INTRODUCTION
An isolated dissecting aneurysm in the posterior inferior cerebellar artery (PICA) is an extremely rare condition. There are several reported cases in which the treatment methods varied15,1621). Because endovascular or surgical obliteration of the dissected segment involving a pseudoaneurysm could result in ischemic complications in the medulla and distal cerebellar vascular territory, several methods of revascularization have been introduced4,610,1117).
We have experienced a dissecting aneurysm occurring at the lateral medullary segment7) of the PICA that resulted in subarachnoid hemorrhage (SAH). For obliteration of the lesion, revascularization was also required. We have performed intersegmental anastomoses between the proximal and distal caudal loops of the PICA in situ following trapping of the aneurysm.
CASE REPORT
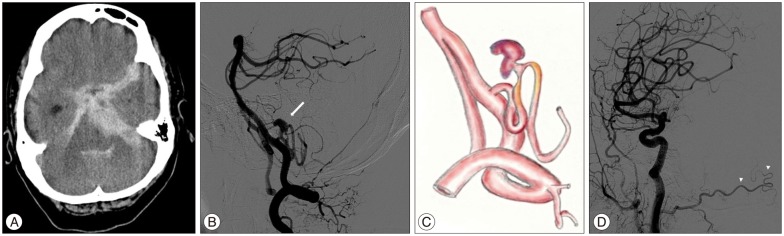
A 74-year-old female patient was admitted to our clinic, presenting with stuporous mentality and vomiting. A computed tomography (CT) scan showed a subarachnoid hemorrhage, primarily in the posterior fossa cisterna, combined with an intraventricular hemorrhage. On conventional angiography, the left PICA ran in an unusual pattern, forming S-shaped dual loops at the lateral medullary segment. Irregular-shaped bulging with proximal stenosis suggesting a dissecting aneurysm was also seen at the cranial loop (Fig. 1).
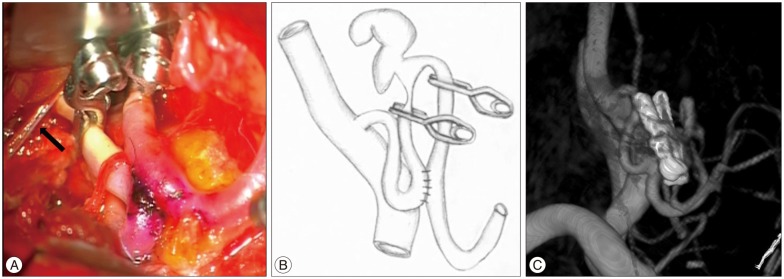
Our primary plan was trapping and revascularization. Because her ipsilateral occipital artery (OA) was not long enough to be a bypass donor, we had prepared to harvest of radial artery graft. The surgery was performed by (blinded for review). After dissection of the OA stump for the bypass, a suboccipital craniectomy was conducted by a far-lateral transcondylar approach. We identified the aneurysm and whitish discoloration at its proximal segment, which suggested the stenosis, seen as a "string sign" in angiography. However, a direct approach to the aneurysm was limited because it was located behind the lower cranial nerve rootlets. On examining the operative field, the idea of an intersegmental anastomosis between the proximal and distal caudal loop of one artery was suggested, because the two segments were sufficiently redundant to be approximated. Methodologically, a side-to-side anastomosis was thought to be more appropriate than an end-to-end procedure because several medullary perforators were identified at the distal portion of the site to be revascularized. Following both proximal and distal trapping of the dissected segment, a conventional side-to-side bypass was performed after temporary clipping, with 10-0 blue nylon. The procedure resembled the bridging or closing of an "omega" (Ōä”) (Fig. 2).
The postoperative course of the patient was uneventful. Follow-up angiography on the first postoperative day showed intact patency of the anastomosis with complete obliteration of the dissection. Later CT follow-up at the 14th postoperative day did not suggest infarction of the medulla or cerebellum. The Glasgow outcome scale score was '3' when the patient was discharged, an improvement from the status at admission.
DISCUSSION
A PICA dissecting aneurysm is an extremely rare condition. Because they usually appear combined with a vertebral artery dissection and the isolated form is much rarer, only a few cases have ever been reported18). The etiology of this rare condition remains unknown, although underlying hypertension14,20) and trauma8) have been reported as preexisting factors. Others have reported that segmental arteriopathy was considered a reason19,21). However, none of these seemed relevant in this patient.
In most cases of a PICA dissecting aneurysm that caused a SAH, emergency intervention is necessary. However, the surgical approach to this area is challenging because of the risk of injuries to the brain stem or lower cranial nerves1,9). Moreover, PICA is one of the most anatomically variable arteries in terms of its course, supplying a territory including perforators13). Several surgical and endovascular procedures for the treatment of PICA dissecting aneurysms have been described : trapping or proximal occlusion, reconstruction with multiple clips, wrapping with or without revascularization, and remote distal occlusion without bypass12,1516). No single treatment method has been suggested as the gold standard for this rare condition, because each case should be considered individually in terms of the pathological conditions and anatomical relationships5,2122).
Occlusion of the proximal PICA potentially results in two kinds of ischemia in the vascular territories of the perforators and distal segments18). Most perforators from PICA originate from the first three segments of PICA : the anterior medullary, lateral medullary, and tonsillomedullary segment13,21). Because occlusion of these perforators can result in clinically serious lateral medullary infarction, also known as Wallenberg syndrome, revascularization for distal flow is strongly recommended when the proximal PICA is occluded. Occlusion of the distal segment of PICA leads to infarction of the cerebellar tonsils, inferior portions of cerebellar hemisphere, and cerebellar vermis7). Infarction in the vascular territory of distal PICA may generally be tolerable or subclinical because of the potential collateral circulation from the anterior inferior cerebellar and/or superior cerebellar artery2). However, occlusion without revascularization should not be a primary choice unless anastomosis is not possible.
Because in this case the dissecting aneurysm was located in the lateral medullary segment and there were perforators, including a relative large one just distal to the pseudoaneurysm, revascularization was considered essential. There are several methods of revascularization for PICA : direct end-to-end anastomosis of PICA with aneurysm resection12), side-to-side or end-to-side anastomosis with the contralateral PICA11,1617), and anastomosis with OA3,4). However, numerous adjacent perforators, short lengths of mobile and non-dissected segments, a high riding contralateral PICA, and a hypoplastic OA did not permit use of any of the previously reported anastomosis methods. In fact, we had planned to trap the dissected segment and use a distal bypass using an interposed radial artery graft. However, harvest site complications, a size discrepancy, the potential risk of occlusion, and operation time caused us to select a "closing omega" method.
Although it was an unscripted scenario, an in situ canalling anastomosis in this patient was an effective and rational method. To our knowledge, this is the first report of this method for the treatment of a PICA dissecting aneurysm. We consider that the limitations of this method make it appropriate for only a narrow indication. Nonetheless, it is an alternative method for the revascularization of a PICA lesion. Moreover, the method could be useful in similar situations when revascularization is required at other sites.
There are several points to considering regarding the surgical method. The surgeon should detect the medullary perforators as much as possible with a surgical probe, because when perforators are present, as in this case, medullary infarction could develop during temporary clamping for anastomosis. The surgeon in this case made a small arteriotomy at the site of the anastomosis that allowed the clamping time to be shortened. Next, removal of a considerable amount of occipital condyle is essential for a 'good' operative corridor because almost all procedures were performed in the premedullary or lateral medullary cistern.
CONCLUSION
A dissecting aneurysm of PICA is a rare, but potentially fatal, condition. Emergency treatment is required to prevent rebleeding. However, there is no standard treatment method because of the high anatomical variability of PICA. An in situ side-to-side intersegmental anastomosis within a single artery can be an alternative method for revascularization in selected cases.