EPIDEMIOLOGY
Spinal column and/or spinal cord trauma patients can present within full spectrum from mild to disabling injury, and even death. According to the numerous data from foreign references, of which the majority from USA, pediatric spine trauma is infrequent, known to be only about 2% to 5% of all spinal injuries [13], and 60% to 80% of them involves cervical spine largely due to the anatomy and biomechanics of those specific age group [81]. Pediatric thoracolumbar spine fractures mainly occur during adolescent age of 14 to 16 [14]. The predominant mechanism of injury for younger children (0 to 9 years of age) is falls and pedestrian-to-automobile accidents, whereas for older children (10 to 18 years of age) automobile accidents prevail [88]. Child abuse is another noteworthy cause of pediatric spine injury, as cases are expected to increase and initial active involvement is crucial. Korean Statistical Information Service reports that child abuse cases are escalating yearly, and its detailed national report on year 2017 revealed that 2.64% of whole pediatric population was reported to be abused, with physical abuse involvement accounts for almost 40% of all cases [54]. Several USA studies showed that child abuse account for less than 1% of all pediatric spine injuries [44], and skeletal survey for suspected child abuse revealed that about 10% of them had spinal fractures [5]. Regarding spinal cord injury (SCI), neonatal patients are associated with obstetrical manipulation, with the incidence of one in 80000 live births [81], and there is a bimodal peak age group for young adults and adolescents as a first peak and geriatrics as a second peak, with the rough incidence of 115 and 800 per 1 million, respectively [44,45,92].
PEDIATRIC SPINE ANATOMY, BIOMECHANICS, AND DEVELOPMENT
Children have unique spinal anatomy and biomechanics that contributes to various features of pediatric spine trauma. One neonatal cadaver study revealed that neonatal vertebral column can stretch as much as 2 inches without disruption, but the spinal cord can only stretch 0.25 inches [59]. This bony column flexibility stems from inherently flexible and elastic pediatric spinal ligaments and joints.
Specifically, facet joints are smaller, more horizontally oriented and shallower than adults which allow for more translation during spine movement with less stability. Absent uncinate process until age of 10 adds additional mobility to the cervical spine as this structure limits lateral and rotational movements. Spinal ligaments and joint capsules are able to stretch without disruption of tissue due to the higher water content. These biomechanics combined with the relatively stiff spinal cord accounts for higher rates of SCI without radiographic abnormality (SCIWORA) of all pediatric spine injuries compared with adults reported in multiple studies [6,30,88].
Another important feature for children under age 8 is that their head is relatively heavy and large compared with their body. This high head-to-torso ratio makes neck in relatively flexed position compared to adults [96] with the fulcrum of flexion at C2-C3 in infants, C3-C4 by age 5, C4-C5 at age 10, and C5-C6 by age 15 [9,52]. These features account for the finding that upper cervical injury predominates for children under the age 8 [70].
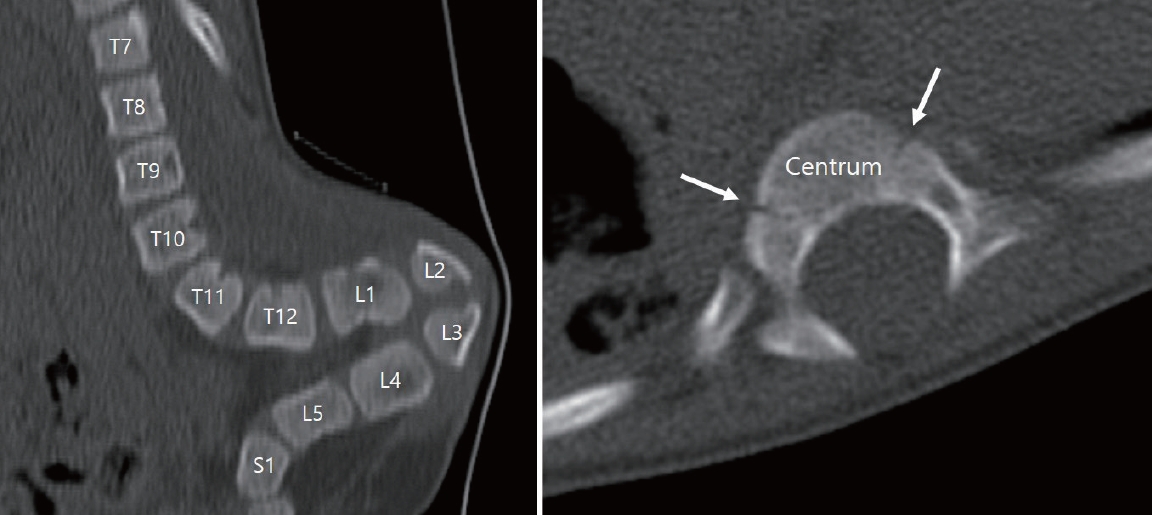
Ossification process is an important part of pediatric spinal development which affects trauma pattern and radiographic findings. One noticeable finding is the neurocentral junction (NCJ), which is the synchondroses between developing vertebral body (centrum) and vertebral arch (Fig. 1), subsequently begins to fuse at the age 3-6, becoming the physeal scar in adult spine [64]. Surgical implication of NCJ is that as a persistent plate of bone inside every vertebral body throughout life, it is recommendable to be traversed when inserting pedicle screw to get additional support and avoid loosening [64]. Other relevant pediatric spine features are as follows. Initially cartilaginous C1 body at birth is radiographically not visible until the age 1, spinous processesŌĆÖ synchondroses at midline fuses at age 3. At the age of 3-6 years, NCJ and synchondrosis between odontoid and body of C2 fuse, with ossification center appearing at the tip of the odontoid, and the anterior wedging of vertebral bodies resolve. Upper cervical spine pseudosubluxation and widening of predental space resolves by age 8. At puberty, superior and inferior epiphyseal rings together with secondary ossification centers at the tip of spinous processes appear and summit ossification center of odontoid fuses. Secondary ossification centers fuse roughly by the age 25.
Epiphyseal injury should be always kept in mind as consequent premature epiphyseal fusion can lead to deformity and affect growth, which is difficult to detect initially from plain radiograph. SharpeyŌĆÖs fibers exist at the periphery of annulus fibrosus and insert into adjacent superior and inferior epiphyseal rings. The strength of this fiber exceeds that of attachment of epiphyseal rings and vertebrae, and this accounts for the detachment of epiphyseal rings from vertebrae with shearing force [52].
PEDIATRIC CERVICAL SPINE TRAUMA
Cervical spine injury comprises most of the pediatric spine injury which makes the categorical review invaluable. Younger children below age 10 have relatively heavy head and are subject to high-velocity pedestrian accident, which makes them vulnerable to craniovertebral junction (CVJ) injuries, which are classified and reviewed in detail. Conversely, older children have spinal injury pattern similar to adults mostly at subaxial spine with less involvement of CVJ. The Congress of Neurological Surgeons have published a guideline for imaging surveillance for pediatric trauma patients to clear cervical spine [85]. It suggests cervical spine anteroposterior and lateral X-rays or high-resolution computed tomography (CT) to pediatric trauma patients with difficulty in communication, neurologic deficit, neck pain, distracting pain, intoxication, or high energy injury mechanism. In addition, open-mouth view is not recommended for children under age 9, and CT over X-ray is recommended for suspected atlantooccipital dislocation (AOD). Algorithm provided by Pediatric Cervical Spine Clearance Working Group is similar to some extent, utilizing Glasgow coma scale, trauma history, and physical exam findings for the decision to carry out surveillance X-ray or CT [39].
CVJ injuries
CVJ is the most mobile segment of spine which consists of occiput, atlas, and axis. Grossly 2 segments comprise CVJ : atlantooccipital segment and atlantoaxial segment. Each segment has its own ligaments which stabilize and allow specific motion. And several extrinsic ligaments that are not specific to CVJ but contiguous to the other parts of spine function as stabilizers. The atlanto-occipital segment allows 23┬░ to 24.5┬░ of flexion/extension and 3.4┬░ to 5.5┬░ lateral bending of the cranium. Among cervical spinal rotational capacity of 90┬░, atlantoaxial segment contributes the most (25┬░ to 30┬░), with flexion/extension capacity of 10.1┬░ to 22.4┬░ [77]. Supraphysiological motion or excess force applied to CVJ can cause various types of injuries.
AOD
Although rare, younger children below age 10 are vulnerable to this type of injury due to relatively heavy head and smaller, horizontally oriented atlantooccipital joints [52] which makes CVJ vulnerable to shearing forces. Fatal AOD cases are found to have widespread ligamentous disruption, especially alar ligament and tectorial membrane [2]. Clinical presentation is variable, including neck pain, low cranial nerve deficit, extremity weakness, and even death [36]. Radiographic diagnostic criteria is not clearly defined for AOD, as none of the single available method is perfect [50]. The Traynelis classification divides AOD into three groups [95] : anterior displacement is type I, axial distraction is type II, posterior displacement is type III, but this method overlooks coronal malalignment [36]. PowersŌĆÖ ratio measured at the midsagittal plane compares distance from basion to anterior cortex of posterior arch of atlas with distance from opisthion to posterior cortex of anterior arch of atlas [82]. Normal value is less than 0.9, with higher values represent type I AOD, but is less sensitive for type II or III AODs. The X-line method, which is more sensitive than powersŌĆÖ ratio in detecting Traynelis type II and III AODs, draws two lines at midsagittal plane and assess anatomical relationship of CVJ [57]. Measuring basion-dens interval and basion-axis interval is the other way to detect AOD, and Harris method utilizes these two measurements collectively [37,38]. Lastly, occipital condyleC1 interval measurement is specific for Traynelis type II injuries, and is validated in pediatric population. As above, AOD presents clinically and radiographically diverse which makes clinicianŌĆÖs high index of suspicion important for diagnosis and prevention of secondary injury. Prompt cervical immobilization, hemodynamic management and early aggressive surgical stabilization is crucial for better outcome. Traction is generally avoided due to the risk of neurological deterioration [94]. Halo fixation use is declining these days due to its ineffectiveness in immobilization and potential for morbidity [80], combined with the AODŌĆÖs lack of ability for spontaneous healing [35]. Posterior fixation is more useful for AOD than anterior fixation to achieve surgical treatment with O/C1, O-C2, or O-C2 without C1 fusion. Former wiring techniques are mostly replaced with various screw fixation techniques including transarticular, lateral mass, C2 pedicle, or laminar screws [36].
Atlantoaxial rotatory subluxation (AARS)
The atlantoaxial joint is mainly stabilized by transverse ligament and alar ligaments and has harmonious biomechanical relationship during rotatory movement [74]. Transverse ligament limits excessive anterior translation of atlas on axis, and alar ligaments limit excessive rotation of atlas. Injury of these ligaments due to various mechanisms lead to atlantoaxial joint instability. Atlantoaxial rotatory displacement (AARD), AARS, and atlantoaxial rotatory fixation (AARF) are terms used to describe a spectrum of atlantoaxial joint rotational abnormality [7,74-76]. Sometimes the terms AARD, AARS, and AARF are intermixed, and torticollis is mistakenly regarded as same as AARD, despite being a separate entity [33]. For the umbrella term for three spectrums of condition, AARS is used in this article. There are various pathologies (infection, head/cervical operation, major/minor trauma, genetic disease) associated with AARS, but culprit biomechanical cause of fixation, or locking of the atlantoaxial joint followed by subluxation/dislocation is not fully understood [33]. AARS clinically presents with neck pain and discomfort, limited rotation, typically cock-robin deformity with neck rotated in one direction and tilted in the opposite direction, and rarely neurologic symptoms. Diagnosis is difficult to attain radiographically as simple radiography is not fully diagnostic, and even standard or dynamic CT can be misleading [72]. Due to the inability to retain neutral head position, bony relationships are obscured by soft tissue in plain radiograph. Although CT is a valuable tool to investigate static joint relationship of atlas and axis, it does not represent dynamic relationship. For this reason, some advocate the use of dynamic CT, but there are also concerns about the reproducibility and its diagnostic value [73,75]. Magnetic resonance imaging (MRI) can reveal joint capsule or ligamentous edema, surrounding soft tissue pathology or cord injury, but has little implication in treatment decision so far. Therefore, diagnosis of AARS is primary a clinical one, aided by multiple imaging modalities. Torticollis and AARD can be distinguished by the side of the sternomastoid spasm, as torticollis shows contralateral spasm relative to the side of the chin, but AARD shows the opposite. Fielding and Hawkins presented classification of AARF based on the degree and direction of displacement of atlas, utilizing static CT with head position as initial presentation [31]. Various treatment algorithms are presented in literatures with no consensus. As AARS is a clinical diagnosis, some patients will fall into diagnostic grey zone, and they are treated conservatively with/without collar/brace [76]. Many studies classify patients as acute, chronic, and congenital based on the duration of symptom for treatment modality decision purpose, but the cut-off point for acute/chronic is variable. Acute AARS is generally considered benign, treated with less invasive closed reduction such as halter traction, followed by external immobilization or immobilization alone with good clinical outcome [66,69]. Persistent acute AARS cases together with chronic/congenital cases require either longer/repeated closed reduction, or more invasive traction devices such as Gardner-Wells-style tongs or halo vest but there is no consensus upon traction and stabilization period, the number of attempts before considered irreducible, and the type of traction device of choice [66,69,73,75]. Generally, irreducible cases require operative stabilization for C1/C2.
Translational atlantoaxial subluxation (TAAS)
Translation of atlantoaxial joint is limited by intact odontoid process, C1/2 joint capsule and disc, and associated ligaments [83]. Violent trauma, hyperextension, or distraction injury can cause traumatic TAAS [52,67,82]. Nontraumatic cases can also arise from inflammation, facet tropism, spinal tumors, or congenital disorders including spinal fusion, Down syndrome and skeletal dysplasias [1,52,62,86]. Clinical presentation is diverse, from minor neck pain to myelopathy due to cord compression or cerebellar/occipital lobe infarction due to vertebral artery stenosis [8,32,89]. Compared with AARS, radiographic diagnosis of TAAS is relatively straightforward as slippage of atlantoaxial facet is easily identified from coronal/sagittal plane of CT image, with several proposed classification systems for translational subluxation itself or transverse ligament injury [23,61,63]. Noninvasive immobilization can be attempted, but extensive ligamentous injury or neurologic complication is an indication for C1/2 fusion operation [52].
CVJ fractures
Occipital condyle fracture (OCF), although being rare, should be considered when evaluating high impact head trauma patient, including automobile and sports accidents. Associated injuries including intra and extra-axial lesions need to be investigated due to the nature of the mechanism of injury. Neurologically, the patient can present from normal finding to brainstem, cord, or cranial nerve deficit. Neurologic instability comes from direct neural compression by avulsion of the fractured segment, or cord contusion without bony fragment displacement [15]. Radiographically, OCF is difficult to detect from plain film, so thin section CT is recommended for diagnosis. Some suspect that OCF is underdiagnosed due to the difficulty of diagnosis [15,22]. OCF might cause instability of CVJ due to the attached ligaments at occipital condyle, especially when the alar ligaments are coaffected [4]. The general principle of OCF management is conservative with stable CVJ, and occipitocervical fusion with CVJ instability [71].
Pediatric atlas fracture is rarely reported with consistent mechanism of injury of fall from vertex or automobile accident. It is important to note lateral pseudospread, a normal variant of atlas due to the initial fast growth than axis, and three synchondroses which can be confused with true fractures. For isolated atlas fracture, conservative treatment is reported to be sufficient with full functional recovery [46].
Younger children has odontoid fractures at neurocentral synchondrosis which is known to fuse by age 5 to 7, and older children has true adult type odontoid fractures [52]. Most of the patients will not experience neurologic deficits. Resultant widening of odontoid epiphysis can be visualized by CT or MRI. Conservative management is considered without marked displacement of odontoid process and is applicable to most of the cases [29,68]. Operative osteosynthesis of dens is achieved through various techniques, and the gradual posterior angulation of dens through aging and its transverse dimension should be considered with odontoid screw fixation technique [93].
Pediatric axis body and ring fracture including hangmanŌĆÖs fracture is rarely reported as a result of child abuse or high energy trauma [51,84]. AxisŌĆÖs neurocentral or dens-arch synchondrosis should not be mistaken as fracture, but fracture through this synchondrosis is also reported. It is common to classify axis ring fracture by the system described by Effendi et al. [27] and modified by Levine and Edwards based on the degree of displacement and stability which provides clinically reasonable guideline for management. For type I or II fractures without neurologic deficit, conservative treatment with immobilization is generally sufficient for excellent bony union, but surgical treatment should be considered for LevineEdwards type IIa or III fractures with significant dislocation and possibility of later instability [17,34,60]. Axis body fractures are uncommon and mostly stable, but burst fracture with associated vertebral artery injury should not be missed [26].
Subaxial cervical spine injuries
Subaxial spinal injury refers to fracture, dislocation, or ligamentous injury of C3 to C7. Most common mechanism of injury is motor vehicle accidents, followed by sports injury and fall. Subaxial cervical spine injury mostly occurs between age 9 to 16 which reflects the fulcrum of cervical motion at C5-C6 for adolescents [9,25]. For children under the age 9, pure ligamentous injury with SCI is more common, whereas bony injuries are more common for older children [65]. The most important determinant of treatment depends on neurologic status and stability of the injury, and imaging plays a key role for the evaluation [25,70]. The decision whether to initiate cervical spine imaging for pediatric patients following blunt trauma can be aided by National Emergency X-Radiography Utilization Study tandard criteria [40,99], bearing in mind that only 2.8% of the most difficult-to-assess group of age under 2 are included in the study [16], and that the usefulness of this criteria for pediatric population is being debated [28,90]. Static plain radiographs of antero-posterior and lateral views are generally used with the advantage of less radiation exposure to the patient. Plain film with dynamic flexion and extension views are used to investigate instability although it may be unsatisfactory initially due to the muscle spasm or the need for immediate immobilization. For children under the age 8, angulation greater than 7┬░ or subluxation greater than 4.5 mm is generally considered unstable [70], which is the modification of the criteria by White and colleagues suited for adult population [101]. Supine CT can provide little information regarding stability, but still useful for bony anatomy and surgical planning. MRI is superior in revealing soft tissue, ligamentous, disc, or spinal cord injury. DenisŌĆÖs three column model, originally developed for thoracolumbar injury [21], is also widely used to assess cervical spine stability [10,16], and Subaxial Cervical Spine Injury Classification (SLIC) system encompass treatment strategy with prognosis [53,79,97,98]. Generally, stable injuries are managed conservatively, and surgical intervention is considered for mechanically or neurologically unstable injuries with shortest construct as possible to avoid compromising spinal column growth [65]. Future cervical deformity would require surgical treatment based on the degree of malalignment, as cervical spine is in a dynamic relationship with whole spine which can influence global spinal balance [47,58]. Those who have objective finding of myelopathy from trauma, with negative plain radiographs, CT, and MRI are classified as SCIWORA, although some argue that this diagnosis can be made with cord signal change on MRI [16,52]. Most investigators advocate conservative treatment of cervical orthosis for up to 12 weeks followed by examining for late instability for SCIWORA [52,53,65]. And it is noteworthy that some consider the term SCIWORA a misnomer especially for adult population because they actually have baseline degenerative changes [88]. Instead, the terms SCI without CT evidence of trauma (SCIWOCTET) or SCI without radiographic evidence of trauma (SCIWORET) are being advocated and used in literature as much as the traditional term, SCIWORA.
PEDIATRIC THORACOLUMBAR SPINE TRAUMA
Majority of pediatric thoracolumbar spine injury occur during adolescence age with male predominance, mostly by sport activities or motor vehicle accidents [14,24]. Among all injury mechanisms, unrestrained motor vehicle accident is the culprit for more than half of SCI for all pediatric age groups [11,100]. Injury types can be subdivided into compression fracture, burst fracture, fatigue fracture of pars interarticularis, seat belt fracture, slipped vertebral apophysis, shear injury, crushing injury, and SCIWORA. Stability of the spine and neurologic deficit are the most important part of assessment. Even mechanically stable injury can elicit neurologic deficit which warrants decompression or fusion operation. Specifically, shear injury is a form of fracture-dislocation type injury with instability at all three columns, and it should be kept in mind that burst fracture and slipped vertebral apophysis can damage germinative layer and lead to premature epiphyseal fusion. AOSpine thoracolumbar spine injury classification, DenisŌĆÖs three column model and thoracolumbar injury classification and severity score (TLICS) are all widely used for classification and treatment decision for pediatric population [3,18,19,87]. Neurologically and mechanically stable thoracolumbar injuries can be treated conservatively with immobilization via orthosis. Besides, most neurologically intact burst fractures and potentially unstable injuries can also be treated nonoperatively with orthosis and bed rest [91]. The prognosis of SCIWORA depends on initial neurologic presentation and are usually treated conservatively [56,91]. And it should be noted that children with further growth potential can develop chronic instability and subsequent deformity from spinal injuries, which may require surgery [20,55]. In such cases, intuition from previous experience and research can be helpful. For spinal deformity surgery, global and regional alignment are important considerations for surgical planning [47-49,58]. Detailed decision including surgical approach, deformity correction technique, upper/lowest instrumented level, and adjunct material to use all matters and impacts clinicoradiological outcome [12,41-43,78,102].