INTRODUCTION
Isolated abducens nerve palsies caused by vertebra artery (VA) aneurysm have been rarely reported1-3,7). Nerve compression due to aneurysm, cisternal hematoma, vascular insufficiency, increased intracranial pressure (ICP) have been suggested as potential mechanisms for isolated abducens nerve paralysis following ruptured VA aneurysm. The patients usually presented with bilateral or ipsilateral gaze palsy to the pathologic lesions.
To the best of our knowledge, we describe the first case of dissecting VA aneurysm presenting with contralateral abducens nerve palsy and discuss its possible mechanisms.
CASE REPORT
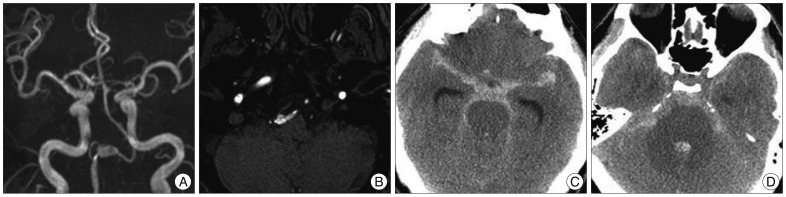
A 38-year-old man was admitted for management and evaluation of a headache that had persisted 6 days. The headache had initially developed after completing a marathon. The patient had visited the visited emergency department in our institution 3 days later. Neurologic and laboratory examinations at that time revealed no abnormalities. Computed tomography (CT) scan revealed no evidence of hemorrhage. The patient was discharged receiving analgesic and further radiologic tests were recommended. On the present admission, the patient was alert and displayed no signs suggesting neurologic deficits. Time of flight magnetic resonance angiography (Fig. 1A) and axial magnetic resonance angiography source image (Fig. 1B) disclosed a fusiform dilatation of the right vertebral artery involving the proximal portion of the posterior inferior cerebellar artery (PICA). The patient suddenly suffered from severe headache with diplopia a day before the scheduled cerebral angiography. Neurologic tests revealed nuchal rigidity and impairment of conjugate left lateral gaze. Emergent intracranial CT demonstrated a high density area in the basal cistern and prepontine cistern without ventriculomegaly (Fig. 1C, D).
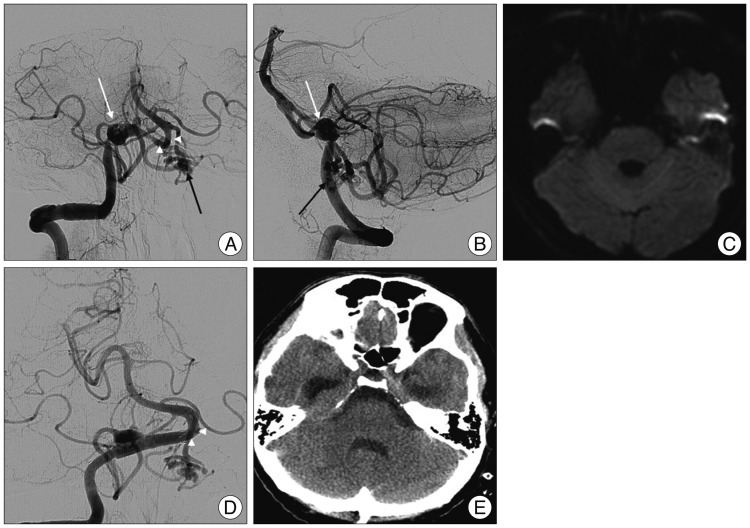
Right vertebral angiography (Fig. 2A, B) revealed a dissecting aneurysm of right distal vertebral artery compromising proximal PICA with blood supplying to the left proximal portion of PICA through glomus-like vascular channel from right VA. In particular, the vertebrobasilar artery was remarkable flexed to the inferior on the left side. A double-stent method was performed for ruptured dissecting vertebral artery aneurysm. No diffusion restriction was found in follow-up magnetic resonance imaging (MRI) of the brain stem (Fig. 2C). Four weeks later, another angiography (Fig. 2D) illustrated the upward displacement of the vertebrobasilar artery compared with previous images and a CT scan (Fig. 2E) showed hemorrhage resolution in the prepontine cistern. Full recovery of left abducens nerve paresis was achieved in 11 weeks after onset (Fig. 3B).
DISCUSSION
The incidence of isolated abducens nerve palsy following VA aneurysm is rare. To our knowledge, only three cases of VA aneurysm (two ruptured and one unruptured) presenting with unilateral sixth nerve paralysis have been reported1-3).
The possible mechanisms of the isolated nerve palsies related to aneurysm of VA can be divided into several groups : direct compression by aneurysm1,2), brain stem or nerve compression due to thick cisternal hematoma, especially prepontine cistern7), stretch nerve injury on the petrous apex triggered by increased ICP6), and vascular insufficiency to the abducens nuclei by vasospasm9).
The chance of the direct nerve contact with aneurysm could be ruled out in our patient because the patient suffered left sixth nerve palsy after ruptured right dissecting VA aneurysm. Coppeto and Chan1) and Dumas and Shults2) showed ipsilateral sixth nerve palsy to the same direction of VA aneurysm.
Thick prepontine cisternal hemorrhage was found in an intracranial CT scan, but the possibility of nerve paresis was thought to be low, considering the prepontine segment of the abducens nerve, because direct compression by cisternal hematoma causes only bilateral abducens nerve palsy. Morioka et al.7) illustrated two cases of bilateral isolated sixth nerve palsy compressed by cisternal hematoma.
Regarding the increased ICP, no prominent brain swelling or acute hydrocephalus was seen on brain CT. Follow-up MR imaging demonstrated no diffusion restriction on brain stem. Thus, vasospasm could be excluded as a candidate etiology. In addition, the neurologic deficit sings associated with facial nuclei or medial longitudinal fasciculus were not noted9).
Therefore, for this patient, a thick blood clot in the prepontine cistern (Fig. 1D) may attribute to marked displacement of vertebrobasilar artery (Fig. 2A) and may lead to compression of the abducens nerve on the opposite side.
A similar mechanism has been suggested as a cause of isolated sixth nerve palsy on the contralateral side. Elongation of vertebra artery8) and prominent flexion of basilar artery related to aneurysm of superior cerebellar artery5) can lead to isolated sixth nerve palsy on the contralateral side by compression of the vertebral artery of the opposite side.
Every VA aneurysm presenting with isolated sixth nerve palsy was treated by clip placement. Opening of Liliequist's membrane and cisternal irrigation of hematoma may seem to be effective for clinical improvement4). Complete recovery of nerve palsy was observed in three cases (two bilateral and one unilateral)3,7).
In this case, endovascular flow diversion by double-stent method was performed. Full recovery resulted by 11 weeks after onset. Although, MRI with spoiled gradient recalled echo images was not obtained for the confirmation of direct abducens nerve contact with vertebral artery due to the limited time, the follow-up MRI may support the mechanism of nerve compression by shifted vertebrobasilar artery.