INTRODUCTION
External ventricular drainage (EVD) is an important neuro-surgical procedure performing under emergent conditions. The ideal target for ventricular placement is usually within the ipsilateral frontal horn just anterior to the Monro foramen2). Even though the freehand technique using superficial anatomical landmarks is traditional and generally accepted method for EVD, the accuracy rate of EVD catheter placement has been reported about 39.9% to 84%3,45,7). EVD tips locating in nonventricular space have been reported to be 8.2% to 22.4%4,57).
In 1985, the Ghajar Guide was introduced for ventricular catheter placement1), but it was unfamiliar with most neurosurgeon. Currently, navigation guided EVD may increase the accuracy of placement of EVD, but it requires a lot of time and general anesthesia. Thus, it is not suitable and reasonable in consideration of an emergent procedure and cost effectiveness of EVD. The authors introduce a new device for ideal placement of EVD catheter.
MATERIALS AND METHODS
EVD device
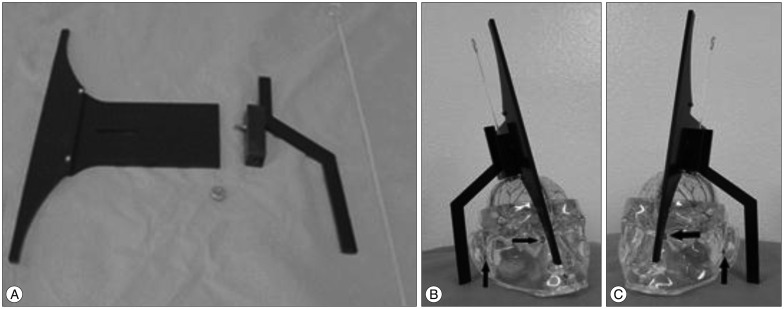
This study was approved by the institutional review board for the medical instrument and its registration number is 2009-08. This device was made of polyoxymethylene. It was designed to direct a ventricular catheter along a course pointing the inner canthus and the tragus. It was composed of three portions, main body, rectangular pillar and an arm pointing the tragus. Main body shaped a large letter T which was composed of horizontal and vertical portions. Vertical portion has a role to direct a ventricular catheter toward the right and left inner canthi, respectively, and horizontal portion has a shallow longitudinal opening to connect the rectangular pillar and move it back and forth. Rectangular pillar is 2×2×8 cm in size and has a longitudinal central hole of 4 mm in diameter to insert an EVD catheter into the frontal horn of the lateral ventricle. Vertical portion pointing the inner canthus was made to be placed coaxially with the central hole of the pillar. On the lateral surface of this pillar, there is a longitudinal groove running parallel with the central hole of the pillar to insert the arm pointing the tragus (Fig. 1).
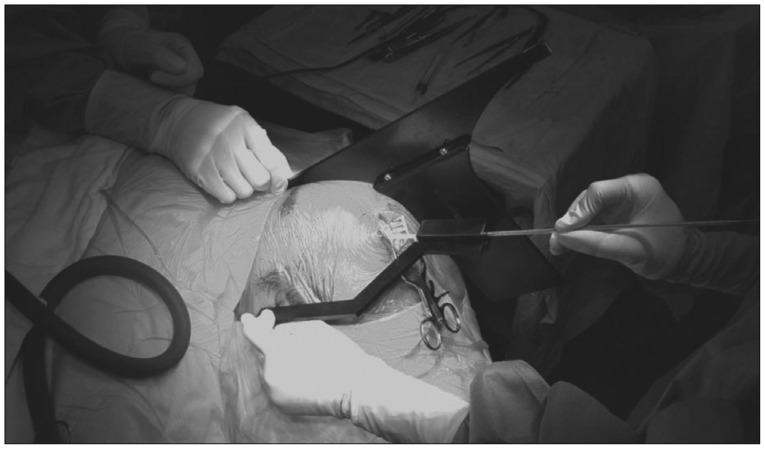
In order to perform an EVD at the Kocher's point, the rectangular pillar was connected with the horizontal portion of main body through its opening using a screw. The arm pointing the tragus was inserted into the longitudinal groove of the pillar. To position the tip of verticalportion toward the inner canthus, the main body was slightly moved from side to side centering the burr hole. The direction of the arm pointing the tragus was also controlled by back and forth movement and turn of the pillar attached to the main body. EVD catheter through the central hole of the pillar was finally inserted into the ventricle in depth of 5.5 cm from the dura mater (Fig. 2). If the thick blood had been pushed out of the ventricle through the EVD catheter due to the increased intracranial pressure in a case of intraventricular hemorrhage (IVH), IVH was aspirated using a syringe of 10 cc.
Patients for EVD
Between April 2012 and December 2014, 57 emergency EVDs were performed in 52 patients using this device in the operating room. Admission diagnoses in 52 patients were aneurysmal subarachnoid hemorrhage in 21, intracerebral hemorrhage (ICH) associated with IVH in 21 (thalamus 15, caudate nucleus 5, pons 1), pure IVH in 2, moyamoya disease in 2, cerebellar infarction in 2, meningitis in 1, ventriculitis in 1, ruptured arteriovenous malformation in 2. Bilateral EVDs were performed in 5 patients who had thalamic hemorrhage and ruptured AVM, aneurysmal subarachnoid hemorrhage, respectively. Postoperative computed tomographic scans were examined in all patients.
RESULTS
All ventricular punctures were accomplished at one time. Catheter tip located in the frontal horn in 52 EVDs and in the 3rd ventricle in 2, in the wall of the frontal horn of the lateral ventricle in 3. Small hemorrhage along to catheter tract occurred in 1 EVD. Even though 3 EVD catheters located in the wall of the frontal horn of lateral ventricle, CSF was well drained.
DISCUSSION
Even though freehand insertion of an EVD using superficial anatomical landmarks is the most common method practiced by young neurosurgical trainees, the catheter tip locations have been reported to be unsatisfactory. EVD catheter placement has been reported to be 39.9-84% in the ipsilateral frontal horn4,56,7), 2.7-12.4% in the contralateral frontal horn4,57), 18% in the lateral ventricle body7), 1.8-10.4% in the subarachnoid space5,7), approximately 10% in the brain parenchyme5,7), 1.8-22.4% in the extraventricular space4,5), and 8.2-19.5% in the third ventricle4,57). Toma et al.7) reported that 40% required EVD revision or reinsertion procedure. They recommended to use neuronavigation, ultrasonography, or other guidance techniques to position the catheter tip accurately in the frontal horn of the lateral ventricle. To increase the accuracy of ventriculostomy at Kocher's point, Ghajar guide was introduced in 19852). It was designed to direct a catheter along a course that lies at a right angle to the cranial surface. This device is rigid and consists of three equal-length standards that are applied to the patient's scalp and a central tube at the apex of the formed pyramid for passage of the catheter. However, Ghajar guide is not familiar with neurosurgeons and is not popularly used. Currently, navigation guided EVD may increase the accuracy of placement of EVD, but it requires a lot of time, room for procedure and frequent general anesthesia. In consideration of an emergent procedure and cost effectiveness of EVD, navigation guided EVD is not suitable. In this presentation, EVD device could be used very conveniently and quickly. When performing EVD using this device, the location of EVD catheter tip can't be reach enough in the frontal horn due to the slight backward movement of the catheter in the process removing the device after ventricular puncture or due to the sight midline shift. In this study, 3 patients showed that catheter tip located in the ventricular wall of the frontal horn. However, In all patients, CSF was well drained and well functioning up to the removal of EVD. There was no problem for CSF drain through the EVD catheter because the ventricular puncture had been already accomplished. In addition, the accuracy of the direction of catheter tip toward the frontal horn was 100%. If the surgeon use this device, extraventricle location of the catheter tip will be never happened. If this device is used in patient with a slight midline shifting, EVD catheter tip can be located in the contralateral frontal horn. The depth of an EVD catheter inserting into the ventricle seems to be suitable to be positioned at a depth of 5.5 to 6 cm from the dura mater. An accurate placement of the ventricular catheter tip is also very important, particularly, in view point of the intraventricular thrombolytic therapy in IVH and the direct conversion of an EVD to ventriculoperitoneal shunt.
CONCLUSION
Freehand insertion of an EVD can be somewhat inaccurate, particularly in beginners. If the neurosurgical residency use this device more than several times during the training course, the accuracy of EVD by freehand technique will be also improved because of the familiar direction of EVD device for ventricular puncture. This device for EVD guides to provide an accurate position of catheter tip safely and easily.