INTRODUCTION
Various histological types of tumors arise in the pineal region. The most common tumors are pineal parenchymal tumors and germ cell tumors. Primary malignant melanoma is very rare in central nervous system and only 3.6% of these tumors arise in the pineal region12). To our knowledge, only 17 cases of pineal malignant melanomas have been reported since 189914).
Generally, malignant melanomas are known as radio-resistant tumor and the role of many treatment modalities are controversial. Here we report a rare case of primary pineal malignant melanoma with favorable outcome, which was totally removed by surgery and followed by radiotherapy.
CASE REPORT
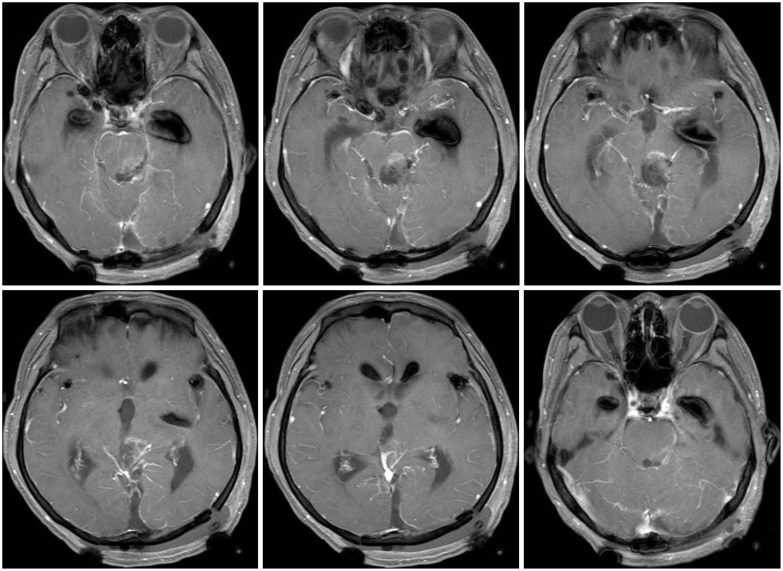
A 59-year-old male patient had 5-month history of gait disturbance and memory impairment. His initial brain computed tomography (CT) scan (Fig. 1) showed 3.5├Ś2.8 cm sized mass with very high density in the pineal region. This lobulated contoured mass showed dense hypointense rim on T2 weighted images (Fig. 2), and hyperintense on T1 weighted images of magnetic resonance imaging (MRI) scans. It contained heterogenous enhancement of central portion. Minimal ventricular dilatation was also suspected. There was no other intracranial lesion identified. On the basis of neuroimaging findings, the initial preoperative differential diagnosis included densely calcified pineal mass such as teratoma, less likely germinoma, and meningioma with dense calcification. Before surgery, he was taken for additional magnetic resonance spectroscopy (MRS) and perfusion MRI. Choline/Creatinine ratio was not elevated in MRS and regional cerebral blood volume was also not elevated in perfusion MRI.
In the operation room, we firstly performed endoscopic third ventriculostomy in the supine position. After tuber cinerium was punctured, the endoscope was removed and extraventricular drainage catheter was placed in the right lateral ventricle. And then we used left occipital transtentorial approach with the patient in the three-quarter prone position. An operated side (left)-down approach was used to minimize occipital lobe retraction. The paramedian linear skin incision was made. Under navigation guide, we performed craniotomy to expose the superior sagittal sinus and transverse sinus with pneumatic saw. The dura was opened with C-shaped flap based on superior sagittal sinus. When the dura was reflected, straight sinus and tentorium were visualized. After opening the tentorium, the quadrigeminal cistern was opened. Basal vein of Rosenthal and black solid tumor was found in the pineal region (Fig. 3). The tumor was adhered to midbrain, meticulous dissection under microscope was done and the mass was removed totally. After 24 hours postoperatively, the patient was taken for MRI, and there was no evidence of remnant tumor nor ventriculomegaly (Fig. 4). His preoperative symptoms were disappeared, and no other specific neurological deficits were founded.
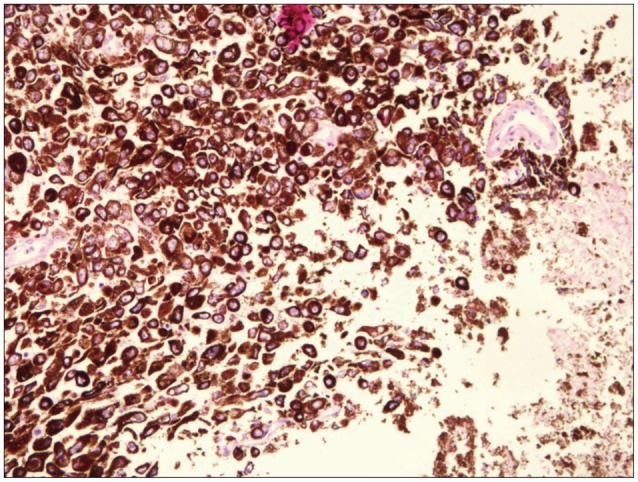
Hematoxylin and eosin (HE) staining showed anaplastic spindle-shaped and epithelioid cells with prominent nucleoli and large amounts of melanin pigmentations (Fig. 5). The tumor cells were immunohistochemically positive for HMB45, Melan-A, and S-100 protein. The Ki-67 index was 1%. Histopathological examination confirmed the diagnosis of malignant melanoma.
To differentiate whether this intracranial lesion is primary or metastatic, whole spine magnetic resonance images and whole body 18-fluoro-deoxyglucose positron emission tomography was done. But both studies could not demonstrate the primary site of this melanoma. It showed no relevant lesion. We also did scrupulous physical examination of his skin and mucosa, and dark pigmented lesion on his left leg was found, but additional studies including magnetic resonance images and skin biopsy showed negative finding. This lesion was due to the scratch wound made by bicycle chain 50 years ago. As a result, final diagnosis of primary pineal malignant melanoma was made.
After wound care, to choose adjuvant therapy, we referred to the most recent case report, which Shinsato et al.14) proposed for the treatment of primary malignant melanoma in the pineal region. We treated with 36 Gy of whole brain radiotherapy and 18 Gy of extended local boost irradiation without chemotherapy. The most recent follow-up image studies showed no recurrence or distant metastasis, which was acquired 26 weeks after surgery. And his Karnofsky Performance Scale score was 90.
DISCUSSION
Pineal gland tumors in adults account for about 0.4% to 1% of all intracranial tumors. And these pineal tumors are grouped into four main categories : 1) Germ cell tumors, 2) pineal parenchymal cell tumors, 3) glial cell tumors, and 4) other miscellaneous tumors and cysts4). The miscellaneous category includes such entities as meningioma, hemangioblastoma, choroid plexus papilloma, metastatic tumor, adenocarcinoma, and lymphoma. Usually, melanomas are included in the category of metastatic tumor.
Malignant melanoma, which represents only 4% of all cancers, has the highest propensity of all systemic malignant tumors to metastasize to the brain9). The incidence of brain metastases among patients with malignant melanoma varies from 6% to 43% in clinical series9) and from 12% to 90% in autopsy series. In clinical series, based on patients in whom the precise location of a single or a predominant metastasis could be determined, the metastases are distributed as follows : frontal lobes (36.1%), parietal lobes (26.4%), temporal lobes (18.9%), occipital lobes (10.6%), cerebellum (7%), and brainstem (0.9%)13). Based on our knowledge, metastatic melanomas in the pineal region are rare.
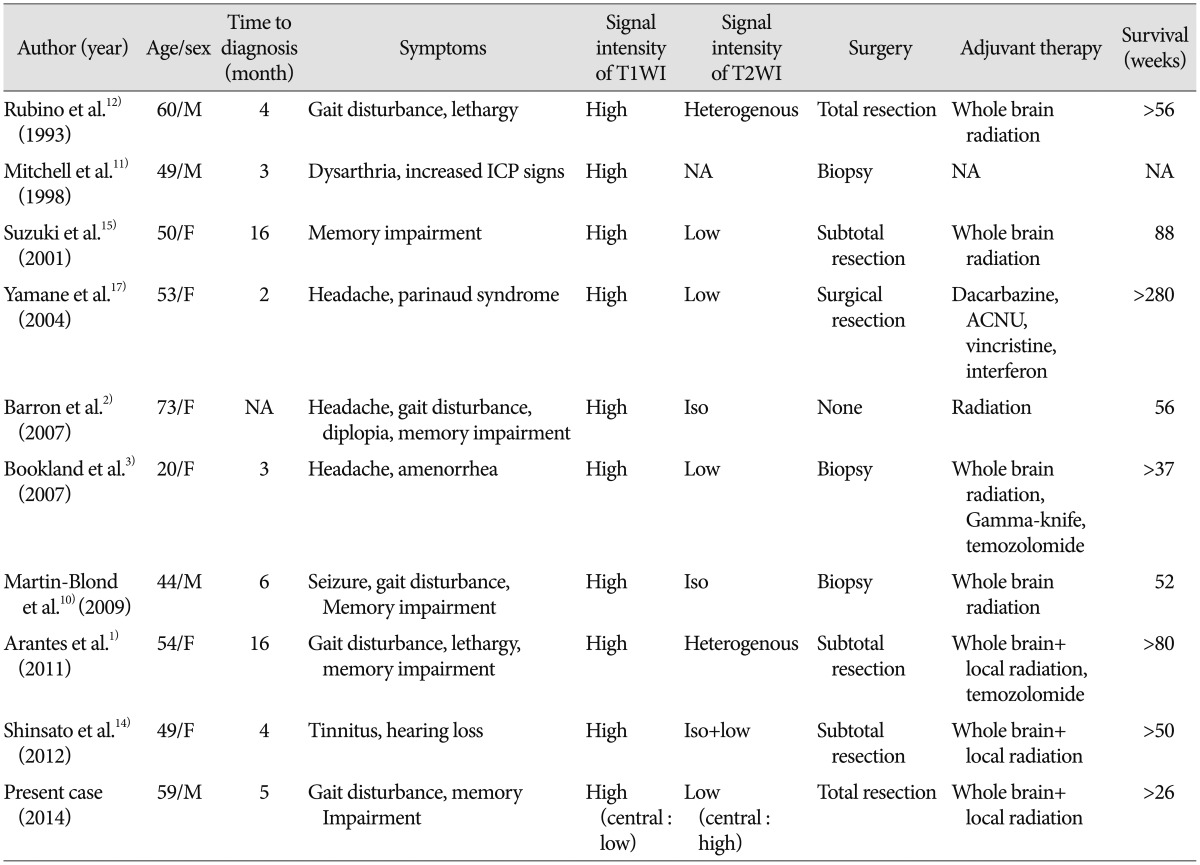
Moreover, primary melanomas of the central nervous system are scarcely found and furthermore, only about 3.6% of these tumors arise in the pineal region12). Only 17 cases have been reported to date and out of these, only nine cases were detected by MRI (Table 1)14).
Primary intracranial melanomas are thought to be developed from melanocytes, predominantly from the leptomeningeal melanocytes, that originated at the neural crest and migrated during embryogenesis16). These cells are found underneath the brain and the brainstem, inside the ventricles, at the optic chiasm, in the grooves of the various lobes, in the substantia nigra, and in the choroid16). And most reported lesions of primary melanomas were found in the spinal canal or the posterior fossa because of the higher concentration of leptomeningeal melanocytes at the anterior and lateral surface of the spinal cord and ventrolateral to the medulla oblongata14).
Intracranial malignant melanoma has a specific appearance on CT and MRI. On CT, the lesions show homogenously high dense mass. On MRI, approximately half of melanoma metastases are hyperintense on T1-weighted images before the administration of gadolinium whereas other cerebral metastases rarely demonstrate T1 hyperintensity5). Potential explanations for this intrinsic T1 hyperintensity include the presence of blood products and melanin8). And the shorter T1 relaxation time, which means higher signal intensity on T1-weighted images, correlates with the amount of melanin in the tumor1). Gaviani et al.6) proposed that no correlation was found between melanin content and T2 weighted signal intensity loss. In our case, the rim portion of the mass, which is hyperintense on T1-weighted images and hypointense on T2-weighted image, seemed to be the melanoma. And the central portion, with showed opposite signal intensity to the rim portion, seemed to be the tumor bleeding. These image findings, especially hyperintense signal on T1 weighted images, can help us to differentiate melanoma from other pineal gland tumors (Table 1).
It is difficult to distinguish primary intracranial melanoma from metastatic melanoma on neuroimages alone. Hayward proposed the following factors for establishing a diagnosis of a primary melanoma7) : 1) no malignant melanoma outside the CNS, 2) leptomeningeal involvement, 3) intramedullary spinal lesions, 4) hydrocephalus, 5) tumor location in the pituitary or pineal gland, and 6) a single intracerebral lesion. Despite aggressive multimodality treatment, the reported median survival of patients with metastatic melanoma is only 3-6 months, which is much shorter than the patients with primary melanoma. Therefore, it is necessary to distinguish between primary and metastatic melanomas.
At present, there is no optimal treatment of intracranial melanoma. Most authors agree that complete surgical resection is essential. And whether we should add radiotherapy or chemotherapy as an adjuvant therapy is controversial. However, recent case reports show that radiotherapy should be performed as mandatory, and chemotherapy as optional for primary malignant melanoma1,2,3,12). Barron et al.2) reported a patient with primary pineal gland melanoma who survived for 56 weeks after receiving only radiotherapy. And Shinsato et al.12) report a rare case of primary melanoma of the pineal gland with prolonged survival of more than 56 weeks after subtotal tumor resection followed by whole-brain and extended local irradiation without chemotherapy. The present case underwent complete surgical removal without complication and received 36 Gy of whole brain radiotherapy and 18 Gy of extended local boost irradiation without chemotherapy. And the patient had no recurrence until 26 weeks after surgery. So far, this treatment seems to be efficient for this patient (Table 1). Although there are only few cases to prove the outcome of each treatment, we suggest that surgery followed by radiation without chemotherapy can be sufficient and be recognized as the optimal treatment for primary malignant melanoma in the pineal region.
CONCLUSION
We report a rare case of primary malignant melanoma in the pineal region, who underwent complete surgical resection and adjuvant radiotherapy without chemotherapy. A long-term follow-up was needed to determine whether radiotherapy without chemotherapy is sufficient for the treatment of primary pineal malignant melanomas. Although there is only limited results about each treatment, we suggest that surgery followed by radiation without chemotherapy can be sufficient and be recognized as the optimal treatment for primary malignant melanoma in the pineal region.