INTRODUCTION
Spinal cord injury (SCI) with its devastating burden both for the victim and the health care system continues to be a great problem without significant improvement in management. The annual incidence of SCI is estimated as 10-50 cases per million37,40) and there is no established treatment modality on clinical base except for methylprednisolone even though the effect is controversial7,8,9,10,11,12).
Present basic science experiment is designed to demonstrate the effects of a potential pharmacological agent-adalimumab (Humira, Abbott, Abbott Park, IL, USA)-on SCI in rats. Previously we have demonstrated the effects of a tumor necrosis factor-alpha (TNF-╬▒) inhibitor infliximab's (Remicade, Merck&Co, Whitehouse Station, NJ, USA) effects on different experimental models of neuronal injury24,31,32). Adalimumab, human recombinant monoclonal IgG1 antibody specific for cytokine TNF-╬▒, is the third TNF-╬▒ inhibitor approved for inflammatory diseases such as ulcerative colitis after infliximab and etanercept14).
As emerged from the experimental knowledge, injury to neural structures results from two different mechanisms. The first is the primary insult that is resulting from the mechanical event itself and the other is the secondary insult that is resulting mainly from the inflammatory response of the organism's to the primary insult. Neutrophils are blamed for orchestration of secondary injury by releasing various types of enzymes, reactive oxygen species and proinflammatory factors. These factors play important roles in glio-neuronal cell damage1,2,19,25,26,27,30).
MATERIALS AND METHODS
All experiments were approved by our Institutional Review Board and performed in accordance with the local guidelines to minimize animal discomfort.
Thirty two male adult Wistar rats weighing between 250 and 300 g were used in this study. Animals were kept under constant laboratory conditions. After spinal cord trauma, manual emptying of the bladders was performed for the injured animals.
The experimental methodology used in this study was described in detail elsewhere32). Briefly, after the period of habituation, rats were randomly divided into four groups. Induction of anesthesia was performed with proper administration of ketamine hydrochloride (50 mg/kg, Ketalar, Pfizer, Istanbul, Turkey) and xylazine (10 mg/kg, Rompun, Bayer, Istanbul, Turkey). Their midbacks were prepared in a sterile fashion. Using surgical microscope, a midline incision was performed over T5 and T12 vertebrae. A total laminectomy was performed over the segments of T7 and T10 with utmost care preventing SCI. The dura was left intact. Using an aneurysm clip (70 g closing force, Yasargil FE 721, Aesculap, Istanbul, Turkey) compression was applied to the spinal cord at the midpoint of the laminectomy site. The clip was removed after 1 minute of application and the wound is irrigated with normal saline before closure of the layers. Rats in the control group did not receive clip compression procedure. No further treatment was applied to the animals in the trauma group after clip compression. Animals in treatment groups received 5 mg/kg subcutaneous adalimumab and infliximab respectively right after wound closure.
After 72 hours, rats were killed with overdose pentobarbital. Trauma site being at the epicenter, 2 cm length spinal cord segments were removed en block. Tissue samples were immediately stored in a freezer for malondialdehyde (MDA) assay.
Neurological evaluation
Preoperative and postoperative neurological assessments were performed every day until the end of the study by an observer who is blinded to the groups. The Tarlov scoring system was used35). According to this system 5 tier scale was used to evaluate the neurological status : score 0, spastic paraplegia and no movement of the lower limbs; score 1, spastic paraplegia and slight movement of the lower limbs; score 2, good movement of the lower limbs, but inability to stand; score 3, able to stand, but unable to walk normally; score 4, complete recovery and normal gait/hopping.
Determination of lipid peroxidation in traumatized spinal cord tissue
The level of lipid peroxides in traumatized spinal cord tissue were measured as thiobarbituric acid-reactive material and determined using the method of Mihara and Uchiyama34). MDA has been identified as the product of lipid peroxidation that reacts with thiobarbituric acid to give a red species absorbing at 535 nm. The assay procedure for lipid peroxide in spinal cord tissue was set up as follows. Tissues were homogenized in 10 volumes (wt/vol) of cold 1.5% of KCl. One half a milliliter (0.5 mL) of homogenate was mixed with 3 mL of 1% of H3PO4 (Carlo Erba Reagnts, Cat No : 30406, Val de Reuil, France) and 1 mL of 0.6% of thiobarbituric acid (Merck & Co., Cat No : M.108180.0025, White House Station, NJ, USA). The mixture was then heated in boiling water for 60 minutes. After cooling, the color was extracted into 4 mL n-butanol (Sigma-Aldrich, Cat No : 24124, St. Louis, MO, USA), and the absorbance was recorded at 535 and 520 nm with a spectrophotometer (U-2900, Hitachi High Tech, Tokyo, Japan). Using tetramethoxypropane as the standard, tissue lipid peroxide levels were calculated as nanomoles per gram of wet tissue32).
Statistical analyzes
Commercially available software package SPSS (SPSS Inc., Released 2007, SPSS for windows, version 16.0., Chicago, IL, USA) was used to compare MDA levels between groups. Results are expressed as mean values and probability level less than 0.05 was accepted as significant. Nonparametric tests of Kruskal-Wallis and Mann-Whitney U were used to determine differences between groups regarding mean MDA levels.
RESULTS
Lipid peroxidation
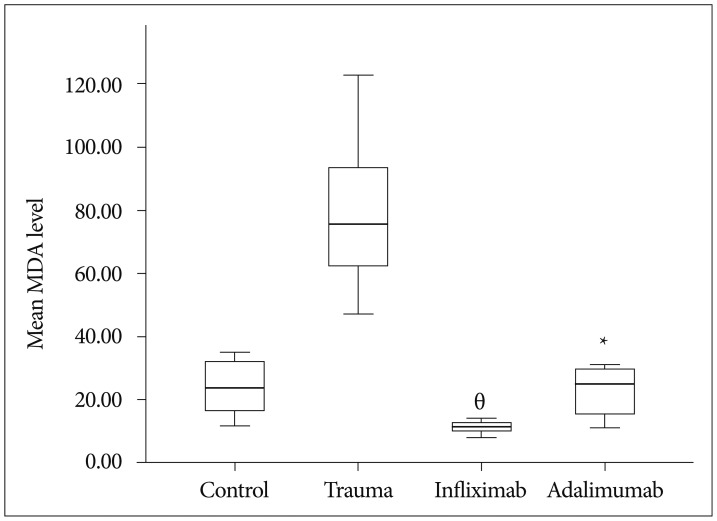
The mean MDA level of the control group was 23.87┬▒8.96 (range : 12.00-35.00), trauma group was 79.12┬▒24.19 (range : 47.00-123.00), infliximab group was 11.25┬▒1.90 (range : 8.00-14.00) and adalimumab group was 22.75┬▒8.10 (range : 11.00-31.00). MDA levels was statistically significantly different between groups, Žć2(3)=23.063, p <0.01. Pairwise comparisons were performed using Dunn's procedure with a Bonferroni correction for multiple comparisons. MDA levels were significantly different between the trauma and infliximab groups (p <0.01) and trauma and adalimumab groups (p=0.022). Boxplot in Fig. 1 demonstrate mean MDA levels of groups.
Neurological evaluation
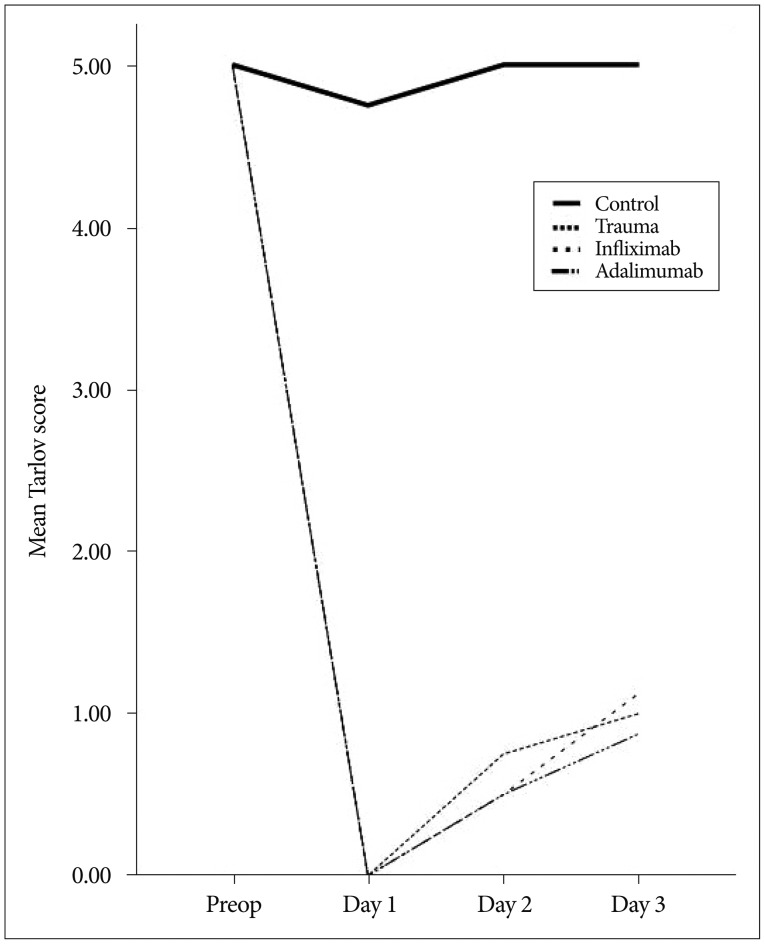
Line chart in Fig. 2 demonstrates mean Tarlov score changes throughout the experiment. There was no significant difference between trauma and treatment groups regarding Tarlov score.
DISCUSSION
Traumatic injury to the spinal cord itself creates an injury site within traumatic tissue. This is the primary injury and apart from preventive measures aimed to prevent accidents, there is virtually nothing that can be done in terms of treatment for now. On the other hand, secondary injury resulting from the changes in the trauma milieu is the main target of research33). Secondary injury results from cascades of ischemia, edema, excitatory amino acid influx and oxidative injury4,16).
Central nervous system is considered as a relatively "immune free" environment in normal circumstances. After an insult, this changes6,16) and it was demonstrated that reducing or blocking inflammatory response may have beneficial effects6,10,21,31).
Oxidative stress occurring after trauma injures nucleic acids, proteins, carbohydrates and lipids17). Since biological membranes constitute of lipids, lipid peroxidation targets them17,22). The lipid rich environment of nervous tissue makes it susceptible to such injuries. MDA is a three carbon, low molecular weight aldehyde which is considered as an important lipid peroxidation marker. Levels of MDA increases in several diseases22,31) and SCI20,24,32).
TNF-╬▒ which is a proinflammatory cytokine produced by monocytes, macrophages and T lymphocytes was proven to play important roles in various diseases such as rheumatoid arthritis, psoriatic arthritis, Crohn's disease, psoriasis and ankylosing spondylitis13,29). Blockage of TNF-╬▒ causes immune system suppression18) and this effect is used to treat aforementioned diseases13,14,18,29,36). Besides its roles in such diseases TNF-╬▒ has demonstrated roles in neural tissue damage and neuroinflammation5,23,38,39). Harrington et al.28) have demonstrated an increase in TNF-╬▒ levels in cerebrospinal fluid in the first hour of SCI. Wang et al.39) had similar findings in traumatized spinal cord tissue. Authors of these studies concluded that TNF-╬▒ has important roles in pathophysiology of traumatic SCI.
Etanercept, infliximab, adalimumab, golimumab, and certolizumab are the anti-TNF-╬▒ agents that are authorized for treatment of diseases mediated by TNF-╬▒15). Only infliximab32) and etanercept3) has been evaluated in SCI and their favorable effects have been demonstrated. This is the first study evaluating the effects of adalimumab on SCI. The study is built on the hypothesis that TNF-╬▒ blockage by adalimumab may have beneficial effects in SCI as demonstrated in previous studies of different agents targeting TNF-╬▒. Results here have showed that adalimumab has favorable effects on lipid peroxidation in spinal cord injured rats. The decrease in MDA levels was significant when compared to controls; however, there were no significant difference between adalimumab and infliximab. This suggests, these two agents have similar effects on lipid peroxidation levels in experimental SCI. On the other hand we could not demonstrate any favorable effect in neurological status. This may be the result of 72 hours of evaluation. This study is primarily designed to demonstrate biochemical effects of the agents on SCI and longer periods may reveal differences.