INTRODUCTION
Whiplash injury is a neck injury caused by sudden forward and backward movements of the head during rear-end automobile collisions like the motion of a whip. It is also called cervical sprain or acceleration-deceleration injury5). The term of 'whiplash' was first used in 1928 to describe the mechanism of delayed neck injury after motor vehicle accidents10). In more past, it was described as spinal concussion7). More severe and chronic status is referred as "whiplash associated disorders"24). The incidence of whiplash injury is reported to be 28-834/100000 (person) per year8). Whiplash injury is mainly caused by rear-end collision but also resulted from head on/side collision. The injury is observed in 40% of traffic accidents but also found after trauma such as diving accidents. Whiplash injury was found in 38% of passengers but other injuries were reported only in 0.7%. Also, cervical spine soft tissue injuries occurred in 16% of traffic accidents and in 38% of rear-end collisions but they increased to 20% when the seat belt was fasten and decreased to 8% otherwise19). Cervical spine soft tissue injuries were mainly occurred after low speed rear-end collisions. However, painful experience secondary to these injuries is subjective and it is difficult to visualize the symptom. There is no diagnostic tool to objectively demonstrate these symptoms yet. Therefore, there is a lack of objective data reflecting pain.
This study aims to objectively visualize the neck and shoulder pain and any improvements before and after the treatment of whiplash injury using visual analogue scale (VAS) and infrared (IR) thermography.
MATERIALS AND METHODS
IR thermography was performed for 42 patients who were diagnosed with whiplash injury in our hospital between March 2008 and December 2013 (Table 1). Whiplash injury was diagnosed with symptoms, even though it was normal in imaging study. After 2 week conservative treatment, the results of IR thermography and VAS were compared with immediately initial assessment after injury (Fig. 1).
IR thermography was performed in a room without supply of light and heat. The room with consistent airflow and a low humidity was used for IR thermography. The test was performed without light and heat and the room temperature was maintained at 23-25℃ (recorded by the thermometer installed the room or the thermometer of the heating system). We used Digital Infared Thermal Imaging equipment of Dorex company for IR thermography. Subjects kept for about 15-20 minutes without upper garments so that they could accommodate the room temperature and eliminate abnormal thermal differences. All patients were conservatively treated for 2 weeks after initial whiplash injury (bed rest and NSAIDs).
The thermal differences (ΔT) of the anterior and posterior neck and the right and left shoulder were compared to evaluate the symmetry and to obtain basic data. Then the changes in thermal difference (ΔdT) before and after treatment were analyzed. The normal control thermal values were referred to the previous study29). Neck and shoulder pain was assessed using VAS immediately after the injury and after 2 week conservative management and the change in difference (ΔVAS) was analyzed. Data was analyzed by paired t-test and bivariate correlation test using SPSS 20 (SPSS Inc., Chicago, IL, USA). Significance was determined when p value was less than 0.05.
RESULTS
There were 19 male and 23 female patients and the mean age was 43.12 years (range; 21-58 years). There were 36 cases of traffic accidents and 6 cases of trauma. ΔT of the anterior and posterior neck and the right and left shoulder, and ΔdT in thermal differences before and after treatment were analyzed. In addition, VAS of neck and shoulder immediately after the injury and after 2 week conservative management was measured and ΔVAS were analyzed.
IR thermography results (ΔT & ΔdT)
The initial skin surface temperature was 34.71±2.72℃ at the anterior neck, 34.64±2.81℃ at the posterior neck, 33.91±2.57℃ at the right shoulder and 33.76±2.62℃ at the left shoulder. On the completion of 2 week conservative management, the skin surface temperature was 33.99±2.82℃ at the anterior neck, 34.03±2.81℃ at the posterior neck, 33.04±2.61℃ at the right shoulder and 33.08±2.63℃ at the left shoulder. The skin temperature of the neck and shoulder immediately after injury showed 1-2℃ hyperthermia than normal. After two weeks, the skin temperature was almost normal.
ΔT of the anterior and posterior neck and the right and left shoulder immediately after the injury were 0.3±0.16℃ and 0.38±0.2℃, and those after the conservative treatment were 0.28±0.19℃ and 0.16±0.10℃, maintaining the symmetry. They didn't exceed the criteria (ΔT<0.5) for test errors or pathologic conditions and were found to be significant (Table 2).
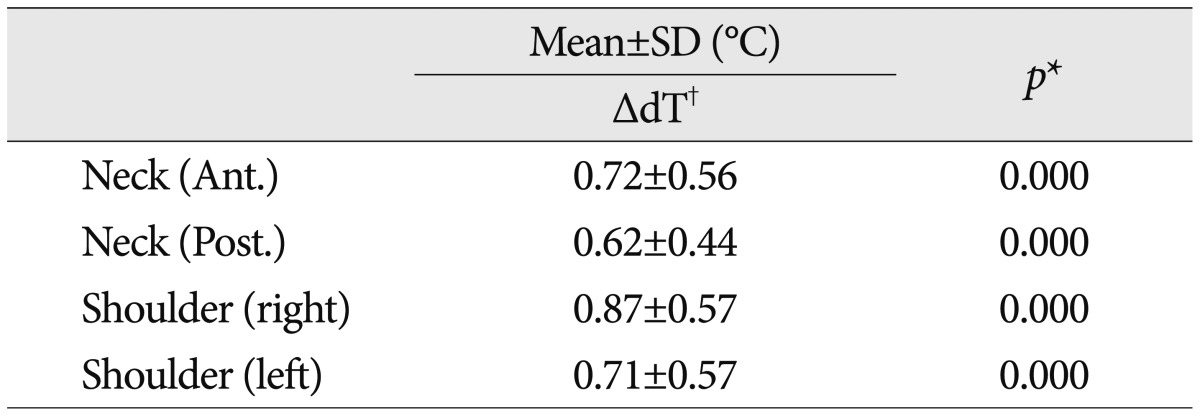
ΔdT was 0.72±0.56℃ at the anterior neck, 0.62±0.44℃ at the posterior neck, 0.87±0.57℃ at the right shoulder and, 0.71±0.57℃ at the left shoulder. These changes were statistically significant (p<0.05) (Table 3).
The thermal difference after immediately injury is higher than normal value, but it gradually decreased after two weeks.
VAS results (VAS & ΔVAS)
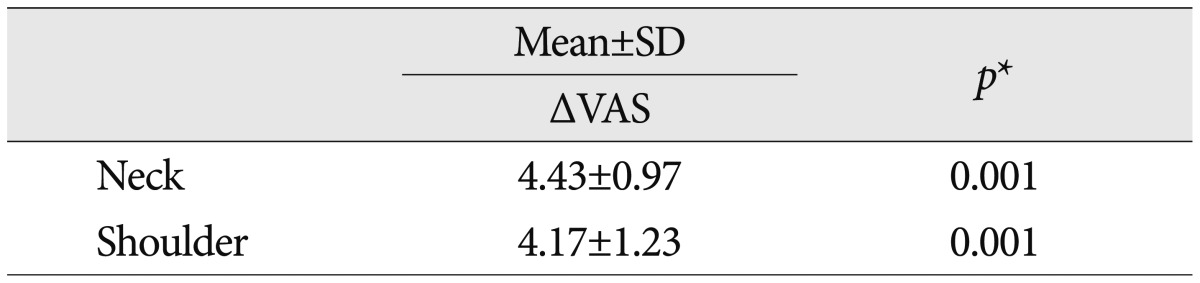
VAS for neck pain was 7.86±0.65 immediately after trauma and was reduced to 3.43±1.06 after conservative management. VAS for shoulder pain was 7.69±0.6 initially but was also reduced to 3.52±1.23 after conservative management (Fig. 2). VAS of the neck and shoulder were significantly reduced after 2 week and were statistically significant (p=0.001) (Table 4).
Also, Bivariate correlation analysis showed that there was significant correlation between ΔdT of the neck and shoulder and ΔVAS in VAS before and after the treatment (the neck; r=0.412, p<0.007) (the shoulder; r=0.648, p<0.000) (Fig. 3).
DISCUSSION
With advances in technology and emergency treatment, the diagnosis of whiplash injury has been increasing. Symptoms of whiplash injury are variously reported from simple neck pain to radiating arm pain28). However, patients are often undiagnosed or misdiagnosed with ruptured cervical disk even with more specific investigations. This reveals the limitation of diagnostic tools for whiplash injury. It was reported that abnormality was started to show on electromyogram 2 weeks after the injury and then investigations were usually commenced. Thermography is a useful tool to visualize and quantify the symptoms of whiplash injury by measuring skin surface temperature19). It is expected that patients will understand better about their condition and any improvement when the imaging is shown. It is also considered to be safer because it doesn't require ionized radiation.
On thermography of a healthy individual without injury, the thermal difference of the anterior and posterior neck and that of the right and left shoulder are trivial, showing symmetric distribution. In a person with injury, there are significant thermal differences. Based on this idea, thermography was developed and first used for the diagnosis of breast cancer15). Thermography is a useful tool that provides objective guidelines for the diagnosis and treatment of pain and the effectiveness of thermography has been evaluated in several studies1,22). Wexler27) first utilized thermography to evaluate pain, there were cold areas on the affected side of the patients with traumatic cervical syndrome and abnormal skin surface temperature related to spinal problem was identified as hypothermia. The majority of traumatic cervical syndrome was sprain in his study.
In studies with myofascial pain syndrome, it was reported that trigger points on thermography could be appeared as either 5-10 cm of hot spots or cold spots14). Furthermore, some studies reported that there were no thermal differences of both sides. Despite of that, it is generally accepted that areas of pain are usually shown as hot spots and areas of nerve damage are detected as hot spots during the acute phase and cold spots during the chronic phase. The diagnostic sensitivity of thermography was high when trigger points were detected as hot spots9,11,14).
Our study was conducted with patients with whiplash injury who complained neck pain and shoulder pain only. Previous studies on the natural history of whiplash injury are mostly small retrospective studies. During a collision, the 6th cervical vertebral body extends upwards as the body moves upwards and the segments above the 6th cervical vertebrae flex at first, creating S-shape. Then the upper segments extend. Extension and flexion are worst 50-100 ms and 100-200 ms after a collision. The lowest collision speed which can cause whiplash injury is estimated to be 8 km/hr. In a head-on collision, the driver's torso and head snap forward and the neck flexes. The movement of head is decelerated by the neck, and the occipitoatlantal joint and the 6th cervical vertebrae are involved in the deceleration force. Then the head and the neck extend due to the elastic force of the occipital and cervical structures. At this point cervical hyperextension cause tissue damages9,12,20). It is important fact that neck is passively moved regardless the direction of the shock. Due to this passive movement, cervical muscle loses an opportunity to prepare for the shock and acquires injury secondary to eccentric contraction4). Sixty percent of the whiplash injury symptoms are neck pain and headache originated from cervical spine and 50% of them are occurred at the 2-3th cervical vertebrae17,24).
There have been a number of studies about the mechanism of whiplash injury which help understand the symptoms. In fact, hot spots were detected on the affected area on thermography immediately after whiplash injury19). It was estimated that the thermal increase was resulted from inflammation, local vasodilation and the secretion of chemical messengers [substance P, calcitonin gene-related peptide, nitric oxide (NO)] from nerve endings in response to painful stimuli3).
Inflammatory sites are always shown as a hot spot. Acute inflammation facilitates the secretion of substance P from nerve endings and increases vasodilation and vascular permeability escalating the effects of nerupeptides such as bradykinin and histamine. This inflammation-induced activation aggravates the inflammation itself and pain. In addition, local perfusion is increased by NO produced by nerve stimulus or humoral factors and regulatory chemical messengers, resulting in an increase of skin surface temperature2). This means that the degree of high temperature indicating the acute inflammation reflects the intensity of the vicious cycle of pain. Therefore, during this period, anti-inflammatory agents and steroids will be effective to manage the symptoms and local anesthetics or radiofrequency nerve block can be administered to stop the vicious cycle of pain13,18,21).
Generally, mild and moderate whiplash injury improves after 2 week conservative management with cervical brace, which alleviates the symptoms and helps the recovery, and the administration of anti-inflammatory agents and analgesics6). The prognosis has been inconsistently reported. Some reported that patients were completely recovered whereas others reported that the symptoms continued for several years. Compensation neurosis may be accompanied and some even files for a lawsuit23). In this case, visualization of changes in skin surface temperature at painful areas using thermography will help provide the evidence of suffering and any improvement as well as establish treatment plans.
Likewise there were no abnormalities in diagnostic imaging studies in our study. Once diagnosed with whiplash injury, the subjects were treated with absolute rest, anti-inflammatory agents and steroids. After 2 weeks, the symptoms were improved in most of the patients. To objectify subjective symptoms and any improvements, thermography was used. On thermography, skin surface temperature was becoming lower to the normal and symmetric imaging was created. We established treatment plans and follow-up based on the thermography results.
However, there were some limitations in our study. The first limitation is possible selective bias secondary to limited selection of patients. The observation period was short because the subjects were selected from in-patients and the sample size was also not many because there were few patients with only whiplash injury, because this study was conducted in a university hospital where more complex patients are dealt with. In addition, patients with grade 1-2 whiplash injury (Quebec classification) were only included in this study. This selection criterion was determined because it is difficult to perform thermography and to communicate with patients if there are severe cervical injuries causing other organ damages. So, we took a long time to recruit patients.
The role of IR thermography is still limited as a diagnostic tool because it is doubtful that thermography is able to identify the entire characteristics of neurogenic dysfunction and disability. The significance of this study is that subjective pain (expressed in VAS score) was objectively quantified with thermography (the comparative analysis of thermal differences before and after the treatment) under the same condition for a certain period of time. In this study, bias from asymmetric distribution was eliminated because the average thermal differences of the anterior and posterior neck and the right and left shoulder were about 0.16-0.3℃ which did not exceed 0.5℃16,25,26). Furthermore, the thermal differences measured after 2 week treatment were very close to the normal skin surface temperature (ΔT<0.3℃)26). Therefore, it was judged that thermography was performed according to the standard guidelines. The changes (ΔdT) of thermal differences greater than 0.5℃ in this study were also found to be significant. Thus, comparing thermal differences using thermography will aid the understanding and evaluation of pain and undefined painful condition and it can be used in the case of a lawsuit. It is also expected that combined use with VAS will also assist the evaluation and quantification of treatment.
CONCLUSION
The skin temperature of sites with immediate whiplash injury is hyperthermia and gradually decreased after two weeks, it got close to normal temperature. These are highly correlated with reduced VAS. Symptoms of whiplash injury are highly varied and some of them are not yet pathophysiologically explained. Although it seems that IR thermography is non-specific and has limited benefits, it can be used as a useful evaluation tool in undefined painful disorders such as whiplash injury because it is able to show objective data about pain experience and improvement.