INTRODUCTION
Cerebral vasospasm (CVS) with delayed ischemic neurologic deficit (DIND) is a well known serious complication of aneurysmal subarachnoid hemorrhage (aSAH), occurring in 20% to 40% of patients [1]. It is characterized by arterial narrowing seen on cerebral angiography and presents as a neurologic deficit after aSAH [9]. Although the exact pathogenesis of DIND after SAH is not entirely clear, a thick subarachnoid clot filling with cistern or fissure had been regarded as an independent predictor [5].
CVS with DIND after unruptured aneurysm clipping surgery is extremely rare. To the best of our knowledge, there are 14 cases with DIND after unruptured aneurysm surgery in the literature, with one study reporting only a 0.08% incidence rate for 2427 patients [19]. Perhaps because of its rare incidence, there has been little attention paid to this condition.
We report two cases of CVS with DIND from 1075 patients who underwent unruptured clipping surgery between January 2010 and April 2020 at a single institution. We also review the literature to provide additional clinical and pathological information on this rare neurologic complication to contribute to the understanding of DIND after unruptured aneurysm surgery.
CASE REPORT
Case 1
History and examination
A 51-year-old right-handed woman underwent magnetic resonance imaging (MRI) of the head to investigate intermittent headache and an unruptured aneurysm was observed. A cerebral angiogram showed a 5-mm-diameter left anterior communicating artery aneurysm.
Operation
A left small supraorbital craniotomy exposed a lesion at the A1-A2 junction. Careful dissection of the aneurysm revealed a fragile wall with a daughter sac. The aneurysm had adhesion to the frontal lobe and a small perforating artery. During dissection of the aneurysm, it ruptured. Immediately, a temporal clip was applied to the left A1, and a permanent clip was successfully applied to the neck of the aneurysm.
Postoperative course
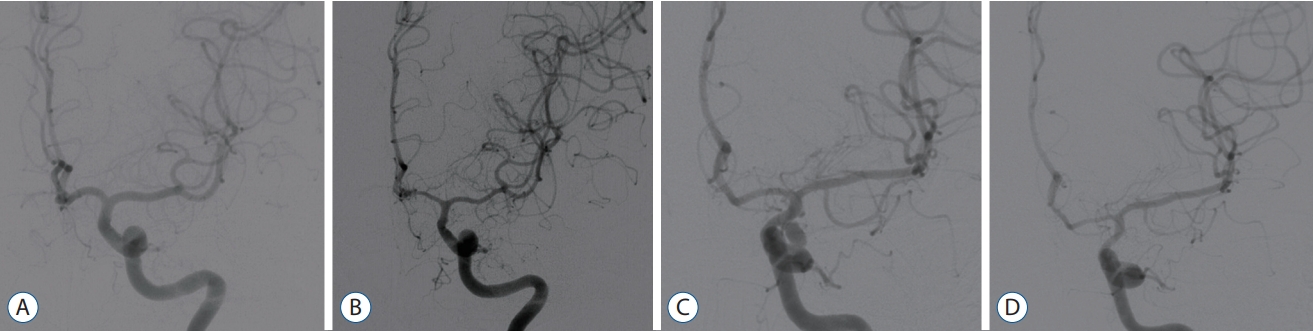
A routine postoperative computed tomography (CT) scan on the next day following surgery showed no blood in the sylvian fissure and basal cisterns. A postoperative CT angiogram showed successful clipping of the aneurysm and no vasospasm (Fig. 1A). The patient was discharged on postoperative day 8 without any neurological deficit. On postoperative day 14, however, motor dysphasia developed. Emergency MRI showed no acute infarction. A subsequent cerebral angiogram revealed vasospasms at the left proximal anterior communicating artery and left middle cerebral artery (MCA) (Fig. 1B). The vasospasms were treated with a 2 mg intra-arterial (IA) nimodipine injection. The patient was discharged with no residual neurological deficit.
Case 2
History and examination
A 45-year-old woman presented with a 1-day history of oculomotor nerve palsy of the left eye caused by an unruptured posterior communicating artery (PCoA) aneurysm (Fig. 1C). She had suffered from ptosis of the upper eyelid and the upward, downward, and medial gaze of the left eye was significantly impaired. The pupil was also dilated and slightly reactive to light.
Operation
She underwent surgery via a supraorbital craniotomy on the day of admission. The aneurysm was laterally positioned below the sphenoid wing. After drilling of the sphenoid wing, neck clipping was successfully done. A puncture of the aneurysm fundus was not undertaken. There was no rupture event during the operation.
Postoperative course
Immediate postoperative CT showed no subarachnoid hemorrhage. On postoperative day 2, the left ptosis was completely resolved, and gaze impairment also recovered. She had no neurologic deficit until postoperative day 12. On postoperative day 12, she presented with motor dysphasia and right hemiparesis. Cerebral angiography revealed significant vasospasm on the left A1 and M1 segment (Fig. 1D). After the IA nimodipine injection, the vasospasm was resolved on follow up angiography. The patient also fully recovered a few days after IA nimodipine.
DISCUSSION
CVS with DIND after unruptured aneurysm surgery is rare. We provide a review of the relevant literature. Then we discuss possible causes including hemorrhage, mechanical stress, and TCVS. Then we review our two cases with respect to these three possible causes of pathogenesis.
In our review of the literature, there have been 14 previous cases of CVS with DIND following unruptured intracranial aneurysm surgery [3,4,10,11,14,16,17,19]. All cases had no SAH prior to unruptured aneurysm surgery. Clinical characteristics, artery of origin, size of aneurysm, time to onset of DIND, and postoperative courses are described in Table 1 [3,4,6,10,11,14,16,17,19,20]. Thirteen patients who suffered from DIND after unruptured clipping surgery were female, and only one patient was male. All aneurysms and CVSs after surgery were in the anterior circulation. All vasospasms were localized at the site of approach for the aneurysm. The size of aneurysm varied from 4 mm to 8 mm, and did not include large aneurysms. Two of 14 cases showed perioperative hemorrhage after postoperative CT, and the other 12 cases did not show postoperative hemorrhage. Paolini et al. [17] reported their vasospasm cases presented a small perioperative hemorrhage in the frontal lobe due to brain retraction after uneventful aneurysm surgery. The onset times of DIND varied considerably, ranging from 16 hours to 28 days after surgery. The mean onset time was 10.5 days for the 14 unruptured aneurysm patients. Three cases of early vasospasm occurred within 4 days after the operation, and 11 cases were delayed.
The first and most common cause of CVS with DIND is hemorrhage. In subarachnoid hemorrhage, several chemical products generating by erythrocyte and their breakdown products such as oxyhemoglobin have been regarded as a mediator of vasospasm. Oxyhemoglobin released from lysed erythrocytes produces reactive oxygen species (ROS) that activates the Rho kinase and protein kinase C pathways, which are known to cause smooth muscle contraction [13]. In addition, ROS and oxyhemoglobin may inhibit nitric oxide (NO) synthase thereby decreasing the levels of NO, which can have a direct effect on arterial smooth muscle contraction. In addition, the production of endothelin, the most potent vasoconstrictor in both vascular endothelial cells and smooth-muscle cells generated by oxyhemoglobin, also may have a significant role in the pathogenesis of CVS [13]. Because of these mechanisms, a thick subarachnoid clot filling with a cistern or fissure has been regarded as an independent predictor of CVS [5].
The second cause of CVS with DIND is mechanical stress. Mechanical stress is caused by operative manipulation and is another possible factor of cerebral ischemia after an operation. Dissection of the sylvian fissure, manipulation of MCA branches, and clipping and manipulation of the sac to dissect adhesion that irritates the endothelium of the aneurysm may induce a vasocontraction response along the vessels. Surgical manipulation of an aneurysm sac next to the midline on the hypothalamus has also been suggested as a possible mechanism of CVS after unruptured ophthalmic aneurysm surgery. However, these mechanical stresses influence the acute phase of an operation, so delayed onset of CVS suggests that mechanical stress may not explain all cases.
The third cause of CVS with DIND is the trigemino-cerebrovascular system (TCVS). TCVS has been also suggested as a possible factor of DIND and CVS. TCVS, the complex nerve network surrounding the arteries of the Willis circles, may be involved in maintaining a normal vessel diameter by the release of vasodilatory peptides [18]. Calcitonin gene-related peptides (CGRPs) are among the most potent microvascular vasodilatory peptides. Vasoconstriction is supposed to be associated with a decrease in CGRP levels in the nerves and an increase in CGRP levels in blood [15]. In SAH patients, the level of CGRP has been significantly decreased in severe CVS patients [7]. This suggests that the stimulation of TCVS nerve endings by blood breakdown products or surgery itself is supposed to activate the release of CGRP, which can lead to a delayed depletion of these CGRPs and may induce vasospasm [2,7].
The first case of our reports presented non-hemorrhagic symptomatic CVS after elective clipping surgery. Although there was no perioperative hemorrhage on the postoperative CT scan, the aneurysm instantaneously ruptured during the operation. In the previous literature, mechanical stress occurring on the arterial wall has been investigated as possible source of spasm [8,12]. We suggest that a momentary rupture can provoke stress on the arterial wall, which may cause mechanical stress and be a possible factor of DIND.
The second case of our reports may be caused by a combination of mechanical stress and TCVS. To the best of our knowledge, there are no reports of DIND where the operation for an unruptured PCoA aneurysm was associated with oculomotor nerve palsy. During the operation for the neck clipping, drilling of the sphenoid wing was performed. Kitazawa et al suggested that drilling of the anterior clinoid process and incision of the dural ring can be responsible for causing vasospasm following internal carotid artery (ICA) aneurysm clipping surgery [14]. As sphenoid wings are near the anterior clinoid process and the dural ring of ICA, drilling of the sphenoid wing might provoke mechanical stress causing vasospasm. It may also be correlated with the stimulation of TCVS. The ophthalmic division of the trigeminal nerve that is innervated with intracranial vessels, meninges, and dura can be stimulated by mechanical stress due to drilling [7,18].
CONCLUSION
CVS and delayed ischemic neurological deficit after unruptured aneurysm surgery is very rare. Its etiology and pathophysiology can be triggered by many mechanisms, such as chemical stimuli of blood breakdown products caused by hemorrhage, mechanical stress to an arterial wall, or TCVS. However, several cases show that vasospasm may recover with appropriate treatment. For unruptured aneurysm surgery, clinicians can keep in mind that careful observation and treatments may be needed for potential postoperative CVS with DIND.