INTRODUCTION
Pituitary adenomas are benign tumors that often extend into the suprasellar space [13,14]. As they grow, the overlying pituitary gland becomes thinned by tumor compression, which then pushes the gland so that it eventually adheres to the overlying arachnoid membrane. During transsphenoidal surgery (TSS), this membrane is very important as it provides a barrier for preventing violation of the suprasellar cisternal space. However, after tumor removal, the redundant arachnoid sinks down into the intrasellar space, often hindering visualization and accessibility to the intrasellar space. When the suprasellar part of the tumor is larger than that inside the intrasellar space, the surgeon must skillfully manage the arachnoid membrane so no remnant remains behind it. In addition, the redundant arachnoid allows delayed hematoma collection in the cavity left behind by the excised tumor.
In our previous publication [5], we demonstrated the effectiveness and convenience of clipping technique for repairing cerebrospinal fluid (CSF) leakage during TSS by using titanium clips and a custom-made clip applier. Based on our experience in the repair of CSF leakage, we found that arachnoid remodeling using the clipping technique is very useful in the management of the redundant arachnoid membrane for enhanced visualization of and accessibility to intrasellar space, as well as and arachnoid remodeling. Herein, we introduce our technique with a description of the technical details, and we demonstrate its effectiveness and safety.
MATERIALS AND METHODS
This retrospective study was approved by Institutional Review Board of Severance Hospital (4-2018-0039). Informed consent was obtained from all subjects that were described for case illustration. Between September 2012 and December 2018, 1342 patients with a pituitary adenoma received a TSS by two neurosurgeons in our institution. We identified 814 cases of pituitary macroadenomas with suprasellar extension. After excluding patients in whom clipping was performed for repair of intraoperative CSF leakage, total 223 patients who underwent arachnoid remodeling with clipping technique were included to this study. All patients underwent preoperative and immediate postoperative (within 48 hours after surgery) 1.5- or 3-Tesla diagnostic magnetic resonance imaging (MRI). Follow-up MRIs were performed yearly after surgery for the first 2 years and every other year thereafter. All tumors were classified by modified HardyÔÇÖs classification scheme [7,9].
Anterior pituitary function was evaluated using a combined pituitary function test (CPFT) that was performed before surgery, 6 months after surgery, and every 2 years thereafter. The changes in pituitary function from before to after TSS were classified into four categories : 1) normal to normal: no pituitary hormone deficiency before or after TSS; 2) improved hypopituitarism: hypopituitarism improved to provide complete recovery; 3) persistent hypopituitarism: the degree of pituitary hormone deficiency did not change after TSS; and 4) worsened hypopituitarism : the degree of pituitary hormone deficiency worsened after TSS. When postoperative CPFTs were performed more than once, the hormone outcome was assessed based on the comparison between preoperative CPFT and the latest postoperative CPFT during follow up. The last of these categories included new development of postoperative hypopituitarism and aggravation of preoperatively existing hypopituitarism. The CPFT was interpreted as previously described [11], as confirmed by two independent endocrinologists. The hormonal outcomes of 166 patients who underwent clipping were compared with those of other patients with pituitary macroadenomas with significant suprasellar extension. FisherÔÇÖs exact test was used to determine the statistical significance of differences in hormonal outcomes. Statistical analyses were performed using IBM SPSS Statistics (version 23.0; IBM Corp., Armonk, NY, USA) and p<0.05 was considered statistically significant.
Operative technique
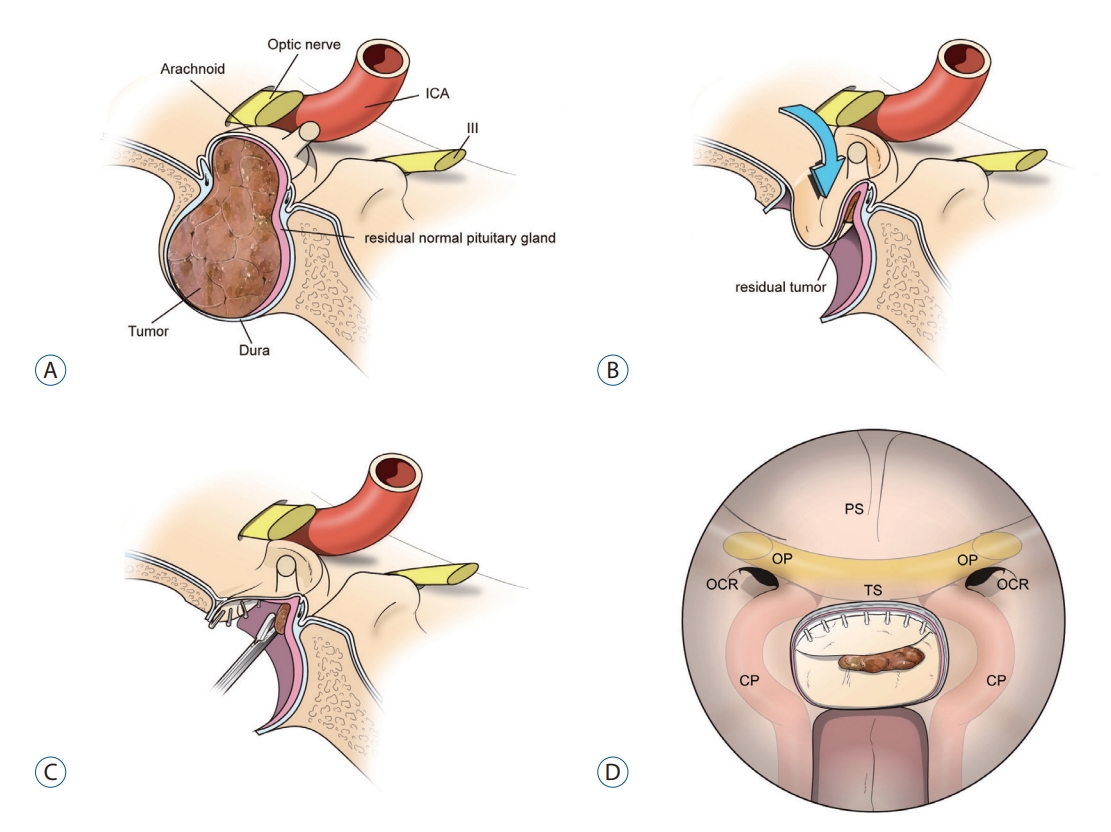
Standard TSS was performed in all patients under microscopic visualization in 182 patients and under endoscopic visualization in 41. After maximal sellar floor opening, the dura was exposed up to the tuberculum sella superiorly and laterally to both medial walls of the cavernous sinus. We preferred making a rectangular dural window, leaving 1-2 mm of dural cuff. Tumor removal was followed by complete removal of pseudocapsule whenever possible. After tumor removal, the overlying arachnoid membrane descended into the intrasellar space with a normal glandular layer. We adopted clip-assisted arachnoid remodeling technique when the redundant arachnoid was thought to hinder direct visualization and accessibility to the space behind it. After meticulous hemostasis, we first checked the thickness of the arachnoid membrane. As the membrane was very thin, and thus floppy, in most cases, the arachnoid was held by grasping forceps and easily lifted to the anterior dural edge. And then we clipped the arachnoid membrane together with the dural edge. We used 2.6-mm-long titanium hemostatic microclips (CLIP 9 Vitalitec; Peters Surgical, Bobigny, France) which are cheap (9 clips/pack, 1.55 USD) and commonly used for neurosurgical procedure such as dural vessel clipping (Fig. 1). In order to apply clips properly, we initially designed a clip applier which has now become commercially available (DS High-tech, Seoul, Korea) [4]. We added several more clips along the dural edge until the redundant arachnoid membrane no longer blocked the surgical route to the intrasellar space (Figs. 2 and 3, Supplementary Video 1).
Occasionally, the suprasellar part of the tumor had a relatively much larger volume compared with its intrasellar space. This resulted in the arachnoid completely occupying the intrasellar space even before the suprasellar tumor came down to the intrasellar space, making manipulation of the arachnoid membrane more technically challenging. In this situation, we started applying clips even when the suprasellar tumor was not yet fully descended. The evaginated arachnoid membrane was hanged with clips securing the route to the remaining suprasellar tumor; this was repeated until the suprasellar part of the tumor completely descended down with its overlying arachnoid membrane (Supplementary Videos 2 and 3). This technique greatly enhanced surgical maneuverability during both microscopic and endoscopic TSS. Furthermore, clipped arachnoid worked as a diaphragm not to re-expand into the suprasellar space by hematoma or packing material. Next, we packed the space previously occupied by the tumor with a fleece-coated fibrin glue patch (TachoSil; Nycomed Austria, Linz, Austria) with or without several pieces of hemostatic materials such as Avitene (CR Bard, Murray Hill, NJ, USA). The entire dural defect was then covered with a piece of TachoSil again. A topical tissue sealant (BioGlue; CryoLife Inc., Kennesaw, GA, USA) was applied for reinforcement. Postoperative lumbar drainage of CSF was not performed in any of our patients.
RESULTS
The 223 patients included 94 males and 129 females, and their mean age was 49.0 years (range, 14-79). Endocrinological and histopathological examination revealed that 193 patients were endocrine-inactive; growth hormone, prolactin, adrenocorticotropic hormone, and thyroid stimulating hormone were positive in 20, five, three, and two patients, respectively. Cavernous sinus invasion was identified intraoperatively in 41 patients (18.4%). Tumors were completely removed in 187 patients (83.9%). The unexpected intrasellar remnant tumors were found only in two cases immediately after surgery.
No patients presented with complications such as infection, visual deterioration, or vascular injury. There were 13 cases (5.8%) of postoperative CSF rhinorrhea that eventually required reoperation, however, majority of them were not directly associated with clipping. On the immediate postoperative computed tomography and MRI, postoperative subarachnoid hemorrhage was identified in six out of 233 patients (2.6%) with arachnoid remodeling, and in 18 out of other 581 patients (3.1%). The incidence of postoperative subarachnoid hemorrhage was not different between two groups (p=0.690). For the 814 patients with pituitary adenomas with suprasellar extension, comparisons between preoperative and postoperative CPFT were available for 595 patients. We compared the anterior pituitary function between the 166 patients on whom arachnoid remodeling was performed and the other 429 patients (Table 1). In the arachnid remodeling group, normal pituitary function was preserved in 44 patients (26.5%). Preoperative hypopituitarism persisted in 32 (19.3%), improved in 68 (41.0%), and worsened in 22 patients (13.3%). Comparison between the two groups showed no statistically significant differences (p=0.517).
DISCUSSION
Pituitary macroadenomas frequently extend into the suprasellar space as they grow. After tumor removal by TSS, this floppy membrane descends down into the intrasellar space due to CSF pressure and eventually occupies the intrasellar space. In this situation, further manipulation of the arachnoid membrane is often technically challenging for both microscopic and endoscopic TSS. The redundant arachnoid membrane often hinders meticulous intrasellar inspection that may result in incomplete tumor resection. To manipulate the evaginated, redundant, arachnoid membrane in an effective manner, we initially tried a purse-string suture technique, which proved to be technically challenging and time-consuming. A snare technique was next attempted [12]. This was very effective for preventing both hematoma formation and CSF leakage; however, it was technically demanding and applicable in only a limited number of cases.
In our previous publication [5], we demonstrated that clipping is a very effective and convenient technique for repairing CSF leakage during TSS. Briefly, when CSF leakage was identified as originating from a defect in the redundant arachnoid membrane, the arachnoid just behind the defect was held by grasping forceps, lifted to the anterior dural edge, and clipped. After clipping, the accessibility and visualization of the intrasellar space was greatly enhanced. We thought this simple technique would be very effective not only for repair of CSF leakage, but also for arachnoid remodeling. We began applying clips for this purpose and found it very useful in most of cases. Owing to arachnoid remodeling by clipping, the routes to intrasellar and parasellar spaces were always secured. Unexpected intrasellar remnant tumors were found in only two patients (0.9%) in our study, which was obviously lower than our old surgical practice (4.9%, unpublished data) before clipping technique was adopted (p=0.022). In addition, as the arachnoid is anchored at the anterior dural margin, thus preventing the arachnoid from being pushed upward or downward, this reconstructed diaphragm may play a role as a buttress, bearing the CSF pressure from above.
Hematoma accumulation in the tumor resection cavity is a common adverse event following TSS for pituitary macroadenomas, one that often leads to compression of the overlying suprasellar neurovascular structures [1-3,8,10]. Moreover, when the arachnoid membrane has a defect in it, hematoma may enter the suprasellar space (subarachnoid hemorrhage), resulting in visual disturbance and possibly even more serious complications such as altered consciousness and hypothalamic injury [6]. Successful arachnoid remodeling by clipping helps prevent these rare but fatal complications. In our early experience, we have experienced four cases of postoperative hematoma in the tumor removal cavity (1.7%). In these cases, the clips were not applied firmly, which resulted in re-expansion of the arachnoid membrane into the suprasellar space. These patients experienced visual recovery in a delayed form. Thus, compared with our surgical practice before we adopted clip-assisted arachnoid remodeling (6.1%, unpublished data), the incidence of optic nerve compression resulting from postoperative hematoma formation in the tumor resection cavity dramatically plummeted owing to our novel technique.
We experienced 5.9% of CSF leakage after surgery in our series which was a little higher than in our other studies. We believe the reason for relatively high incidence of postoperative CSF leakage is that we only included large pituitary adenomas with significant suprasellar extension; many of them were giant adenomas as illustrated in Supplementary Video 3. We experienced the first 10 cases of postoperative CSF leakage in the first 2 years (10 of the first 131 cases, 7.6%). In most of cases of postoperative CSF leakage, the leaking points identified during repair surgery were not matched to clipping sites. Based on the early experiences, we have earned several lessons. First, we never applied clips when normal pituitary gland on the arachnoid was quite thick for two reasons; 1) it was very difficult to apply clips firmly on the dural edge with thick arachnoid as we used very small clips of which length is only 2.6 mm and 2) we also had to concern about possibility that these clips might damage on the pituitary glandular tissue on the arachnoid pouch. Second, when arachnoid is thick, we never used this technique because we were not able to check for the presence of suprasellar vessels beyond the arachnoid. Third, each clip was applied with great care because, once the clip was applied, removal frequently resulted in arachnoid tearing. After we gained experience, postoperative CSF leakage rate was much decreased (three of the later 92 cases, 3.3%), which was comparable with the rate of CSF leakage (3.0%) in 1089 patients of our previous study [4].
We evaluated whether pituitary function was worsened by this technique. However, we found no statistically significant difference in anterior pituitary function between 166 patients in whom arachnoid remodeling was done by clipping technique and the 429 control patients during the same period, providing evidence that this technique does not harm anterior pituitary function and can be used safely. The incidence of aggravated hypopituitarism was 13.3% in this study, which was slightly higher than in the literature and in our previous publication. This is possibly because we only included patients with relatively large tumors with significant suprasellar extension, in which preoperative hypopituitarism is more frequently involved.
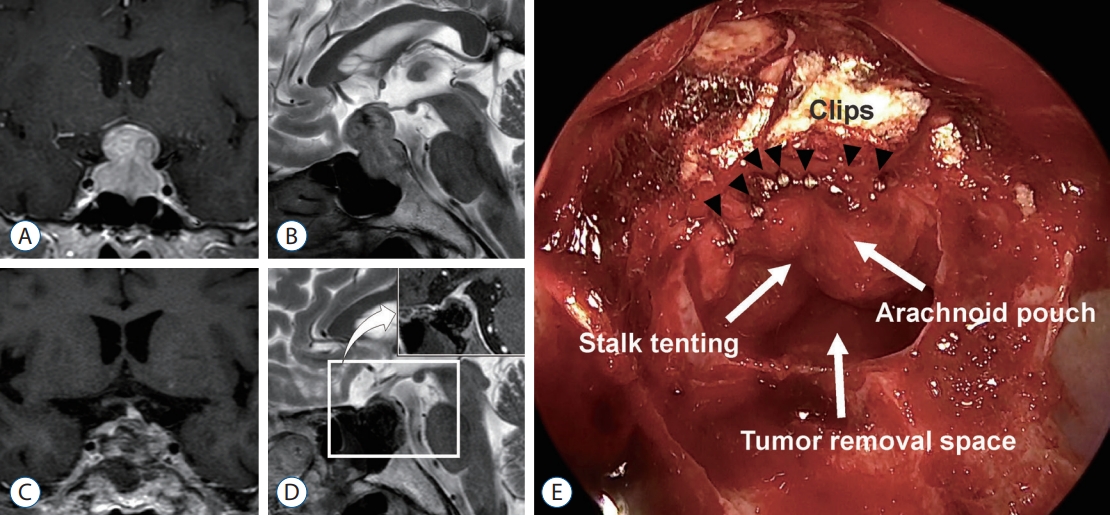
The metallic artifact caused by the titanium clip on MRI is a drawback of this technique. However, as we demonstrated in our previous publication [5], our clips were so small that we did not find significant metal-induced artifact in postoperative MRI (Fig. 3D). Because fewer clips were required for arachnoid remodeling than for type 1 CSF leakage repair, there were almost no noteworthy metallic artifacts in our cases. We carefully inspected the hidden space behind the dural cuff before clipping, so that no remnant would remain that could be later obscured by the metallic artifact on postoperative MRI.
We initially developed this technique for a microscopic TSS. It is true that an endoscope effectively visualized more hidden space behind the redundant arachnoid membrane especially with the aid of an angled endoscope, however, we also found that our technique greatly enhanced the visualization and accessibility in endoscopic TSS. To compensate for the lack of 3-dimensional perception in an endoscopic view, surgeons should confirm proper clip placement by viewing the placement spot from multiple angles before clipping (Supplementary Videos 2 and 3).