INTRODUCTION
Hiccup is a repeated involuntary, spasmodic, and temporary contraction of the diaphragm accompanied by a sudden closure of the glottis, producing the characteristic inspiratory sound "hic" and discomfort9). It can be considered persistent or intractable when it lasts more than 24 hours11). The exact etiology of hiccup remains unclear in most cases. Regarding various central causes, the medulla oblongata has been investigated as one of the most important centers in the hiccup circuit. In addition to neurological disorders, including medullary infarction and hemorrhage, tumors and tuberculoma reportedly generate intractable hiccup2,7,17).
Although few reports demonstrated surgically treated and pathologically confirmed cavernous hemangioma (CH) in the medulla oblongata4,11,12,15,18), most of them were superficially located in the dorsal part of the medulla oblongata. In the current case, the authors demonstrate the fully embedded medullary cavernoma with intractable hiccup surgically treated without morbidity and discuss possible pathogenesis of this condition with a review of the reported cases and related literature.
CASE REPORT
History
A 28-year-old man presenting with persistent hiccup for 15 days was admitted to our hospital. The symptom developed suddenly and aggravated progressively in its frequency and intensity. The patient noticed motor weakness and sensory changes in the left side of his body three days prior to admission. Hiccup did not respond to any types of medication, but occurred only occasionally while asleep. There were no abnormal findings in endoscopy and computed tomography scans for the chest and abdominal organs.
Presentation and examination
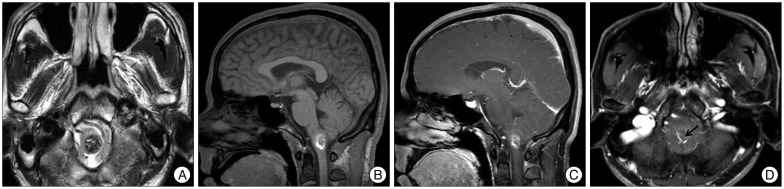
On admission, neurological examination revealed no impairment of mental status, definitive sensory or motor deficits, gaits difficulties, or abnormal deep tendon reflex. The cranial nerves were also unaffected. Magnetic resonance (MR) imaging showed a 1.5×1.5×2 cm nodule in the left medulla oblongata with peripheral hyperintensity on T1-weighted images and predominantly low signal intensity on T2-weighted images (Fig. 1). The lesion was not enhanced by administration of gadolinium. Vertebral angiography demonstrated no staining of the lesion.
Operation and postoperative course
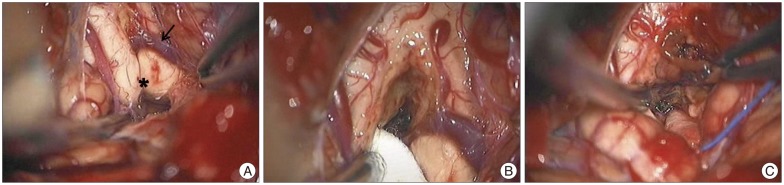
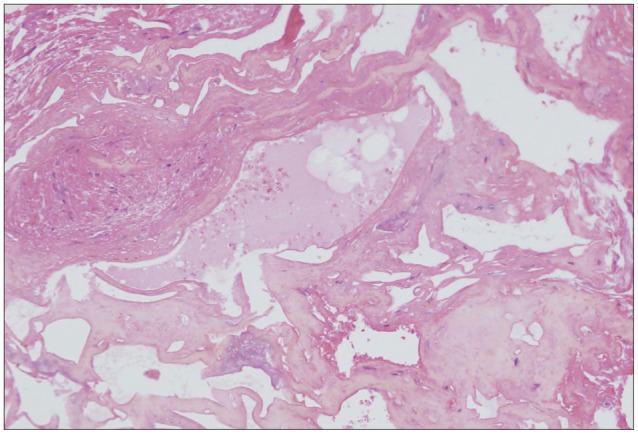
On presumptive diagnosis of cavernous hemangioma in the medulla oblongata, surgery was performed via the midline suboccipital approach under prone position. The lesion was covered by normal parenchymal tissue and made a bulging contour of the medulla oblongata with superficial abnormal draining veins (Fig. 2A). The shortest trajectory to the lesion was confirmed by neuronavigation (StealthStation S7®, Medtronic, Minneapolis, MN, USA) and a 2 cm longitudinal pial incision was made caudally from the obex. After dissecting a few millimeters deep, hemosiderin staining of the neural tissue was encountered (Fig. 2B). The plane of the dissection between the cavernoma and the parenchyma was well-distinguished (Fig. 2C). The lesion was removed en bloc. Histopathologically, the brain specimen revealed irregularly dilated vascular spaces without intervening neural tissue, which are typical features of cavernous hemangioma (Fig. 3). Additionally, there was reactive piloid gliosis with numerous Rosenthal fibers in the periphery of the lesion and occasional hemosiderin-laden macrophages. Hiccup resolved immediately after surgery. The patient had slight hemiparesis (motor grade IV+/IV+) and hemisensory changes that cleared entirely at the time of discharge.
DISCUSSION
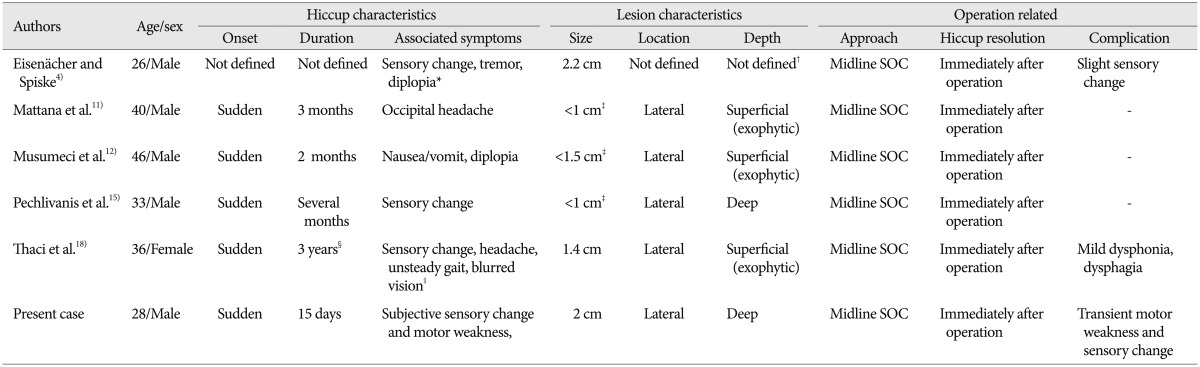
The clinical manifestations of the brainstem CHs closely correlated with the anatomical location of the lesion. The common signs and symptoms include various types of cranial neuropathy, sensory/motor deficits, headache, diplopia, ataxia, vertigo, nausea/vomiting, dysarthria, dysphagia, and dysmetria, but hiccup has rarely been reported1). Porter et al.16), in their review of 100 cases of brainstem cavernous malformations, reported hiccup as the presenting symptom in three cases. Contrary to this, Ward et al.20) reported that intractable hiccup was not infrequent clinical presentation in medullary cavernoma (5/18 cases, 27.8%). However, these case series did not reveal the detail description on the exact location, and clinico-radiological characteristics. For this reason, medullary caverrnoma presenting as intractable hiccup has been reported as a single case report, with the explanation of unique clinical course (Table 1)4,11,12,15,18). Majority of reported cases were in male patients (female in only one case) with the mean age of 34.8 years, relatively younger than the patients with general brainstem CHs in a large series (41.8 years in brainstem CHs; 44.1 years in medullary CH)1). Main accompanying symptoms were sensory/motor deficits, followed by visual disturbance, headache or nausea and vomiting. Intralesional hemorrhage, related with sudden onset natures of hiccup, occurred in all cases and the size of the lesion was varied (range from smaller than 1 cm up to 2.2 cm). Medullary CHs tend to be the smallest among brainstem CHs (mean diameter, 1.2 cm in medullary CHs vs. 1.8 cm in total brainstem CHs), while the preoperative hemorrhagic rate approaches 97% in the medullary CHs and in brainstem CHs as well1). The hiccup was immediately resolved after the surgical resection in all cases.
With regard to the pathomechanism of hiccup, Hassler assumed that hiccup could be the subcortical equivalent of myoclonus generated at the pontomedullary level of the triangle of Guillan-Mollaret (inferior olivary nucleus, dentate nucleus, and red nucleus)5). Other investigators proposed that hiccup could be resultant from denervation supersensitivity caused by dysfunction of the inferior olivary complex, nucleus ambiggus and adjacent reticular formation of medullar oblongata8,10,19). In animal studies, hiccup-like responses were generated by electrical stimulation in the medullary reticular formation, lateral to the nucleus ambiggus and rostral to the obex3). Oshima et al.13) also showed that GABA-containing inhibitory cells in the nucleus raphe magnus could be the source of inhibitory inputs to the hiccup reflex arc.
Medullary lesions other than medullary CHs also reportedly induced hiccups in the dorsolateral aspect of the medullar oblongata6,7,21). In a study conducted by Park et al.14), 14% of patients with lateral medullary infarcts (seven out of 51) had hiccups, mainly when the lesion developed in the dorsolateral region of the middle medulla. All reported cases of medullary CHs, inducing intractable hiccup (except one case with ill-defined location), demonstrated laterally-located lesions in the medulla oblongata; three were superficial exophytic cavernomas and the other two, totally buried into medulla. In addition, the intractable hiccup in the reports resolved immediately after surgery. The location of the former three exophytic cases seems to be in the dorsolateral medulla rostral to the obex, described by Arita et al.3), in which the pathophysiology may be related to excitatory function for hiccup genesis. On the other hand, the latter two cases, including the current one, were located in the deep portion of the dorsolateral medulla caudal to the obex. Intractable hiccup in the latter ones may be induced by inactivation of the inhibitory function of GABA-containg neurons suggested by Oshima et al.13) Considering the aforementioned hiccup pathogenesis and the case summary, we presume that the present medullary cavernoma may also have reduced the inhibitory function or induced a stimulatory signal on the hiccup reflex by displacing or compressing the hiccup arc of the dorsolateral medulla.