INTRODUCTION
Although spinal fusion is the major surgical option for the treatment of degenerative lumbar spinal disease, many studies have reported subsequent mechanical changes and physiological alterations, which can cause unwanted problems, such as, spinal stiffness, the acceleration of adjacent segment degeneration, and chronic low back pain6,7).
Lumbar fusion eliminates motions of functional spinal segments and may overload adjacent segments. Furthermore, surgical trauma and disuse of immobile segments can cause a decrease in paraspinal muscle volume8,23,33). Many authors have addressed the issue of postoperative paraspinal muscle change13,14,17,33). Most have concluded that lumbar fusion affects back muscles and decreases muscle mass regardless of the surgical approach used.
These drawbacks are known to be related to chronic low back pain and failed back surgery syndrome, and have prompted the developments of alternative procedures and techniques for achieving stabilization without fusion, such as, pedicle based dynamic stabilization. Nevertheless the theoretical advantages of non-fusion pedicle based dynamic stabilization (PDS) over lumbar fusion, such as, the prevention of adjacent segment degeneration2,25,27), have not been clearly confirmed or defined18). It has also been reported that PDS can preserve to some extent the motion of stabilized segments1,19). However, no study has investigated the effect that this preservation of motion has upon back muscle changes. In the present study, we studied postoperative back muscle changes after PDS and compared these with back muscle changes after lumbar fusion (LF).
MATERIALS AND METHODS
From February 2005 to January 2008, patients who underwent non-fusion stabilization or fusion were enrolled for this study. The primary diagnosis was degenerative spinal stenosis, and/or degenerative spondylolisthesis. Patients with a history of a previous back operation, revision lumbar surgery, instrumental failure, or perioperative spinal infection were excluded. One senior surgeon performed all surgeries. All patients were followed with our institute routine follow-up protocol, which includes 3-month interval dynamic X-ray and 6-months interval CT scan up to 2 years after operation.
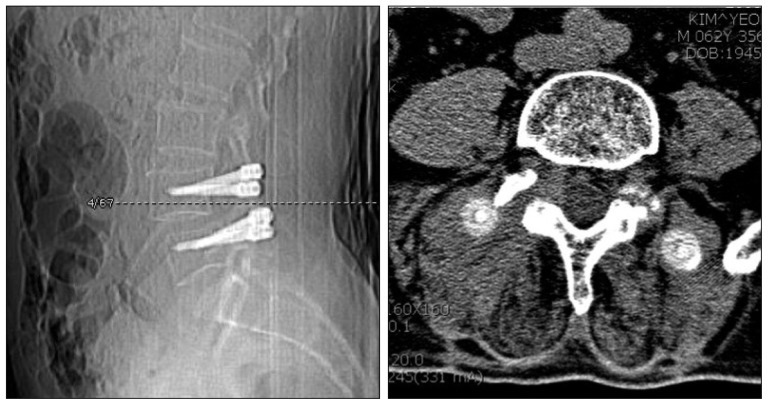
To compare the trend of muscle change with fusion patients, patients with lumbar fusion at L4-L5 segment, operated by same senior surgeon, were enrolled. The author recommended early ambulation, and patients were encouraged to walk immediate postoperative period. There was a difference in wearing time for back brace. It was kept for 3 months after operation in only LF patients, but the patients with PDS did not wear. To quantify muscle changes, paraspinal muscle cross sectional areas (MCSAs) were measured pre- and postoperatively in computerized tomography (CT) images. Postoperative muscle cross sectional area measurements were made using CT scan taken at ≥6 months after operation to allow muscle swelling and edema time to subside31). Last follow-up CT scans were used. The mean postoperative CT follow-up period was 13.0±8.5 months in the PDS group and 13.6±5.4 months in the LF group. We selected an axial cut parallel to the disc space in the lower L4 body level for measuring MCSAs (Fig. 1). This transaxial cut allowed the paraspinal and psoas muscles to be best visualized with less metallic artifact. The cross sectional area (CSA) of the paraspinal muscle and psoas muscle were measured respectively. The CSA of the multifidus muscle, which contributes most to lumbar segmental stability, and which is more directly affected by heat injury during dissection from the adjacent spine and during retraction, was measured separately. We compared the CSAs of these muscles in the PDS and LF groups, and for different surgical approaches. To exclude fatty degeneration of back muscle, regions of decreased density around the muscle were not included in CSA measurements. However, regions of intramuscular decreased density were not excluded due to technical difficulties. The measurements were made using image analyzer software (M-view® version 5.4, Marotech, Seoul, Korea). To test intraobserver reliability, one independent observer repeated measurements three times using the same protocol, and was found to have an accuracy coefficient of 0.71-0.96.
SPSS software (version 12.0, 2003; SPSS Inc., Chicago, IL, USA) was used throughout. The Wilcoxon signed ranks test was used to analyze non-categorical variables, and p values of <0.05 were considered statistically significant.
RESULTS
Thirty-two patients who underwent non-fusion pedicle based dynamic stabilization, including the L4-L5 segments. All patients had interview for surgical approach before operation and only patient who agreed was included for non-fusion stabilization with informed consent and permission of IRB. Posterior midline approach or paraspinal approach was randomly assigned. In the same period, 11 patients was met the same criteria as like non-fusion stabilization during same time period.
In the PDS group, there were 12 males and 20 females of mean age 61.8 years (range 46 to 76 years). All patients in this group underwent pedicle based dynamic stabilization without fusion. The Dynesys® (Zimmer Spine, IN, USA) was used in 21 patients, and the N-flex® (Synthes Spine, West Chester, PA, USA) controlled stabilization system in the other 11 patients. Regarding, surgical approaches, 21 traditional posterior midline approaches (PDS-PM) and 11 minimally invasive paraspinal Wiltse approaches (PDS-PW) were used. In the 11 patients with lumbar fusion and instrumentation (LF) group, there were 7 males and 4 females of mean age 59.8 years (range 37 to 70 years). All patients underwent lumbar interbody fusion and pedicle screw fixation at L4-L5. For lumbar fusion, a traditional posterior midline (LF-PM) approach was used in 7 patients and the minimally invasive paraspinal Wiltse (LF-PW) approach in 4 as described22).
Mean operative time of whole operative procedure including decompression and instrumentation was 204.2±41.8 minutes (range, 120-300) in PDS group, and it was 223.9±65.5 minutes (range, 100-340) in LF group. In PDS-PM group, the mean operative time was 219.1±44.2 minutes (range, 120-300), while it was 178.3±20.4 minutes (range, 90-200) in PDS-PW group. In LF group, it was 250.8±56.2 minutes (range, 100-340) with PM approach, and it was 197.1±40.4 minutes (range, 90-240) with PW approach.
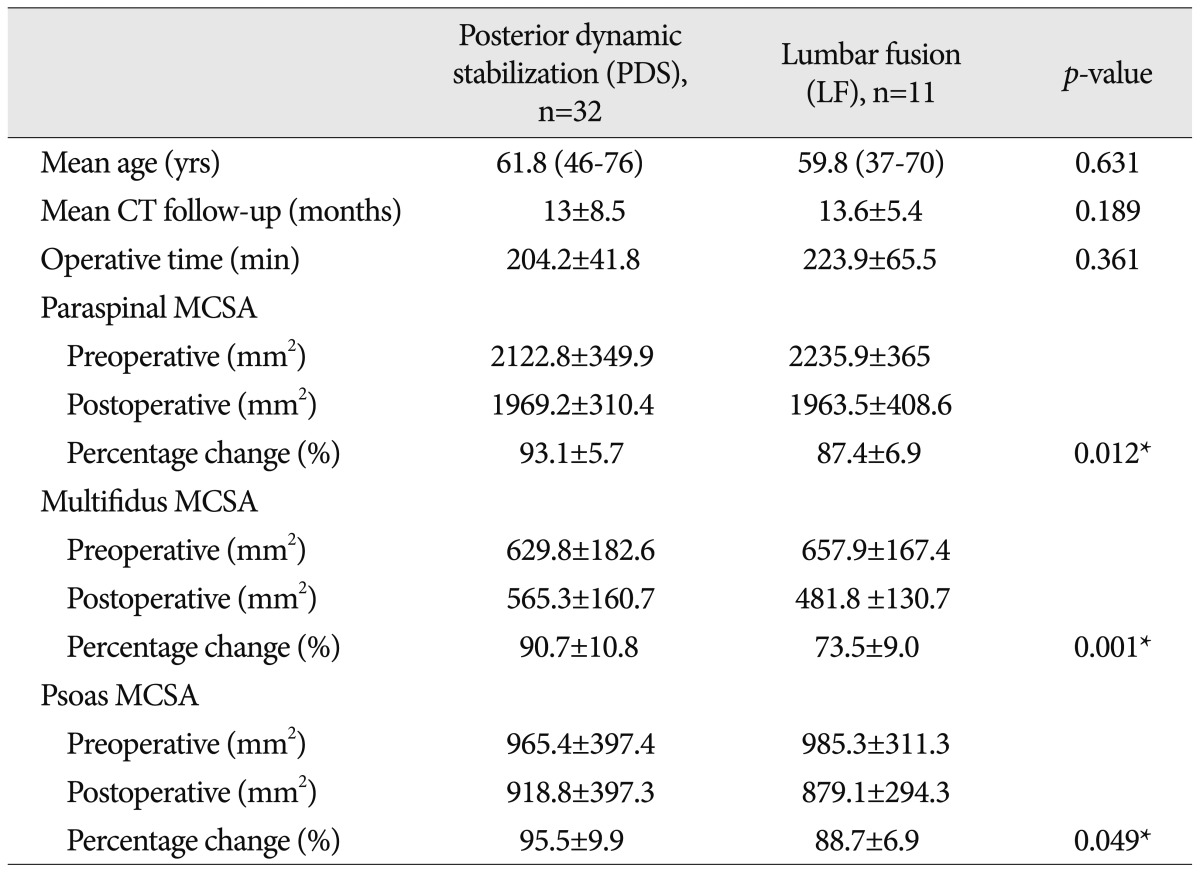
In the PDS group, mean preoperative MCSA of paraspinal muscles (multifidus+longissimus) was 2122.8±349.9 mm2, and mean postoperative MCSA was 1969.2±310.4 mm2, which was 93.1±5.7% of the preoperative value. MCSA decreased by an average of 153.5 mm2. Mean postoperative MCSA of the multifidus decreased from a preoperative mean of 629.8±182.6 to 565.3±160.7 mm2, which was 90.7±10.8% of the preoperative value. Mean psoas MCSA also decreased to 95.5±9.9% of its preoperative value (965.4±397.4 mm2 vs. 918.8±397.3 mm2) (Table 1).
In the LF group, mean paraspinal MCSA decreased significantly (87.4±6.9% decrease, preoperative 2235.9±365 mm2, and postoperative 1963.5±408.6 mm2). Mean multifidus MCSA also showed a significant decrease (657.9±167.4 mm2 preoperatively and 481.8±130.7 mm2 at last follow-up), and this represented an MCSA of only 73.5±9.0% as compared with the preoperative state. The reduction of psoas MCSA mean MCSA was similar to that of paraspinal muscle (88.7±6.9%, 985.3±311.3 vs. 879.1±294.3).
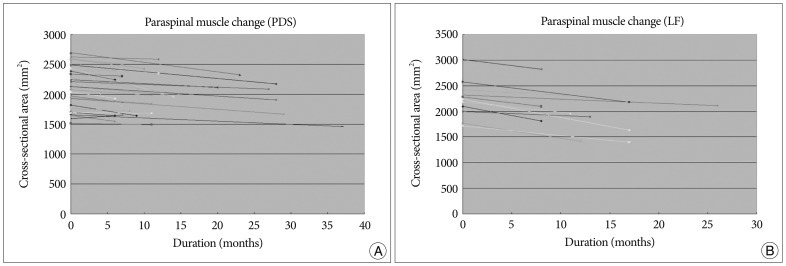
Overall, MCSAs of back muscles decreased in both study groups. The multifidus was the most affected muscle both groups. However, the PDS group showed greater back muscle preservation for all measured muscles. In particular, mean multifidus MCSA decreased more significantly in the LF group. Overall changes in the CSAs of paraspinal muscles (multifidus+longissimus) in the two groups are shown (Fig. 2, 3).
The 32 patients in the PDS group were divided to two subgroups according to surgical approach, namely, into 21 patients that underwent the traditional posterior midline approach (the PDS-PM group, mean age 61.9±7.2 years, mean CT follow-up 13.0±8.6 months), and 11 patients that underwent minimally invasive paraspinal Wiltse's approach (the PDS-PW group, mean age 61.9±9.5 years, mean CT follow-up 13.1±8.6 months).
In the PDS-PM group, mean preoperative paraspinal MCSA was 2124.2±332.1 mm2 and this was decreased to 1954.2±316.4 mm2 (92.2±5.9%). For the multifidus, MCSA decreased significantly from a mean preoperative value of 661.3±196.7 mm2 to a mean postoperative value of 562.4±170.8 mm2 (85.8±10.1%). Mean psoas change in the PDS-PM group was similar to that observed in the PDS group (95.0±11.0%). In the PDS-PW group, paraspinal MCSA decreased from 2120±398.7 to 1997.8±311.6 mm2 (94.8±5.0%) postoperatively, but mean multifidus MCSA did not decrease (569.5±141.1 mm2 preoperatively and 571.0±147.4 mm2 postoperatively), and multifidus MCSA was maintained significantly better in the PDS-PW group than in the PDS-PM or LF groups. Paraspinal muscle changes were slightly lower in the PDS-PW group that in the PDS-PM group (Table 2).
Among 11 LF patients, no significant differences were found between the posterior midline approach and the paraspinal Wiltse approach. In the LF-PM group (7 patients), mean preoperative paraspinal MCSA was 2267.4±196.5 mm2 and this was decreased to 2046.6±165.7 mm2 (90.3±3.9%). For the multifidus, MCSA decreased significantly from a mean preoperative value of 676.8±86.0 mm2 to a mean postoperative value of 510.0±112.8 mm2 (75.0±10.7%). In the LF-PW group (4 patients), paraspinal MCSA decreased from 2268.3±635.2 mm2 to 2000.0±707.2 mm2 (86.9±6.8%) postoperatively, and mean multifidus MCSA was decreased to 76.1±13.5% of its preoperative value (637.8±270.0 mm2 preoperatively and 471.3±161.9 mm2 postoperatively). Mean psoas change was similar in both LF-PM and LF-PW group (88.6±8.5% vs. 90.5±6.4%). Although number of patients was so small to draw conclusion, results revealed minimally invasive LF-PW group did not show better muscle preservation.
DISCUSSION
Posterior lumbar spine surgery inevitably affects back muscles, and may induce subsequent anatomical and physiological changes. Previous studies have determined that dissection and retraction of the paraspinal musculature can lead to denervation and atrophy, and thus, increase the risk of chronic back pain and failed back surgery syndrome6,7,15,30). In particular, after lumbar fusion, paraspinal muscles may undergo atrophy because of the long duration of muscle retraction, large areas of muscle stripping, mechanical and heat injuries to the dorsal rami of the posterior branches, and disturbance of the arterial supply to paraspinal muscles. This muscle atrophy may be exaggerated by postoperative muscle disuse or deconditioning following immobilization of the spine9,10,20,33). These changes in paraspinal muscle functions after fusion may cause chronic back pain and failed back surgery syndrome.
All muscles in the lumbar region contribute to lumbar stability. The multifidus muscle, which is the most important muscle in terms of lumbar segmental stability, is the largest paraspinal muscle located in the most medial portion of the paraspinal muscle. Recent study using architectural design demonstrates that the multifidus muscle is uniquely designed as a stabilizer to produce large forces36). The multifidus, is innervated only by the medial branches of the dorsal ramus without intersegmental nerve supply3), and is the muscle most directly affected by heat injury during retraction and dissection from the adjacent spine. To prevent muscle injuries, intermittent release of the retractor during surgery or different surgical approaches have been recommended12,34,37). The paraspinal Wiltse approach allows manual dissec tion of the multifidus and longissimus muscles to expose the transverse process and lateral aspect of the facet joint with minimal retraction, and thus, this approach may reduce the likelihoods of heat and retraction injuries to paraspinal muscles33). The paraspinal Wiltse approach and the percutaneous fixation technique are known to preserve paraspinal muscles better in fusion patients because severe muscle injuries and paraspinal muscle denervation can be avoided using these approaches11,16,17). Other reports have shown that the minimally invasive approach causes less paraspinal muscle damage than the traditional approach and that it has positive effects on postoperative trunk muscle performance5,11,16). There were few comparative long-term follow-up studies between minimally invasive surgery (MIS) and traditional fusion surgery. Recent two prospective studies revealed that MIS was a method that minimizes damage to the soft tissue and regional muscle immediately after surgery, however, after a period of more than 1 year, there was no significant difference in the paraspinal degenerative change between MIS and traditional surgery21,35). In fact, Remes et al.24) noted that all fusion procedures cause back muscle damage in the long-term. In their report, anterior lumbar interbody fusion, which does not involve the manipulation of back muscles directly, was found to be associated with back muscle atrophy like posterior lumbar interbody fusion and circumferential fusion. This implies that loss of motion affects paraspinal muscle integrity regardless of the surgical approach used, especially in long-term. Accordingly, preservation of motion might play an important role in the maintenance of back muscle integrity besides initial surgical trauma.
Recently non-fusion pedicle-based dynamic stabilization has been introduced as an alternative procedure for the surgical treatment of lumbar degenerative spinal disease. This technique was designed to reduce fusion problems, such as, adjacent segment degeneration and chronic back pain, by permitting limited motion and changing loading patterns at stabilized segments without fusion26,29,32). Although some reports have advocated its advantages over fusion and presented excellent clinical outcomes4,28,38), it is uncertain whether PDS can prevent the progression of adjacent segment degeneration (ASD), and no study has yet documented the real benefit of PDS. However, although it remains unclear whether PDS can prevent ASD, most reports demonstrated that the stabilized segment retains some motion. Thus we focused of the effect of this retained motion at stabilized segments, and sought to determine how preserved motion affects back muscle integrity.
In the present study, we found that both procedures were associated with a decrease in back muscle CSA. However, paraspinal muscle cross sectional area was better preserved in the PDS group regardless of the surgical approach. Furthermore, in the PDS group, the minimally invasive paraspinal Wiltse approach better preserved multifidus muscle. In the LF group, postoperative MCSA decreased significantly more than in the PDS group. We also found that LF did not preserved paraspinal muscles even when a minimally invasive approach was used. Although only 4 of the 11 patients in the LF group underwent a minimally invasive procedure and significance was not critical due to small number of patients, minimally invasive paraspinal lumbar fusion revealed similar back muscle decrease compared to the traditional posterior midline approach. Minimally invasive surgery for lumbar fusion may have benefits during the early postoperative stage, but it may not have long-term benefits. Although initial surgical trauma play a certain role in paraspinal muscle integrity, our results demonstrate that preservation of motion is probably more important than surgical trauma for paraspinal muscle integrity in the long-term. The present study suggests that the preservation of back muscles in the long-term is the real benefit of PDS over LF.
There are several possible explanations as to why PDS better preserves back muscles. First, PDS can preserve some motion at stabilized segments, and this preserved motion helps prevent muscle disuse and atrophy. Second, PDS requires less operative time than LF and causes less injury. Furthermore, PDS does not require fusion bed preparation, facet joint violation, or a bone harvesting procedure, and thus, is less invasive, less traumatic, and less time consuming than LF. We encourage early ambulation and active back muscle exercises, and this probably contributed to the MCSA differences observed between the two study groups.
Some limitations of this study should be clarified. First, because of the retrospective nature of the study, the level of evidence was not strong as prospective ones. Second, the length of the postoperative follow-up period and the number of patients recruited were not sufficient to evaluate long-term outcome. Third, we compared back muscle cross sectional area and did not perform physiologic functional evaluations. Furthermore, we have no data regarding adjacent segment muscle changes, and it is possible that compensatory hypertrophy occurred at adjacent segment in LF patients as Hu et al.10) suggested in experimental study. Finally, we did not study relations between muscle change and clinical outcomes. Nevertheless, despite its limitations, the present study is the first to evaluate muscle changes after dynamic stabilization, and it shows that PDS better preserves back muscles than LF. Furthermore, it suggests that motion preservation at stabilized segments is crucial for the maintenance of postoperative back muscle integrity, and that the surgical approach used also plays a role in back muscle preservation.
CONCLUSION
Pedicle-based dynamic stabilization was found to preserve paraspinal muscles better than posterior lumbar fusion in patients with degenerative lumbar spinal diseases. Furthermore, the minimally invasive paraspinal Wiltse approach was found to preserve paraspinal muscles more than the conventional midline approach in PDS group.
This study also suggests that the preservation of motion at stabilized segments contributes more to postoperative back muscle preservation than initial back muscle injury caused by surgical manipulation and retraction.