INTRODUCTION
Abusive head trauma (AHT) in infants, especially acute subdural hematoma, has an extremely poor outcome. Deaths are common in such cases, and even if the patient survives, severe neurological sequelae, such as delayed mental development, are expected [3,15,16,23,24,28,31,36]. The pathophysiological mechanisms resulting in more severe outcomes have not been fully elucidated. However, an extensive low-density area (eLDA) on head computed tomography (CT) is considered to be a crucial factor in exacerbating outcomes [14,17,18,42].
WHAT IS THE BIG BLACK BRAIN (BBB)?
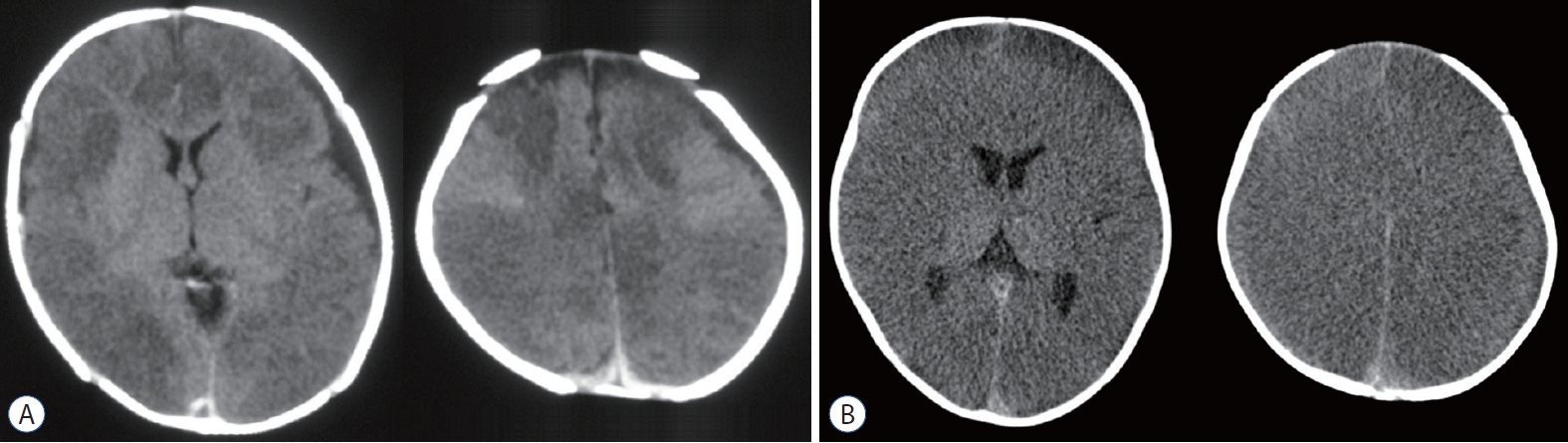
The BBB is a concept advocated by Duhaime et al. [14] and Duhaime and Durham [18]. They described the BBB as hemispheric hypodensity in head CT associated with acute subdural hematoma. This characteristic phenomenon is specific to head trauma in infants and does not occur in adults. It occurs in several AHT cases but can also occur in accident cases. Various physiological stresses, such as hypoxia, hypotension, hypercarbia, and seizures are involved as the onset factors, along with hypermetabolism and hyperpefusion. Recent animal studies have demonstrated that among the above mentioned factors, seizure duration is the most important [11].
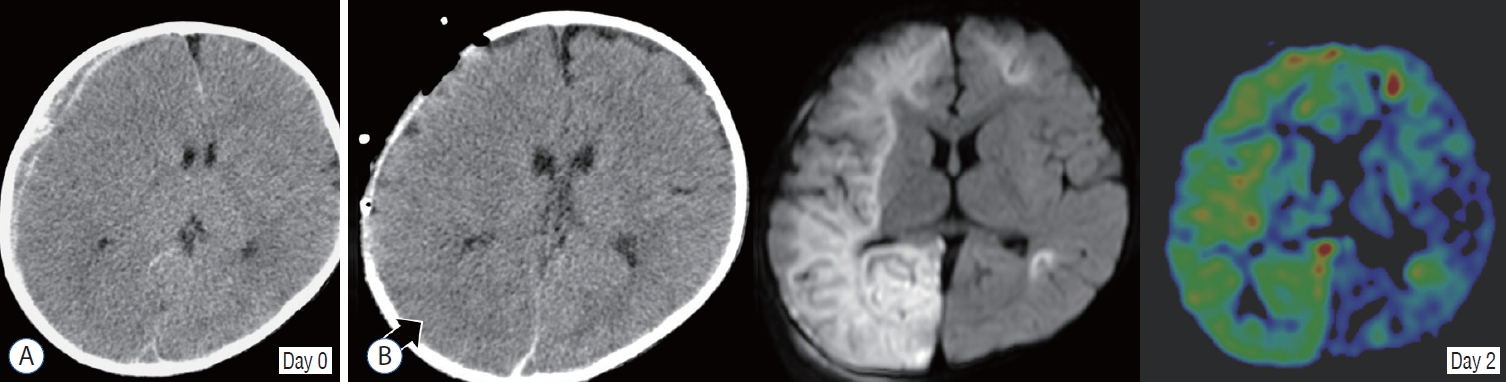
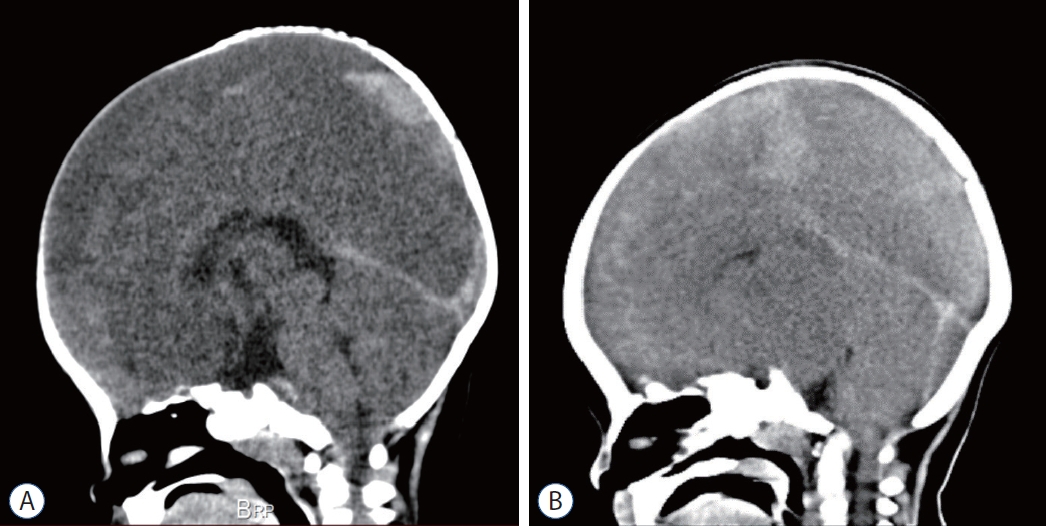
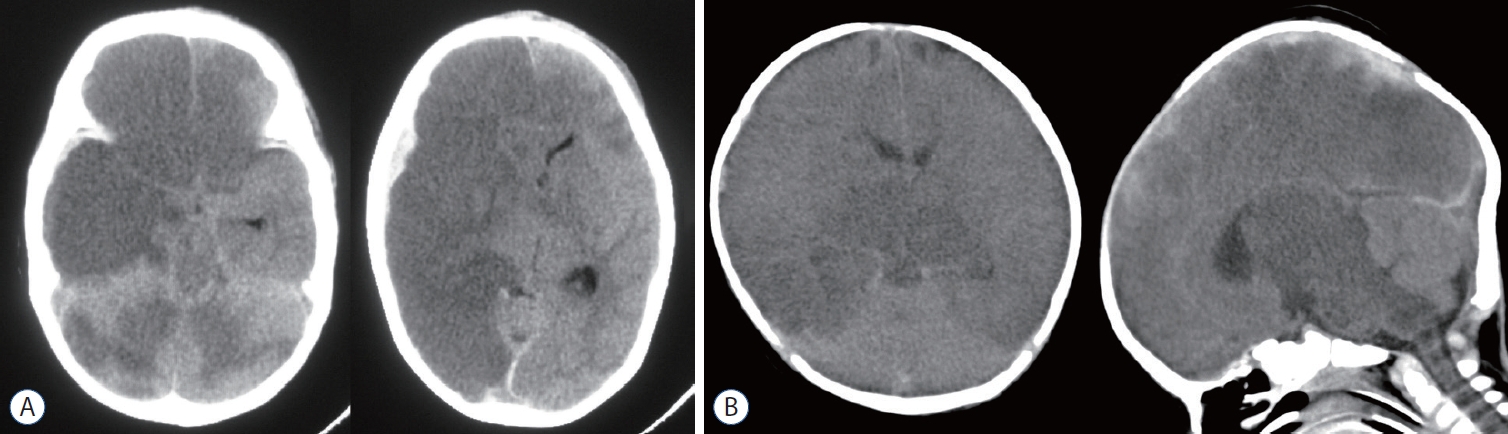
In the original report of the BBB, CT findings were typically characterized by lack of damage to the basal ganglia and thalamus (Fig. 1A) [14,17,18,21]. However, in actual clinical practice, there are many cases where the eLDA extends to the basal ganglia and thalamus (Fig. 1B). Another important fact is the time at which this finding is observed. The BBBs are commonly believed to occur hours to days after head injuries but is often observed on the first CT in some case.
While deepening our understanding of the concept of the BBB, we examined the eLDA pathology, which has a different background from that of the original BBB, and elucidated the cause of aggravation of AHT.
THREE PATTERNS OF extensive low-density area AND THEIR PATHOPHYSIOLOGY
Based on the findings on head CT, eLDA patterns are classified into the following three types according to three factors : when it occurs, where it occurs, and the presence of midline shift (MS).
Pattern A shows that eLDA has already been observed on the initial head CT, is widespread in bilateral cerebral hemispheres, and is not accompanied by MS. Pattern B implies that eLDA has already been observed on the initial head CT, is widely distributed in the unilateral cerebral hemisphere, and is accompanied by severe MS. Pattern C indicates that eLDA appears several days after the injury, may be local or extensive, and is often not accompanied by MS.
It is inappropriate to simply consider the condition that causes eLDA as a cerebral infarction. Other possible pathological conditions include respiratory disorders, brain swelling, status epilepticus (including non-convulsive) [5,26,27,37], hyperperfusion injury [35,38,45,46], arterial compression derived from cerebral herniation, and diffuse brain injury. In addition, there might be an unexplained pathophysiology in infants.
Here, we investigated the possible pathophysiological abnormalities in each pattern. The main pathological condition that results in pattern A is damage caused by respiratory distress, that is, hypoxic ischemic encephalopathy (HIE). Furthermore, in most severe cases, this condition is a typical finding in CPA. The main causes are direct respiratory center damage and traumatic shock associated with head injury, but choking due to vomiting is another cause to be noted. CPA caused by head trauma will be discussed in detail in the next chapter.
Pathological conditions associated with pattern B include status epilepticus and brain swelling immediately after the injury. Infants are more likely to have brain swelling than adults after head injuries. This is related to the effect of water content in the brain and response to hematomas. Finally, the pathology that results in pattern C includes status epilepticus as well as hyper(re)perfusion encephalopathy and mechanical compression of major arteries caused by cerebral herniation.
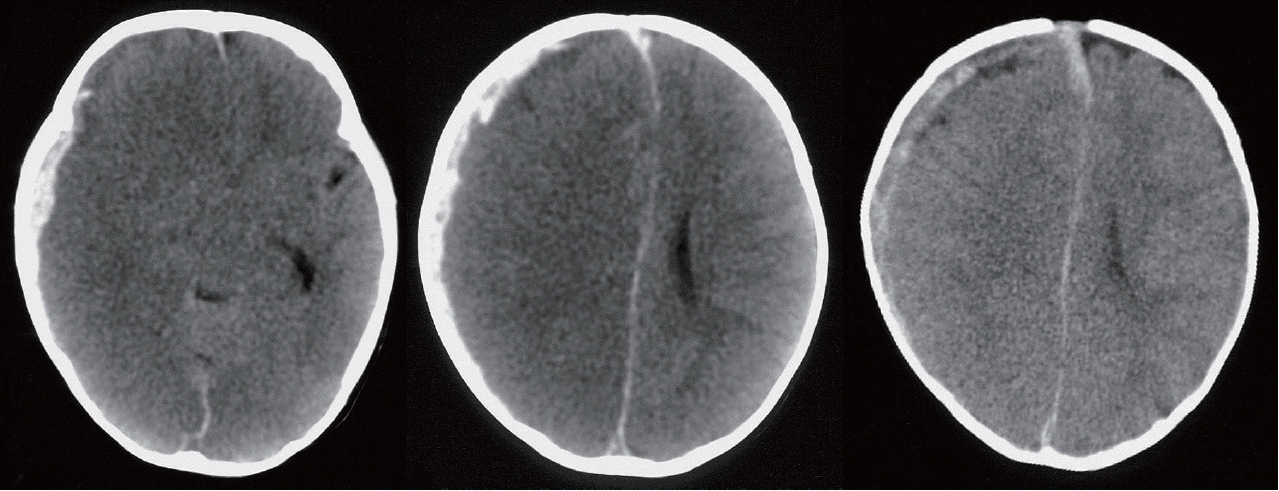
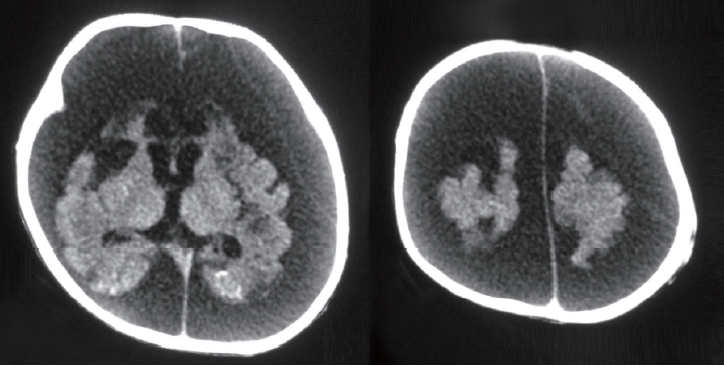
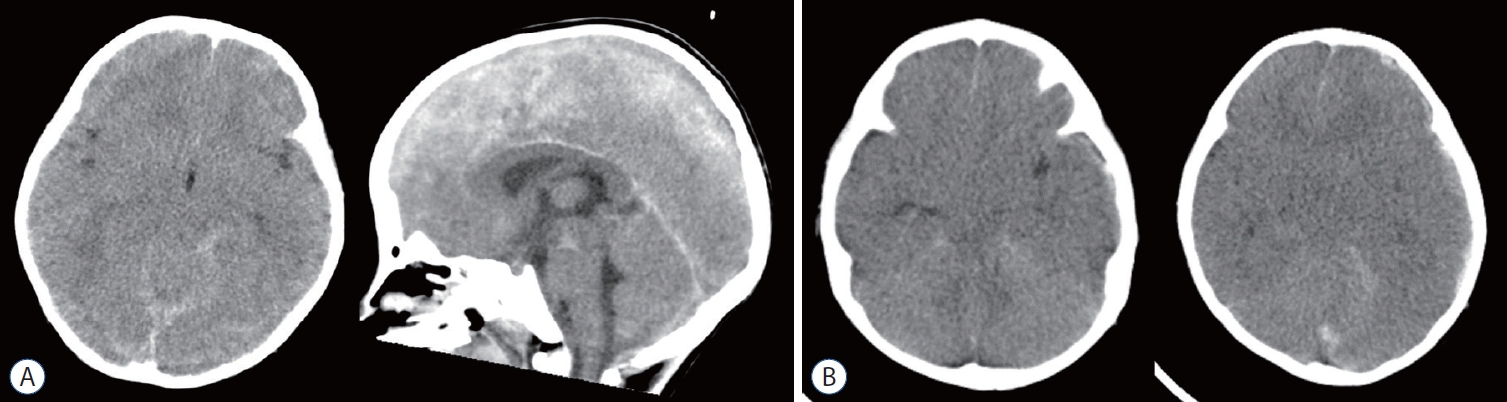
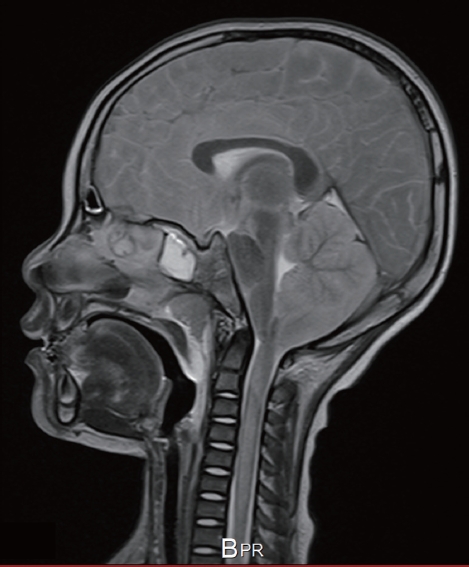
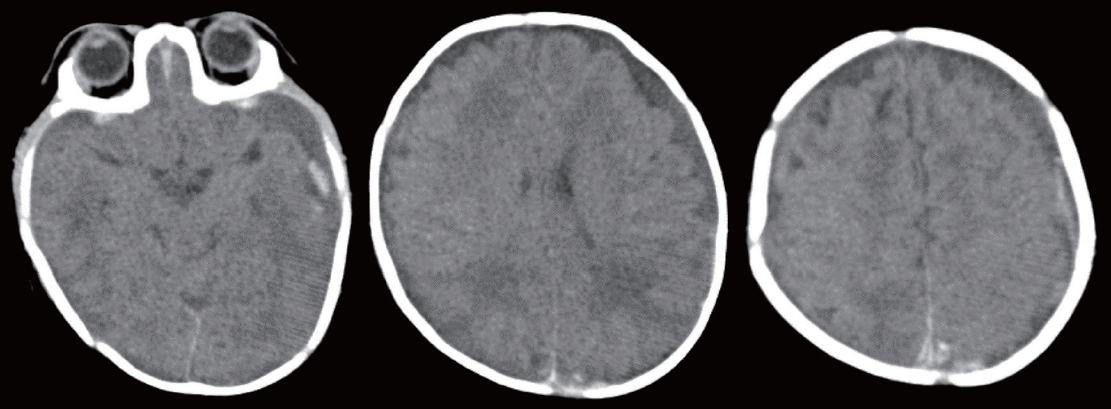
A typical case of each pattern is presented. A 5-month-old girl presented with CPA. Initial CT showed extensive hypodensity changes in the bilateral cerebral hemispheres. LDA extended to the basal ganglia and thalamus. Acute subdural hematoma was also observed in the left cerebral hemisphere, but this might not be the direct cause of CPA (pattern A) (Fig. 2). A 6-month-old girl was thrown on the floor by her father. She was admitted to the hospital because of impaired consciousness and status epilepticus. Head CT showed a right acute subdural hematoma with severe MS and widespread hypodensity in the right cerebral hemisphere (pattern B) (Fig. 3).
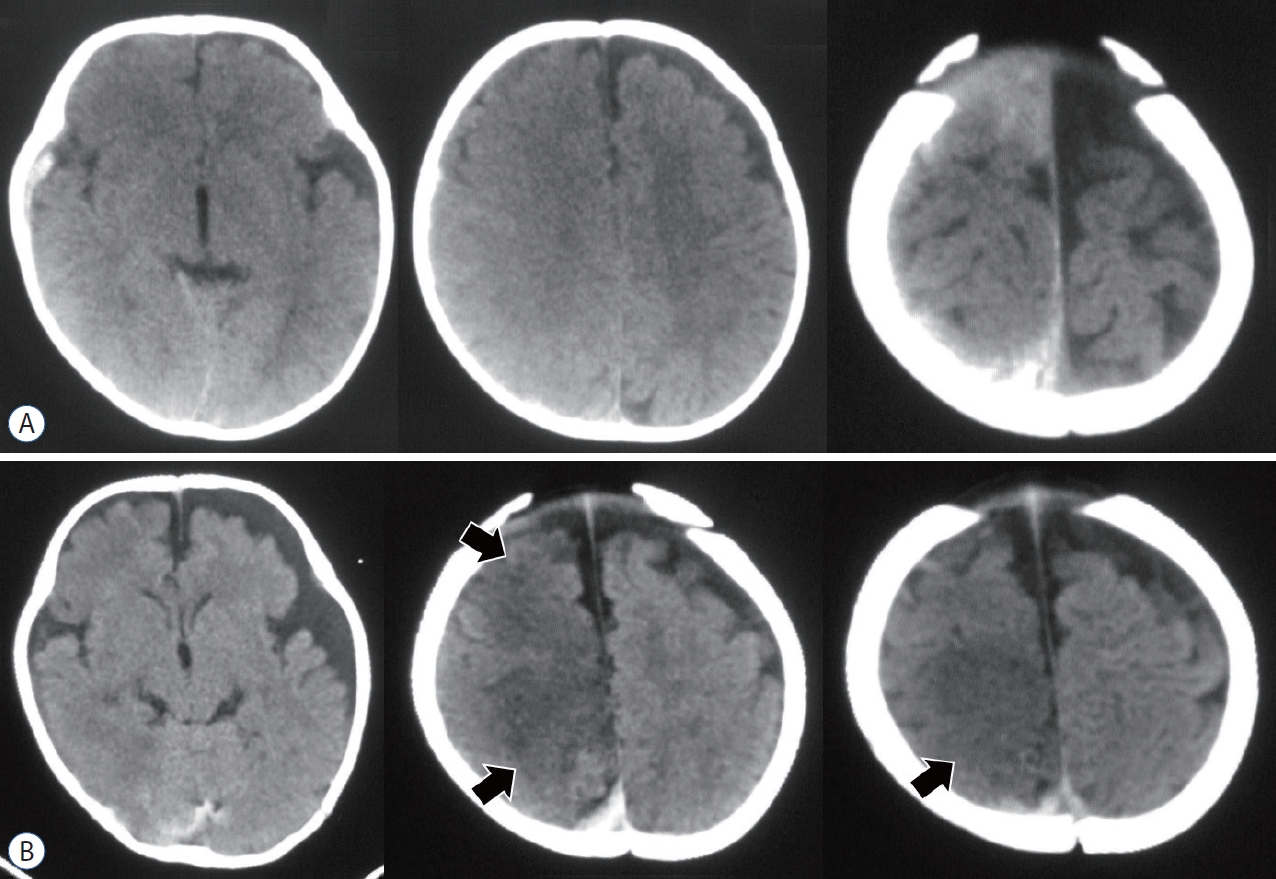
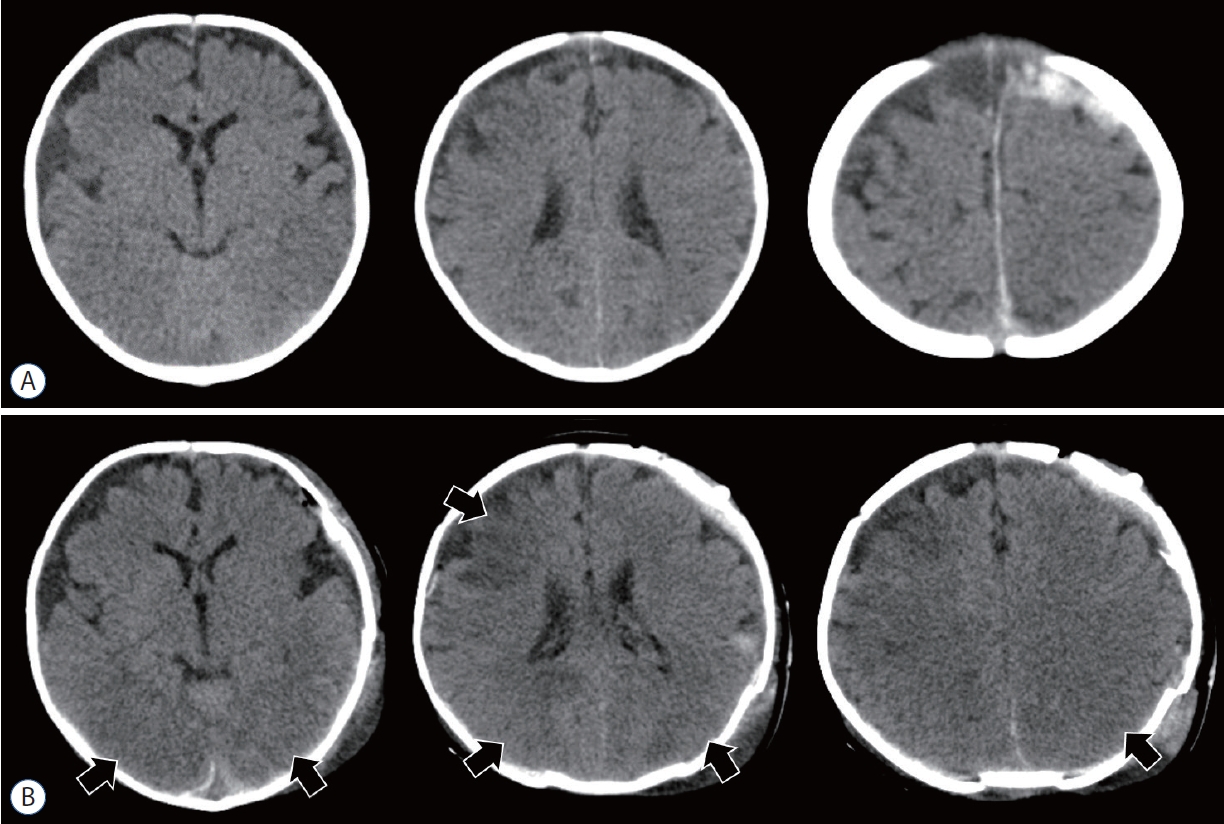
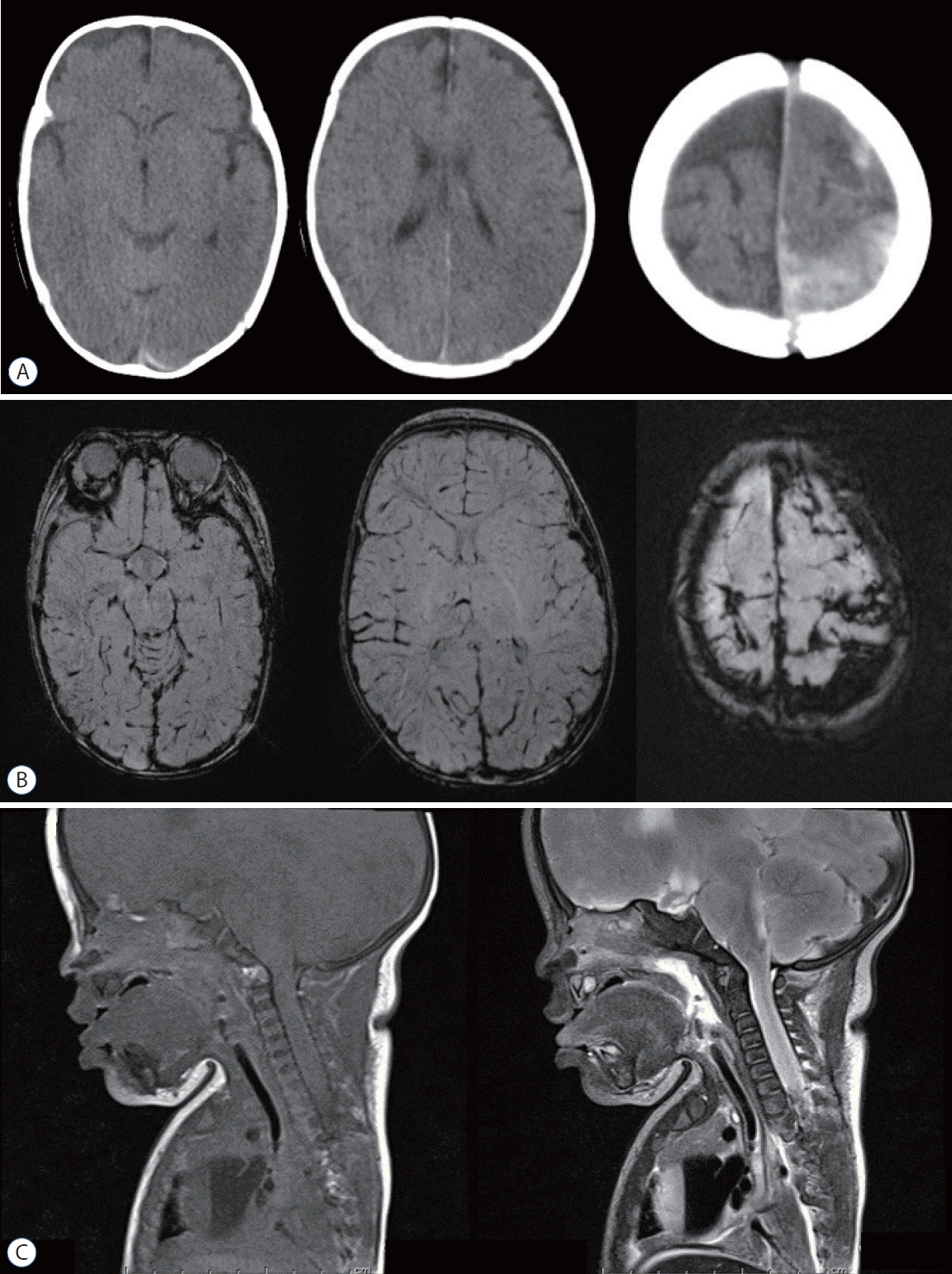
A 4-month-old boy was considered to have shaken baby syndrome (SBS) as the mechanism of injury. The infant was transported to another hospital with status epilepticus. eLDA in the right frontal parietal lobe, which was not visible on the initial CT, was revealed 3 days later (pattern C) (Fig. 4). A 3-month-old girl was also diagnosed with SBS. A craniotomy was performed for the acute subdural hematoma on the left side. Head CT performed 2 days after surgery revealed eLDA in the right frontal lobe and bilateral parietal lobes (pattern C) (Fig. 5).
As mentioned above, eLDA cannot be explained in thorough uniform pathophysiological abnormalities. In the case of AHT, HIE is considered to be an important pathophysiological abnormality, but status epilepticus (Fig. 4) and hyperperfusion encephalopathy after decompressive craniotomy (Figs. 5 and 6) should also be considered as major etiologies of eLDA. In other words, cerebral ischemia alone is not sufficient for explanation. However, once such eLDA is observed, rapid cerebral atrophy associated with cortical lamina necrosis occurs, and the prognosis of neurodevelopmental function is extremely poor (Fig. 7).
WHY DOES AHT CAUSE CPA?
Based on the results of clinical studies reported so far, there are four pathological conditions in which an infant's head injury can be exacerbated by CPA [39]. 1) Cerebral herniation (uncal herniation) : intracranial hematoma and brain swelling cause uncal herniation, and subsequent compression of the brain stem results in impaired consciousness and respiratory arrest. This pathophysiology is a common process from severe head injury to death and is not limited to AHT. 2) Diffuse brain injury : when a strong shearing force is applied to the head, it causes diffuse damage to the brain, including the brain stem, leading to severe consciousness disturbance immediately after the injury and respiratory arrest in the most severe cases. This involves the pathology of clinical diffuse axonal injury (DAI). 3) Injury to the respiratory center : when a direct external force is applied to the medulla oblongata or upper cervical cord, respiratory disorders can occur immediately afterwards. And 4) choking due to vomiting : infants are prone to vomiting after head trauma. The airways are blocked by vomitus, leading to respiratory arrest.
In clinical practice, owing to the presence of anterior fontanelle and unfused cranial sutures, head injuries in infants rarely exacerbate from cerebral herniation to CPA in a short period of time. Without careful observation and proper care within hours to days after injury, intracranial hematomas and cerebral swelling can be aggravated to the worst of CPA. Such cases are judged to be AHT, where the neglect factor is deeply involved.
Diffuse brain injury (clinical DAI) is difficult to diagnose using neuroimaging. Abuse experts have argued that there is extensive primary brain parenchymal injury, only in the presence of subdural hematomas and the presence of widespread LDA in the cerebral hemisphere [7,35,36]; however, this view might be inaccurate. The possibility of HIE due to asphyxia cannot be ruled out.
Therefore, what are the diagnostic imaging findings of primary diffuse brain injury? We must refer to the findings of DAI in diagnostic imaging that have been reported to date. The diagnostic imaging of DAI that occurs in adult cases should also be applied to infant cases. In most DAI cases, micro bleeding occurs in the deep cerebral white matter, corpus callosum, basal ganglia, brain stem, and lateral ventricle, and traumatic subarachnoid hemorrhage (T-SAH) in the basal cistern and peri mesencephalic cistern [1,20,32,33]. In some cases, acute diffuse brain swelling occurs, resulting in narrowing of the ventricular and cistern systems [10,44]. Head trauma experts believe that DAI occurs when these decisive findings are observed on the first head CT scan and causes a serious impairment of consciousness (Fig. 8).
In few cases, such findings cannot be observed. Thus, other etiologies should be considered. It can be said that this is the limitation of AHT diagnosis by neuroimaging (Fig. 9).
When the brain stem, especially the medulla oblongata, is directly damaged by head injury, not only consciousness disorder but also respiratory disorders occur immediately after the traumatic event, resulting in CPA in the worst-case scenario [19,30,34]. Traumatic primary brainstem injury should be evaluated using magnetic resonance imaging (MRI) findings. However, MRI examination is often dangerous in situations of unstable circular breathing. In rare cases, primary brainstem injury can be detected by CT, but in most cases, the artifacts associated with thick bony structures of the posterior fossa interfere with the diagnostic imaging of brainstem injury. Therefore, how should we diagnose primary injury of the medulla oblongata? The presence of hematoma on the posterior surface of the clivus can be an indirect finding of medulla oblongata injury (Fig. 10A). The other is the finding of an early edema with brainstem swelling (Fig. 10B). Brainstem damage derived from hypoxia or hypoperfusion does not cause swelling at an early stage.
Of course, it is the most useful rationale if an autopsy can prove traumatic primary damage to the medulla oblongata. This might include pathohistological diagnostic findings, such as DAI [2,22,43,47].
Upper cervical spinal cord injury is another important non-negligible factor that increases the severity of AHT [8,9,25]. To elucidate why CPA occurs, it is necessary to consider the possibility of upper spinal cord injury. In the case of a traffic accident or a fall accident from a high place, the golden rule of the initial treatment of trauma is to treat spinal cord injury regardless of age. In infants and children, a peculiar pathological condition may occur called spinal cord injury without evidence of radiologic abnormality (SCIWORA), which is a spinal cord injury without bone injury [6,40,41]. It might be easy to imagine the mechanism by which violent shaking causes severe SCIWORA and, in the worst-case scenario, respiratory arrest. However, one major blind spot is that only the findings of acute subdural hematoma and HIE in head CT are focused on and establishing the diagnosis of AHT is discussed, but the evaluation of upper cervical spinal cord injury is unfocused. It may be unavoidable that spinal cord MRI cannot be evaluated in CPA cases, but it is extremely problematic that spinal cord evaluation is often missed by close examination in autopsy. Retinal hemorrhage, multiple rib fractures, and long bone fractures are recognized as important extracranial injuries in AHT diagnosis, but ligamentous neck and/or spinal cord injury is also extremely crucial, especially in CPA cases (Fig. 11).
Additionally, the pathophysiology that must be kept in mind regarding the mechanism of CPA in infant head trauma is asphyxia due to vomiting. Vomiting occurs frequently in children with head injuries, especially in infants. Furthermore, infants have anatomical feature of a large tongue and a small trachea, and physiological feature of having more secretions in their laryngopharynx with a weak cough reflex. Regardless of the severity of the head injury, vomiting causes choking, and accidental injuries result in CPA in the worst-case scenario (Fig. 12). It is inaccurate to make an instant diagnosis of violent trauma solely based on a CPA case. Asphyxia due to vomiting can occur in either AHT or accident. Thus, additional evidence is required to judge AHT.
Of these four etiologies, diffuse brain injury and injury to the respiratory center can almost certainly be caused by AHT. Unless there are obvious assault assumed findings, such as multiple skull fractures or other physical injuries, it is important to note that the pathophysiology that resulted in CPA due to cerebral herniation or choking cannot be judged as definite AHT.
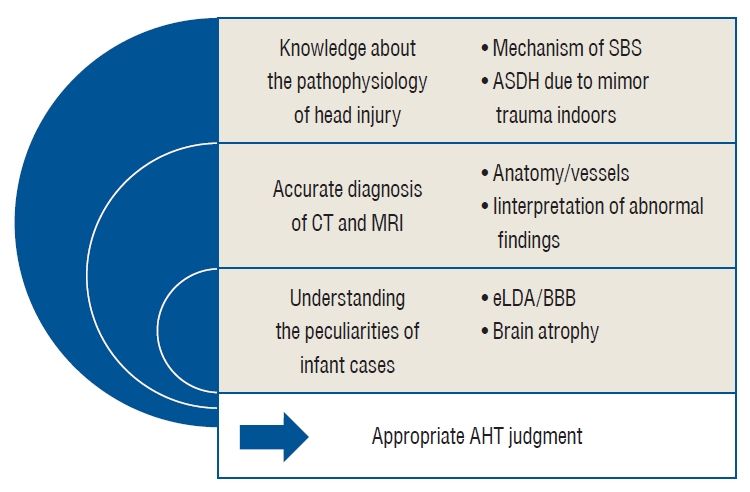
As mentioned above, it is not easy to determine whether a case of infantile acute subdural hematoma with CPA might be AHT. Appropriate and accurate diagnosis requires familiarity with head trauma and infant-specific anatomical and physiological characteristics (Fig. 13).
FACTORS THAT CAUSE AHT TO BECOME SEVERE AND RESULT IN POOR OUTCOME
Most AHT cases become severe and have poor outcomes, and it is necessary to consider various pathological conditions and backgrounds as etiological factors.
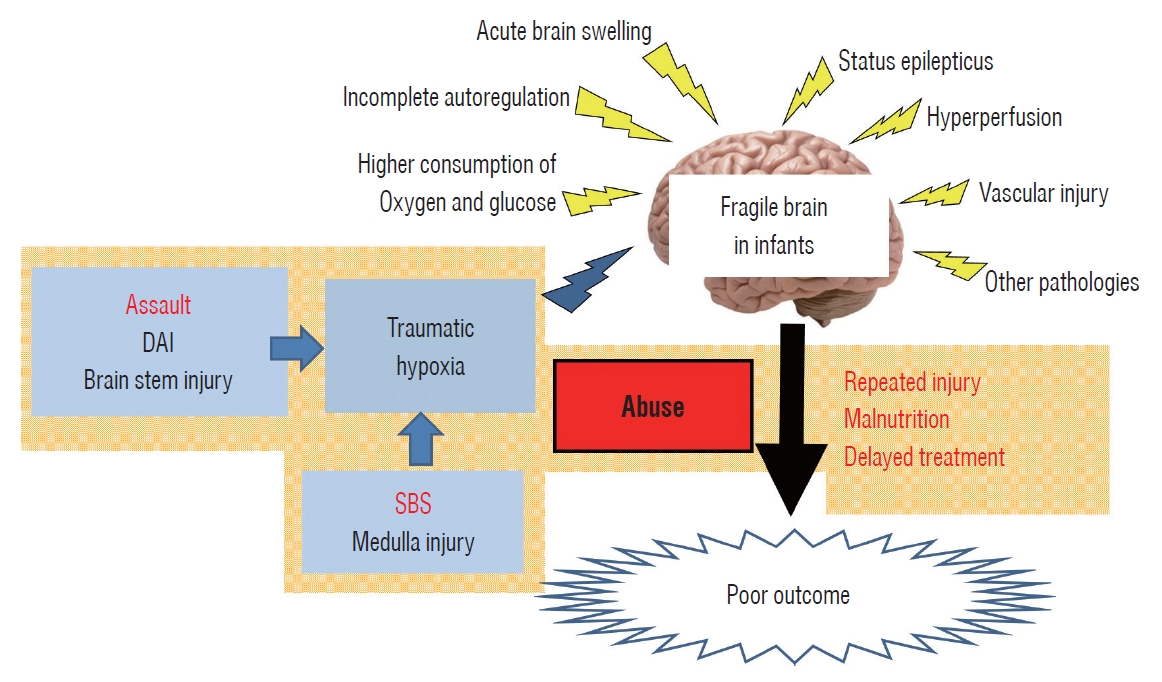
The main factors are summarized as follows. 1) Occurrence of eLDA discussed so far (this condition is not specific to AHT), 2) severe brain injury that causes CPA, specifically diffuse brain injury or direct damage to the medulla oblongata and upper cervical spinal cord, and 3) the social background peculiar to AHT. It should be considered that these factors are associated with in a complex manner (Fig. 14).
Occurrence of eLDA causes significant cerebral atrophy. Rapid and progressive cerebral atrophy can occur days to weeks after a head injury, which is extremely rare, not only in adults but also in children. Physiological features of an infant's brain include immature autoregulation, high oxygen consumption, and high glucose consumption. Their brains can be affected by traumatic primary brain injury and various secondary injuries caused by subdural hematomas, which can result in irreversible damage to the brain. Despite the expected growth and development of the brain, catastrophic damage occurs. In most cases, primary contusion injuries due to head trauma are absent or mild. Nevertheless, it should be recognized that AHT can cause brain atrophy and severe neurodevelopmental retardation.
Furthermore, when violent shaking is applied, in addition to respiratory disorders due to excessive passive movement of the cranio-cervical junction, extension vascular damage can affect the internal carotid artery and vertebro-basilar artery. This conception might be a new finding when considering the aggravation mechanism in AHT (Fig. 15).
Additionally, the specific problems of AHT cases are repeated physical assaults, malnutrition due to care neglect and delayed visits to the hospital, that is, medical neglect. Time is of the essence in treating head injuries. However, despite such emergencies, we have experienced many cases of delay in reporting to the hospital.
In cases of respiratory arrest or CPA at the time of transportation or visit, a poor outcome is inevitable regardless of the treatment.
CONCLUSION
The widespread LDA found in AHT head CT findings is not caused by a single pathology, but by the complex and overlapping additional effect of various harmful physiological factors to the brain of vulnerable infants. The pattern of eLDA that occurs days after injury is not appropriate to be considered a simple ischemic change. Pathological conditions such as status epilepticus and hyperperfusion injury are deeply involved. The pattern of eLDA that occurs early after a head injury is unlikely to occur except for severe disturbance of consciousness and hypoxic-ischemic changes due to CPA, and it is important to identify the cause. In-depth knowledge and abundant clinical experience of such pathological conditions are essential for appropriate AHT judgment.