INTRODUCTION
It has been frequently described that acute stroke is associated with increased incidence of arrhythmias1,9,10,19). One of the most common arrhythmia following stroke is atrial fibrillation23). Although the pathogenesis of these arrhythmias is still obscure, they are obviously associated with impairment of cardiac autonomic balance between the sympathetic8,9,11,15) and the parasympathetic9,10,15) nervous system13).
Arrhythmia immediately after stroke has been reported in patients with both hemispheric9,10) and brainstem cerebral infarcts8). Most post-stroke arrhythmias appear in patients with right-sided hemispheric infarcts12,15,22), especially in patients with right insular infarcts2,3,14,17,22). However, conversion of arrhythmia to normal sinus rhythm following acute cerebral infarct has not been reported. We present here a patient who had spontaneous conversion of atrial fibrillation to normal sinus rhythm after recurrent cerebral infarcts.
CASE REPORT
A 88-year-old men was brought to emergency room with right hemiparesis and aphasia. Six years ago, he was admitted to hospital due to transient ischemic attack and diagnosed of atrial fibrillation, hypertension, hyperlipidemia, gout and chronic renal insufficiency. At that time, brain MRI showed old basal ganglia lacunar infarct without any abnormality in intracranial and extracranial vascular structures. Thereafter, he had regularly visited outpatient clinic of internal medicine with medication including antiplatelet agent. He had not been administered any medication for permanent atrial fibrillation which was continued at regular check-up.
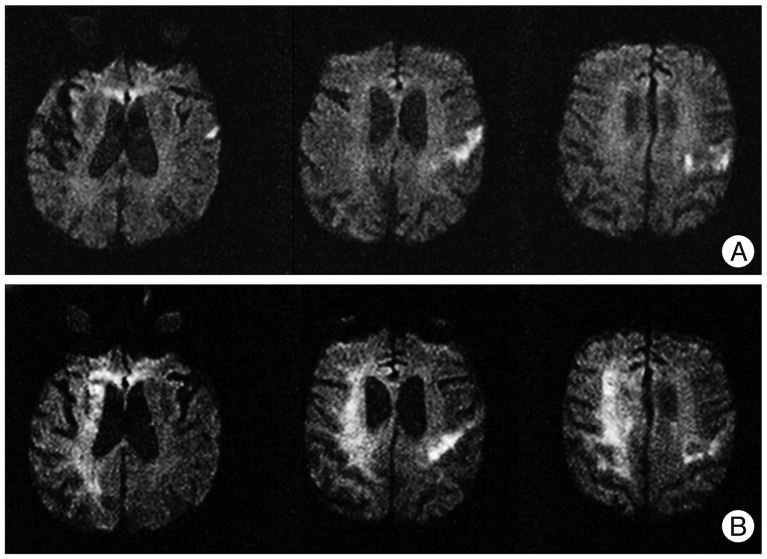
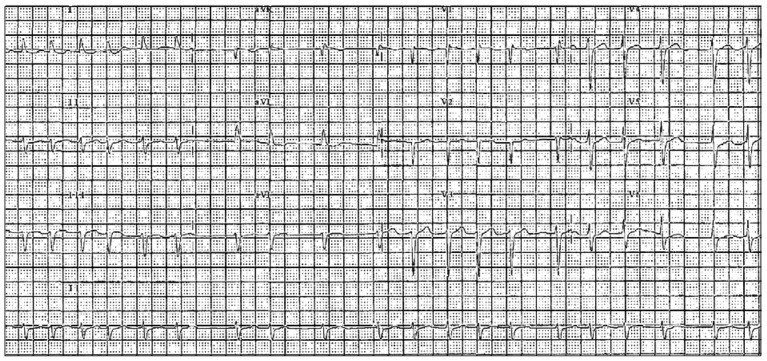
On admission, he was mild drowsy and not communicated. Neurological examinations showed right hemiparesis of grade IV (Medical Research Council grade) and aphasia. Gaze deviation or visual field defect was not detected. Diffusion-weighted MRI showed multiple small cortical infarcts in left middle cerebral artery territory without involvement of insular cortex (Fig. 1A). Electrocardiogram (12 leads) revealed atrial fibrillation with rapid ventricular rhythm (Fig. 2). Echocardiogram revealed moderate aortic valve regurgitation and left atrial enlargement with diameter of 44.7 mm (Aorta, 28.1 mm) on M-mode study. However, ejection fraction was normal and thrombus was not observed in the atrium or ventricle. We started treatment with heparin and digoxin for atrial fibrillation with rapid ventricular rhythm, but did not use antiarrhythmic agent. After few days, digoxin was stopped due to decrement of heart rate less than 40/min. Seven days after admission, anticoagulation was stopped because of gross hematuria. Eighteen days after admission, intubation was performed due to purulent sputum and severe stridor induced by epiglottitis. His right-sided weakness progressed to hemiplegia of grade III, but other neurologic symptoms did not deteriorate.
Approximate 1 month after admission, his consciousness was suddenly decreased to stuporous state. On neurologic examination, eyeball was deviated to right side, and left side hemiparesis of grade I was newly developed. Emergent diffusion-weighted MRI revealed that right-sided diffuse subcortical infarcts of middle cerebral artery territory (Fig. 1B). However, insular cortex was not directly involved. Immediately after second ischemic attack, his atrial fibrillation converted spontaneously to normal sinus rhythm which detected by intensive care unit monitoring and ECG follow-up (Fig. 3). Cardiac enzymes were normal and follow-up echocardiogram was not different to previous exam. Normal sinus rhythm was sustained until he died due to sepsis on 11 days after second attack.
DISCUSSION
Although there have been many reports about acute onset arrhythmias following stroke, spontaneous conversion of arrhythmia to normal sinus rhythm after stroke has not been described. Post-stroke arrhythmia has been reported to develop a few hours to 3 days after stroke and then spontaneously reversed to normal sinus rhythm after a few days to possibly even a few months16,19,23). Cerebrogenic mechanism of post-stroke arrhythmias was suggested by the temporal relation between stroke and arrhythmia. In our case, conversion of atrial fibrillation to normal sinus rhythm immediately following second stroke attacks may also support the theory of "cerebral arrhythmogenesis". However, it is obscure whether this conversion to normal sinus rhythm was prolonged effect because our patient died during acute period of second stroke attack.
Several experimental or clinical evidences that acute stroke deranges cardiovascular autonomic regulatory system and results in electrocardiographic changes or arrhythmias have been reported1,19). This finding was shown in patients with subarachnoid hemorrhage, subdural hematoma, brainstem hemorrhages and infarcts, and both hemispheric hemorrhages and infarcts irrespective of cortical or subcortical areas1,7,22). Many investigations for cortical lateralization indicated that the right-side hemispheric stroke was more arrhythmogenic than left-side lesion4,11,14,23,24). In particular, right-side insular cortex was suggested as cardiovascular regulation center in brain through few case reports with cerebral infarctions2,3,14,17,20). However, post-stroke arrhythmias were found more commonly in patients with subarachnoid hemorrhage or intracranial hematoma without notion of any specific localization or vascular territory5,8,23). Our case showed bilateral hemispheric infarctions within the middle cerebral artery territories. After right hemispheric infarction, his atrial fibrillation was converted spontaneously to normal sinus rhythm. This finding supports the hypothesis that cardiovascular regulation center in the brain is more lateralized to right hemisphere. A possible mechanism of cardioversion in our patient can be suggested by previous reports. Increased QT interval, which means the prolongation of action potential, is the main mechanism for arrhythmia conversion of class IA anti-arrhythmic agent such as quinidine, procainamide. The prolongation of QT interval following right hemispheric infarction has reported by previous studies6,20). Although exact mechanism of conversion to normal sinus rhythm is not clearly understood, the possible prolongation of QT interval after the second stroke in right hemisphere may contribute to the spontaneous cardioversion in our case.
CONCLUSION
Our case may suggests possibility that physicians could miss the risk factor due to immediate conversion of arrhythmia to normal sinus rhythm after cerebral infarcts on admission. If no risk factor was revealed by intensive investigation, physicians should concern arrhythmia as a possible etiology of stroke even if the patient has normal sinus rhythm.