INTRODUCTION
Endovascular treatment (EVT) has been widely performed for acute ischemic stroke with better outcome than medical treatment [9]. According to patient data from five randomized trials (MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, and EXTENDED IA) [9], EVT can significantly reduce disability at 90 days compared to medical treatment (adjusted common odd ratio [cOR], 2.49; p<0.001). Nevertheless, usefulness of EVT for acute M2 segment of middle cerebral artery (MCA) occlusion remains unclear because most results are obtained from patients with large artery occlusion in the anterior circulation [3]. Goyal et al. [9] have reported that EVT has no favorable effect for M2 occlusion than medical treatment (cOR, 1.28; 95% confidence interval [CI], 0.51-3.21). Compared to M1 segment of MCA, M2 shows smaller caliber size with thinner wall [24]. Although vascular territories affected by acute ischemia of M2 occlusion are smaller than M1 occlusion, M2 occlusion can also lead to massive strokes that cause death or moderate to severe disability in approximately 50% of patients [28].
Due to advances in endovascular technologies, treatment outcomes of mechanical thrombectomy for acute M2 occlusion have been increasingly reported. Nevertheless, systematic review or meta-analysis of EVT outcomes, in particular technical aspects of successful recanalization and procedure-related complications, has not been well studied. Therefore, the aim of this study was to examine procedural outcomes of EVT for isolated M2 occlusion. In addition, procedural outcomes according to thrombus location were compared between M2 and M1 occlusion.
MATERIALS AND METHODS
Literature search
Literature searching through PubMed, Embase, and the Cochrane Central were searched using the following key words: ŌĆ£ischemic strokeŌĆØ, ŌĆ£endovascular therapyŌĆØ, ŌĆ£cerebral infarctŌĆØ, ŌĆ£intra-venousŌĆØ, ŌĆ£intra-arterialŌĆØ, ŌĆ£fibrinolysisŌĆØ [6], ŌĆ£thrombolysisŌĆØ, ŌĆ£thrombectomyŌĆØ, ŌĆ£MCAŌĆØ, ŌĆ£M1ŌĆØ, ŌĆ£M2ŌĆØ, ŌĆ£hemorrhageŌĆØ, ŌĆ£embolusŌĆØ, ŌĆ£deathŌĆØ, ŌĆ£peri-operative complicationsŌĆØ, and ŌĆ£mortalityŌĆØ.
Selection criteria and data abstraction
Our inclusion criteria were : 1) studies that included patients presenting with acute M2 occlusion; 2) participants over 18 years; 3) endovascular treatments such as intra-arterial thrombolysis using tissue plasminogen activator (tPA) or urokinase and mechanical thrombectomy with stent retrieval, Merci retriever, or suction devices; 4) studies that included a minimum of 10 endovascular procedures through the common femoral artery [15,16]; 5) clinical information on angiographic recanalization, clinical outcome, mortality, and complications can be extracted; and 6) randomized controlled studies, prospective or retrospective case-controlled studies with quality score over 5 on the Newcastle-Ottawa scale [20]. Exclusion criteria were : 1) patients who did not show acute ischemic stroke; 2) incomplete data or unclear distinction between acute M1 and M2 occlusion; and 3) review articles or case reports [10,13,14].
The primary outcome was successful recanalization rate and symptomatic intracranial hemorrhage (S-ICH) after the procedure. Secondary outcomes were good clinical outcome after 3 months and mortality. Subgroup analysis compared procedural outcomes such successful recanalization and SICH according to thrombus location (M1 and M2). Successful recanalization was defined as thrombolysis in cerebral ischemia (TICI) or modified TICI Ōēź2b or thrombolysis in Myocardial infarction grades 2 or 3 [1]. Good clinical outcome was defined when 3-month modified Rankin scale (mRS) score was Ōēż2. S-ICH was defined as any cerebral hemorrhage concomitant with an increase of at least 4 National Institutes of Health Stroke Scale (NIHSS) score within 24 hours or resulting in death [18]. An extensive electronic search was performed by an experienced researcher. Two authors (J.P.J. and C.H.K.) independently evaluated the eligibility of these studies and extracted data using a uniform and standardized form. Disagreements between the two authors were resolved by discussion and consultation with a third author. This meta-analysis was performed according to PRISMA guidelines [19].
Statistical analysis
Cumulative incidence (event rate) and 95% CI were estimated from each study. Dichotomous variables are presented as odds ratio (OR) with 95% CI. Heterogeneity was evaluated using I2 test. If I2 was less than 50%, a fixed effect model was used [23]. Publication bias was determined using EggerŌĆÖs test of the intercept, and Begg and Mazumdar [4] rank correlation test. Comprehensive meta-analysis (CMA) sof tware (CMA v2.2.064; Biostat, Englewood, NJ, USA) was used for all analysis. Statistical significance was accepted at p <0.05.
RESULTS
Identification of relevant studies
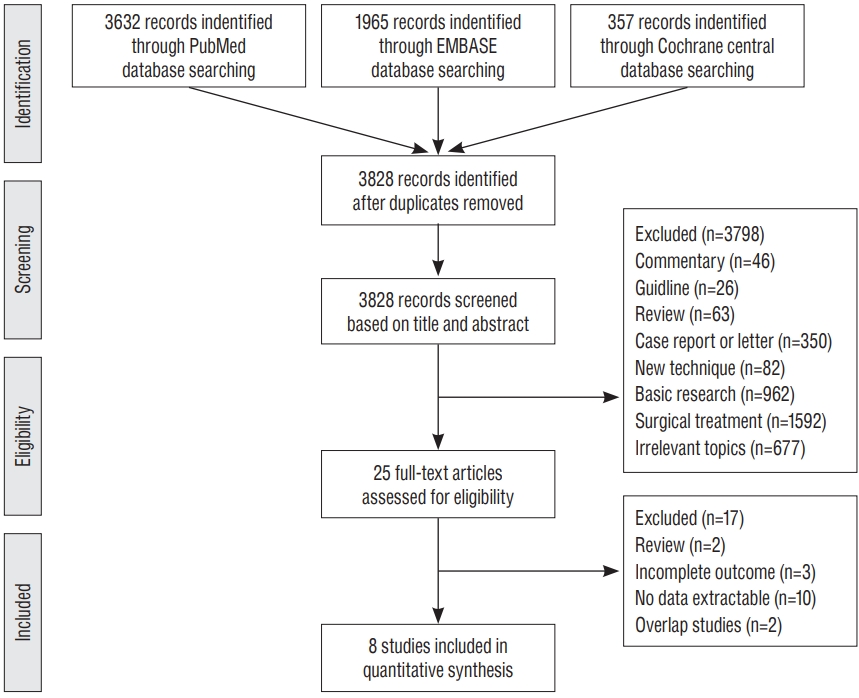
A flow diagram of the search process is detailed in Fig. 1. After screening records and deciding eligibility, eight articles were selected for analysis. Among them, three studies compared endovascular treatment outcomes between acute M1 and M2 occlusion. The mean age of patients used for each study ranged from 63.7 to 71 years. The median NIHSS score at admission ranged from 12 to 17. Detailed baseline characteristics are summarized in Table 1.
Procedural outcomes of acute M2 occlusion after EVT
A total of eight studies (650 patients) reported events of successful recanalization, S-ICH, good clinical outcome on 3-month follow-up and mortality. Of these, one article was excluded for mortality analysis because they did not provide such information. Successful recanalization rate at final angiogram was 69.1% (95% CI, 54.9-80.4%). The rate of S-ICH was 6.1% (95% CI, 4.5-8.3%; Fig. 2). Good clinical outcome rate at 3-month follow-up after EVT was 59.4% (95% CI, 49.9-68.2%). Mortality rate was 14.9% (95% CI, 11.4-19.3%).
Comparisons of EVT outcomes according to thrombus location (M1 vs. M2)
A total of 706 patients (M2 occlusion, n=159; M1 occlusion, n=547) from the three studies [2,8,29] reported procedural outcomes according to thrombus location (Table 2). The number of successful recanalization was 105 (66.0%) in M2 and 394 (72.0%) in M1 occlusion. Successful recanalization (OR, 1.539; 95% CI, 0.293-8.092; p =0.610) and S-ICH (OR, 1.313; 95% CI, 0.603-2.861; p =0.493) did not differ significantly between the two groups (Fig. 3). Good clinical outcome was more evident in M2 occlusion after EVT compared to that in M1 occlusion (OR, 1.639; 95% CI, 1.135-2.368; p =0.008). Mortality did not differ significantly according to thrombus location (OR, 0.788; 95% CI, 0.486-1.276; p =0.332).
Publication bias
In the publication bias analysis for comparing successful recanalization according to thrombus location (M1 vs. M2), EggerŌĆÖs regression test revealed that the intercept was 3.98 (95% CI, -21.56 to 29.53; t=1.98, df=1; two-tailed p =0.30). For rank correlation test, KendallŌĆÖs tau was 0.33 with two-tailed p value of 0.60. Regarding S-ICH according to thrombus location, EggerŌĆÖs regression test disclosed that the intercept was -1.13 (95% CI, -11.31 to 9.04; t=1.42, df=1; two-tailed p =0.40). For rank correlation test, KendallŌĆÖs tau was -0.33 with two-tailed p value of 0.60. Accordingly, there was no evidence of publication bias based on these comparisons.
DISCUSSION
Due to advances in endovascular technologies, mechanical thrombectomy has been increasingly conducted for distal arterial occlusion [12,31]. Kim et al. [17] have reported that direct aspiration has successful recanalization rate of 72.0% (vs. 87.5% in stent retriever group) and good functional outcome rate of 84.0% (75.0% in stent retriever group) at 3-month follow up. Park and Kwak [21] have reported successful recanalization rate of 84% (27 out of 32) and good functional outcome of 78% (25 out of 32) at 3-month follow-up using Penumbra 4 MAX catheter (Penumbra, Alameda, CA, USA) without any occurrence of S-ICH. Nevertheless, beneficial effect of EVT for M2 occlusion compared to medical treatment remains questionable. Recently, a multicenter retrospective analysis [25] has compared treatment outcome between EVT and medical management for patients with acute M2 occlusion. Good outcomes at 3 months were more evident in the EVT group (n=181, 62.8%) than that in the medical treatment group (n=83, 35.4%) (p =0.001). The rate of S-ICH did not differ significantly between the two groups (5.6% in EVT vs. 2.1% in medical management; p =0.10). Therefore, they suggested that EVT was more feasible for treating acute M2 occlusion than medical treatment.
Comparative studies of procedural outcomes according to thrombus location (M1 vs. M2) are important since it can provide indirect evidence of EVT for M2 occlusion. Sheth et al. [28] have found similar recanalization rate (44% vs. 46% in M1, p=0.31) and discharge mRS 4-6 rate (49% vs. 64% in M1; p=0.13). The rate of S-ICH was significantly lower in M2 occlusion (21%) than that in M1 occlusion (56%) after EVT. Coutinho et al. [7] have performed a post hoc analysis to examine M2 occlusion outcomes after stent retriever thrombectomy in three multicenter prospective series [22,26,27]. There was no significant differences in the rate of successful recanalization (85% vs. 82% in M1 occlusion; p =0.82), mortality (12% vs. 10% in M1 occlusion; p =0.62) and S-ICH (2% vs. 2% in M1 occlusion; p =1.00). M2 occlusion tended to be recanalized with lesser number of stent pass compared to M1 occlusion (mean, 1.4 vs. 1.7; p =0.07). On the contrary, Arnold et al. [2] have reported better recanalization rate (76.8%) in M1 occlusion than that (68%) in M2 occlusion (p<0.001). Such difference in the rate of mechanical thrombectomy (40.6% in M1 occlusion and 23.4% in M2 occlusion) might be due to better recanalization in M1 occlusion. Our meta-analysis revealed no significant difference in procedural outcomes such as successful recanalization and S-ICH after EVT according to thrombus location. Accordingly, M2 occlusion can be given the same consideration as M1 occlusion if EVT is suitable [28].
Differences in endovascular devices and proportion of mechanical thrombectomy could affect treatment results for M2 occlusion. Stent retrieval thrombectomy provided better recanalization and clinical outcomes than Merci retrieval system. Broussalis et al. [5] have reported that stent retrieval thrombectomy has successful recanalization rate of 82% and good outcome rate of 65% at 3 month follow up, which are higher than 62% and 35%, respectively, in the Merci retrieval system. Hentschel et al. [11], have also reported better recanalization rate of 97.01% and good clinical outcome rate of 61.67% at 3 months in patients treated with stent retriever thrombecvtomy (79.80%) compared to those treated with non-stent retrieval thrombectomy (22.54%). For M2 occlusion, solitaire stent yielded successful recanalization rate of 93.3%, good outcome of 60.0%, mortality of 6.7%, and S-ICH of 6.7% [8]. The Merci system has shown successful recanalization rate of 82.1%, good outcome rate of 39.3%, mortality of 25.0%, and S-ICH rate of 3.6% [29]. Rahme et al. [24] have reported a pooled analysis of treatment outcome in M2 occlusion from PROACT II, IMS, and IMS II trials. Successful early reperfusion was noted in 31 patients (49.2%). Good functional outcome rate was 58.1% in M2 occlusion with successful recanlaization. They found that patients with acute M2 occlusion did not show positive correlation between reperfusion status and clinical outcome at 3 months (p =0.80). However, the PROACT II study compared treatment outcomes between IA recombinant prourokinase with low-dose intravenous (IV) heparin and low-dose heparin excluding mechanical clot disruption. The IMS trial also determined the efficacy of combined IV and IA tPA for acute ischemic stroke. Sheth et al. [28] have reported a successful recanalization rate of 44.2% after EVT. In their study, IA tPA (n=33, 63.5%) was used the most frequently, followed by the Merci system (n=10, 19.2%). Accordingly, larger studies are needed in consideration of treatment strategies (thrombolysis using drug or devices; or stent retriever or direct aspiration) to determine the beneficial effect of EVT in acute M2 occlusion on clinical outcome.
This study has some limitations. First, most studies of this investigation were retrospective in nature. Second, several factors such as endovascular devices and prior use of IV tPA might have affected clinical outcomes. Third, definition of M2 occlusion can be different according to investigators. Accordingly, consensus about anatomical M2 definition is needed to analyze treatment outcome [30]. Fourths, difference in stroke severity at admission could be a confounding factor in interpreting these results, especially analyzing clinical outcome. This was because patients with M2 occlusions often present with few to moderate symptoms and may be therefore not considered for EVT. In this study, we aimed to assess technical aspects such as successful recanalization and S-ICH after the procedure. Until now, a direct comparative analysis of clinical outcomes between EVT and medical treatment for M2 occlusion has not been widely performed due to high probability of procedural risk. Our results demonstrated that procedural outcomes were not significantly different between M1 and M2 occlusion after EVT, although M2 branches were small-caliber arteries. Accordingly, further studies delineating specific subgroups of M2 occlusion who can benefit from EVT compared to medical treatment can be justified.
CONCLUSION
Our meta-analysis showed that EVT for M2 occlusion provided an overall successful recanalization rate of 69.1% and SICH rate of 6.1%. No significant difference in successful recanalization and S-ICH was noted according to thrombus location. EVT seems to be technically feasible for acute M2 occlusion. Direct comparative studies between EVT and medical treatment for M2 occlusion are needed further to find specific beneficiary group in patient with M2 occlusion.