported the increased risk of postoperative instrument failures and revision surgeries,and went on to propose a mechanism of ongoing kyphosis adjacent to the levels operated in PD patients. They suggested the primary causes of the revisions to be adjacent segment disease, material failure or pullout, pseudoarthrosis, and infection. Likewise, a case study of 12 patients with PD undergoing corrective spinal surgeries was published by Bourghli et al.3), who reported increased incidence of instrument failure and need for revision surgeries in such patients. Another explanation for surgicalcomplications in PD patients might be the coexistence of osteoporosis and Vitamin D deficiency resulting in overall reduction of bone mineral density9). These etiologies were clearly observed in our patient. In addition to progressive degeneration, improper reconstruction of the spino-pelvic balance with a special focus on LL8) resulted in progressive kyphosis in our patient, which eventually led to screw failures and revision surgeries. Indeed, radiographic examinations clearly revealed the presence of severe osteoporosis and degenerative changes; however, after performing osteotomy with pedicle screw insertion from L1 to S1 along with iliac screws insertion, the sagittal balance was maintained, resulting in correction of the deformity. Both Bridwell et al.4) and Wadia et al.16) advocated for the use of PSO to gain further sagittal plane correction up to 30° to 40°. In a case report of camptocormia in PD, Peek et al.11) emphasized the establishment of substantial forces on the caudal end for stability along with multiple fixation points and anterior column support while performing revision surgeries.
With the advent of cutting-edge medical procedures leading to a longer average life span, age-related debilitating diseases are becoming more common. PD is one such example, and causes not only physical debilitation, but emotional and economic effects as well. It is estimated that camptocormia is present in 7% of patients with PD14), which indicates the high probability of corrective spinal surgeries and need for multiple revisions in these patients. Although spinal surgeries, especially revision surgeries in patients with PD are regarded as complicated and unfavorable outcomes are common, we were able to achieve a good result in one such patient.
CONCLUSION
Spinal deformitiesare very common in patients with PD, but deformity-correcting surgeries in such patients should be performed cautiously due to the increased incidence of intraoperative and postoperative complications including instrument failure. Thus, we concluded that revision surgery in patients with PD can be undertaken only after proper planning, and should involve restoration of sagittal balance and stabilization. Importantly, even a short segment fixation and corrective fusion surgery can be beneficial in such patients. Nevertheless, the most important aspect of surgical treatment in patients with PD is the realization that unfavorable surgical outcomes are inevitable due to the natural course of the disease itself9).