INTRODUCTION
Anterior cervical corpectomy and reconstruction comprise a treatment for cervical spondylotic myelopathy (CSM) or an ossified posterior longitudinal ligament (OPLL) [5,10,21,23]. An anterior plate was first applied to overcome the high reoperation rate and symptomatic pseudarthrosis associated with anterior cervical corpectomy and reconstruction using iliac bone grafts [6]. This practice was followed even when a titanium mesh cage (TMC) graft was used instead of iliac bone. Many institutions currently use TMCs with anterior plate augmentation as a reconstructive method [7,10,12,21,23]. Many studies have addressed the advantages of anterior cervical plate fixation, such as improved stability, improved fusion percentages, decreased duration of fusion, prevention of graft migration, maintenance of intervertebral height, and a shorter duration of brace use [2,20], whereas other studies have reported that the anterior plate is not as effective as expected [1,2,6]. Epstein [6] compared single-level anterior cervical corpectomy and fusion performed with and without plates and found that plating did not reduce pseudarthrosis or the graft extrusion rate. Al-Mashani et al. [1] suggested that an anterior plate does not lead to a better result. Benzel and Francis [2] reported that anterior plating required additional soft tissue retraction, which led to a longer operating time. Without a firm screw-bone interface, the anterior plate can still be dislodged from the vertebral body and may cause mechanical problems [15], even if the plate has a screw-locking system. We hypothesized that an additional plate is not crucial to cervical stability. We devised a novel reconstruction method using a TMC with f langes instead of an additional anterior plate for fixation. This new method has not been reported before. This study was designed to investigate clinical and radiographic outcomes of anterior corpectomy and reconstruction using a flanged TMC instead of an anterior plate for CSM and OPLL. We also evaluated whether this method could be an alternative option for cervical reconstruction.
MATERIALS AND METHODS
Patient population
This retrospective study enrolled 50 patients with CSM or OPLL between January 2012 and January 2018 at a single institution. All patients underwent single- or two-level anterior corpectomy and reconstruction using a flanged TMC. Include criteria were patients presented with both clinical and radiographic evidence of CSM or OPLL and were refractory to conservative treatment. Exclude criteria included previous cervical spine surgery, cervical spine trauma, active infection and neoplasm. Information about patients, surgery, and associated perioperative complication were obtained from medical records. This study was approved by Soonchunhyang University Bucheon Hospital Institutial Review Board (IRB No. 2019-01-006-001).
Surgical procedures
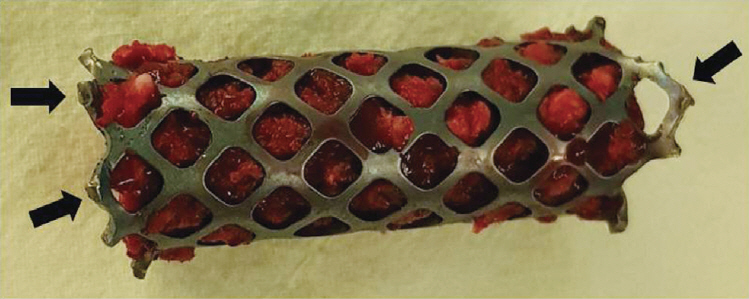
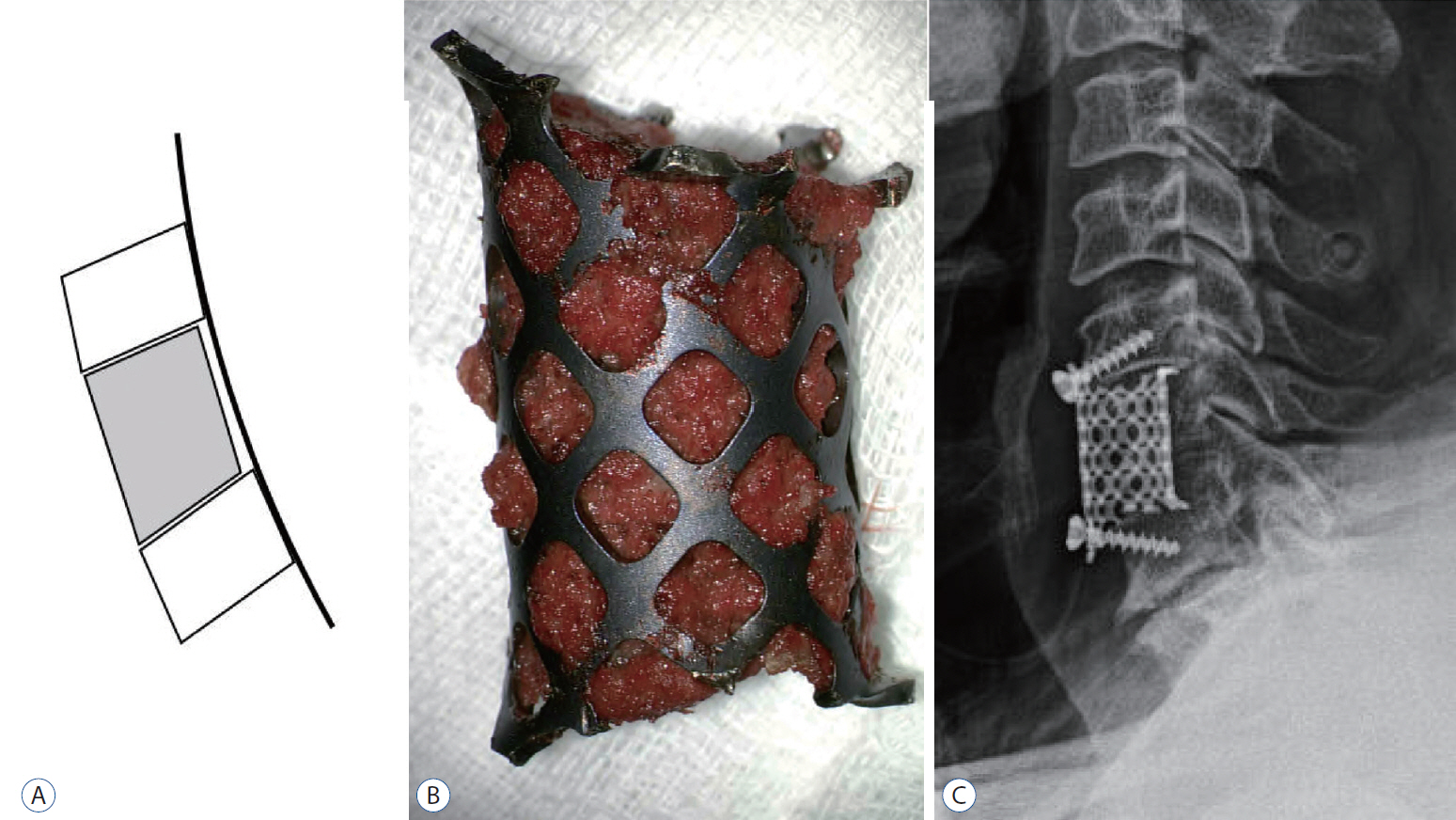
A 15-mm SynMesh cage (DePuy Synthes, Zuchwil, Switzerland) was used for reconstruction. Corpectomy and decompression were performed using standard methods. We trimmed the edge of the TMC to the appropriate height with cutters and tailored it to have small flanges in the uppermost and lowermost parts of the midline. The both end of TMC was bend outward like sunflower to increase the surface area. All cages were filled with autologous bone harvested at the local corpectomy site (Fig. 1). No TMC endcaps were used. The TMC was positioned on the anterior-most part of the vertebral body adjacent to the cortical rim and fixed with one or two screws in the flanges. All cases were operated on by the same surgeon. The patients were instructed to wear a soft collar for 4 to 6 weeks postoperatively.
Clinical assessment
We used Odom’s criteria (Table 1) and divided the patients into four categories of excellent, good, fair, and poor based on improvement of their preoperative symptoms and ability to carry out daily activities. We also investigated surgery-related complications, including neurological deficit, cerebrospinal fluid (CSF) leakage, dysphasia, hoarseness, neck pain, and hardware complications such as screw breakage or loosening.
Radiological assessment
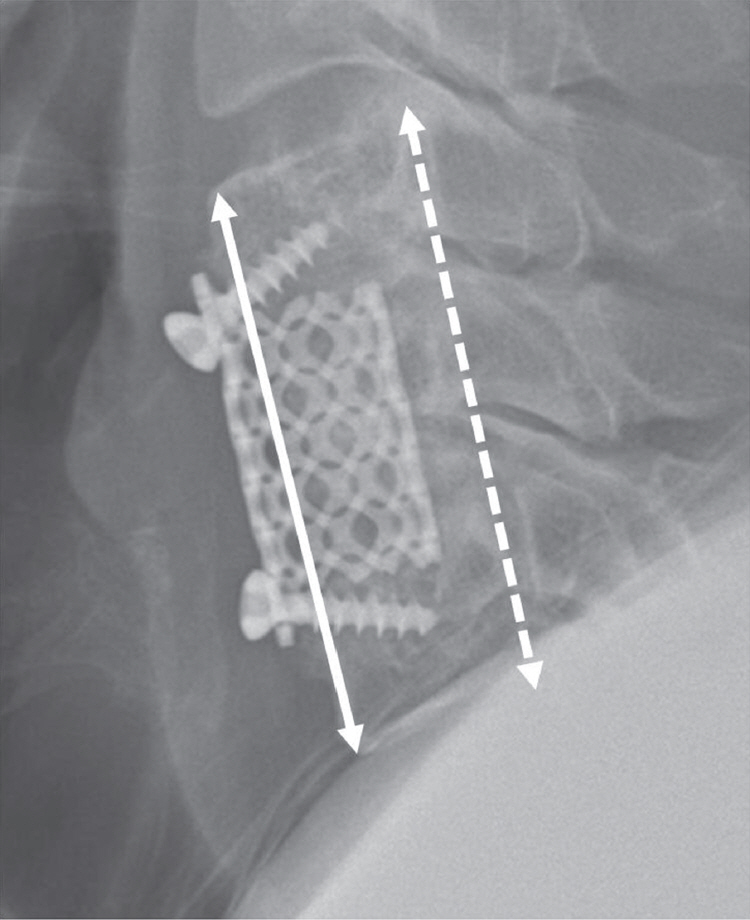
All patients were assessed via plain anteroposterior (AP), lateral, and flexion-extension X-rays preoperatively, plain X-rays and computed tomography (CT) during the immediate postoperative period and subsequent repeated radiological follow-up at regular intervals. Anterior and posterior interbody height (AIBH and PIBH) were assessed from plain lateral radiographs (Fig. 2). The AIBH is the length between the anterior portions of the adjacent upper and lower endplates, and the PIBH is the length between the posterior portions of the adjacent upper and lower endplates. Mean interbody height (MIBH) was defined as the average of AIBH and PIBH. We used postoperative CT in cases involving a lower cervical segment or when the segment could not be seen on a plain radiograph. Subsidence was defined as the difference between the postoperative and final follow-up values. Patients with ≥3 mm of change were classified as the severe subsidence group [4].
Successful fusion was defined as radiological cross-trabeculation in the plain AP and lateral views or in CT by a lack of segmental movement in the flexion-extension views, and no radiolucent gap around the implanted cage [16].
Statistical analyses
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Quantitative data are presented as mean±standard deviation. The level of significance was set at p<0.05. The paired t-test, one-way analysis of variance, and Pearson’s correlation analyses were used.
RESULTS
Demographic characteristics
The demographic characteristics are shown in Table 2. This study included 50 patients (35 females and 15 males; mean age, 59.6 years). The mean follow-up period was 16.8 months. Pathologies included OPLL (n=24) and CSM (n=26). Thirty-eight (76%) patients received a single-level corpectomy and 12 (24%) received a two-level corpectomy.
Clinical outcomes
Most of the patients showed improved neurological symptoms. At the last follow-up, 19 patients (38%) were classified as excellent, 25 (50%) as good, four (8%) as fair, and two (4%) as poor based on Odom’s criteria. Surgery-related complications included two patients with C5 palsy, two with CSF leakage, three with hoarseness, and three with dysphasia. The patients with C5 palsy underwent revision surgery, and the symptom was resolved. The two patients with CSF leakage were successfully treated with bed rest and antibiotics. The hoarseness and dysphasia were temporary, and no patients showed hoarseness or dysphasia at the last follow up. No infections, epidural hematomas, or visceral injuries were observed during the follow-up period. The most common hardware complication was screw breakage (n=8), which occurred mainly in the early period, followed by screw loosening (n=6). No cage extrusions occurred (Table 3).
Radiological outcomes
Table 4 summarizes the radiological outcomes of the 50 patients. The mean extent of the corpectomy was 1.24. The overall fusion rate was 98% and no pseudoarthrosis according to the last follow-up X-rays. One case required reinforced reconstruction with an anterior plate because subsidence progressed and C5 palsy occurred. The average MIBH was 56.8±10.8 mm immediately after surgery and 54.0±10.3 mm at the last follow up. Subsidence of MIBH was 2.8±2.4. The subsidence rate was 34% (n=17) at the last follow up.
Relationship between subsidence and Odom’s criteria, age, follow-up period, and corpectomy level
Correlation analyses were performed to investigate the relationship between MIBH subsidence and Odom’s criteria, age, follow-up period, and corpectomy level. Subsidence tended to be larger in the poor Odom’s criteria group than in the excellent and good groups (p=0.381) (Table 5). No correlations were observed between subsidence and age or follow-up period (Table 5). The mean subsidence of patients who underwent a two-level corpectomy was 3.9±3.0 mm, which tended to be greater than that of patients who underwent a single-level corpectomy (2.4±2.1 mm; p=0.127) (Table 5).
Illustrative cases
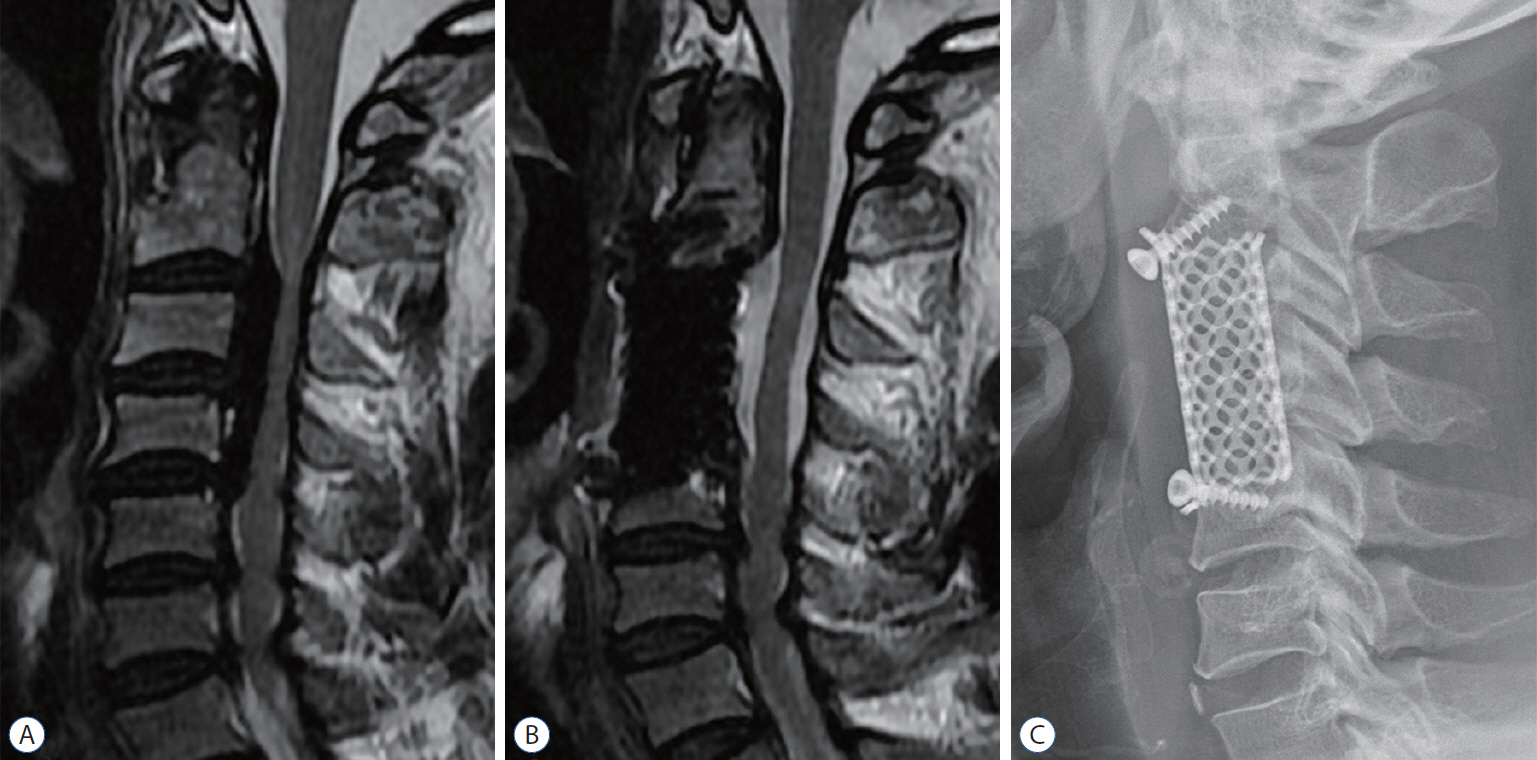
A 64-year-old man complained of hand and leg tingling sensation on both sides for 2 year and symptoms got worse overtime. Both hands grasping power started weakened from 1 month ago. A cervical magnetic resonance imaging (MRI) showed at C3-C7 with spinal canal stenosis in C3-5 compressing spinal cord. We performed a C2/3 and C5/6 discectomy, C3 and C4 corpectomy and decompression OPLL at C3-C4. His symptoms improved to “good” after surgery based on Odom’s criteria. The patient did not complain of any complications at 6 months after operation, and cord compression was resolved, and bone fusion occur on follow-up MRI and X-ray (Fig. 3).
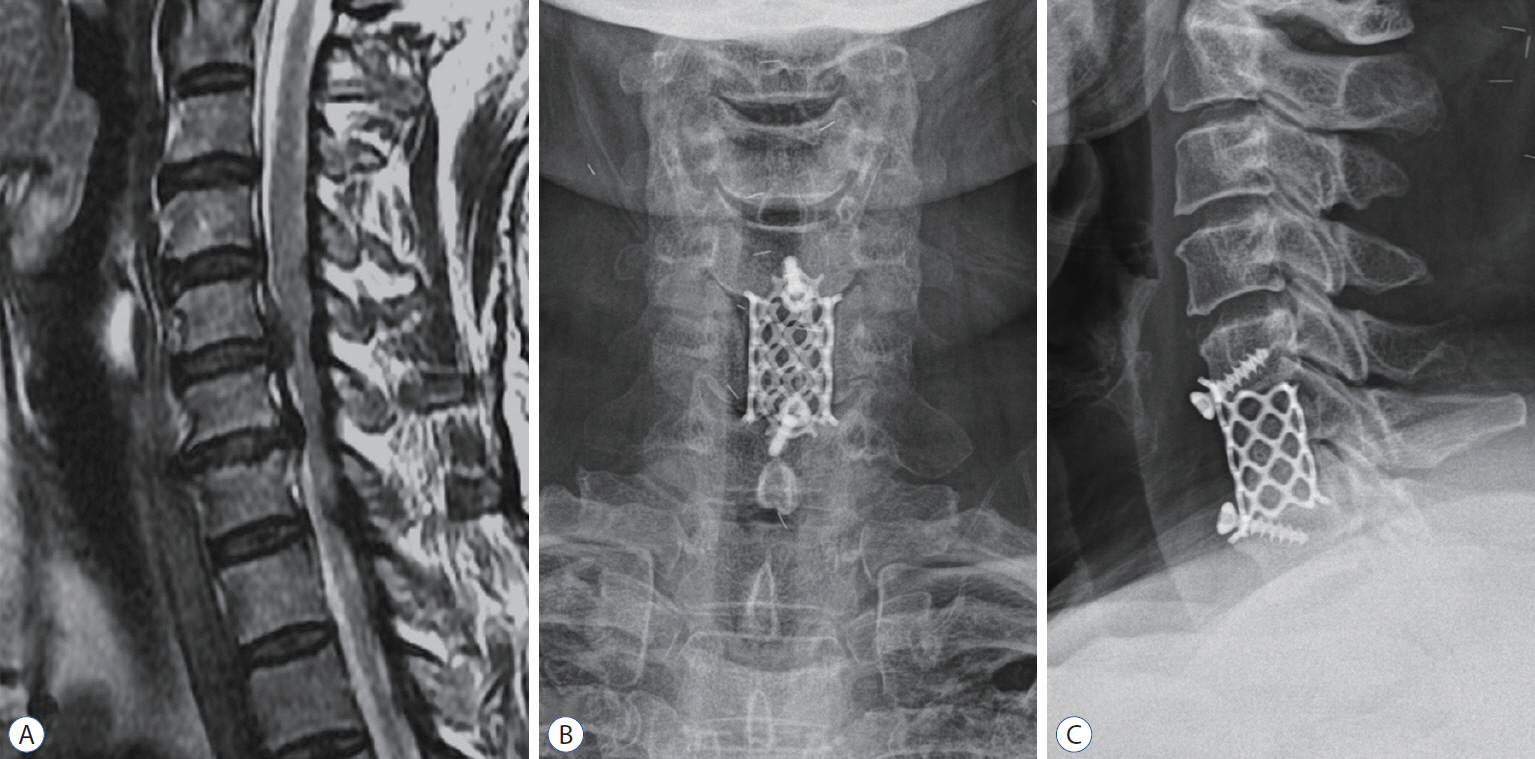
A 56-year-old women present with gait disturbance due to both leg weakness for the 3 months and both hands tingling sensation was started 1 weeks before vising our hospital. A preoperative MRI showed compressive myelopathy at C5/6 and C6/7 due to disc extrusion. We performed a discectomy at C5/6 and C6/7, and total C6 corpectomy. Her symptoms improved to “excellent” after surgery based on Odom’s criteria (Fig. 4).
DISCUSSION
We introduced an innovative cervical reconstruction using a TMC with flanges instead of an additional anterior plate for fixation. The key point of this article is evaluation of flanges and direct screw fixation into the flanged hole at TMC. The flanges play a key role in stability because they are used to position the TMC effectively in the anterior-most portion of the vertebral body. In contrast, the ends of a conventional strut graft lack such protrusions [17]. The location of a strut graft is important to the efficacy of the reconstruction [9]. The outer shell of the vertebra consists of cortical bone that is stronger than the cancellous bone that comprises the inner part of the vertebra. The cortical rim on the upper and lower edges of the vertebra is the strongest portion of the outer shell of a vertebra. The anterior-most location of a strut graft allows maximum contact with the anterior cortical rim, which is undamaged, unlike the posterior part. The posterior cortical rim is often undermined to remove posterior osteophytes or calcified ligaments, which makes the area more vulnerable to subsidence. This minimizes kyphotic angular deformation and subsidence [10]. Graft subsidence can result if a strut graft is located centrally on the vertebral body due to a relatively weak cancellous bone portion. The bone graft in conventional anterior plate fixation may be located slightly more posterior to the anterior vertical line due to the anterior plate. Flanged mesh fixation and fitting at the cortical rim appear to be much easier than fitting mesh without flange.
The screw in conventional anterior plating frequently penetrates the mid-body of the cervical vertebra where the segmental vessels penetrate, and cancellous bone is abundant. We fix a cancellous screw in the cortical margin through the upper and lower holes of the f lange. The screw through the flange directly penetrates the cortical rim. This appears to be effective in increasing postoperative stability and securing the graft because the cortical rim is much stronger than the midportion of the vertebral body.
Screw breakage has been reported in 3.2% to 10% of cases with an anterior plate in the references [15,17]. In this study, screws broke more frequently (n=6, 12%) but did not affect the fusion rate or lead to complications. The role of the screw is to prevent the cage from dislodging only in the early phase of the fusion process. As the fusion progresses, the role of screws diminishes. We demonstrated a case even though the screw is broken, but the fusion is well done (Fig. 5). We use one screw in 42% of the subtotal corpectomy case. The surface of the subtotal corpectomy site which the f langed cage will contact is rough cancellous bone, not the solid endplate. The cage dislocation is not expected without the screw at this subtotal corpectomy site and dislodgement is not occurred in our series even in fixing with one screw (Fig. 5).
We had good overall clinical outcomes with an enough follow-up period. We achieved a 98% fusion rate and satisfactory clinical improvement at the last follow-up evaluation. Of the patients, 19 (38%) were classified as excellent and 25 (50%) as good based on Odom’s criteria. The mean follow-up period was 16.8±13.7 months. Panchal et al. [17] reported the clinical results of 91 patients who had undergone TMC with an anterior plate; of the patients, 27 (33.8%) were classified as excellent and 24 (30.0%) as good based on Odom’s criteria.
Chen et al. [4] reported subsidence in 300 patients who underwent anterior cervical corpectomy with an anterior plate. The cases of subsidence were divided into a mild group (1-3 mm) and a severe group (>3 mm). In total, 182 cases had mild subsidence (60.7%), and the mean was 1.6±0.2 mm. Severe subsidence occurred in 59 cases (19%), and the mean amount was 3.8±0.4 mm. Jang et al. [10] reported anterior and posterior subsidence in 30 patients who underwent anterior cervical corpectomy with an anterior plate. Mean anterior subsidence was 1.4±0.9 mm, and mean posterior subsidence was 2.9±1.2 mm. Zeng et al. [22] reported 35 patients who underwent anterior cervical corpectomy with an anterior plate. Mean subsidence was 2.8±1.3 mm, and the severe subsidence rate was 31.4%. In the present study, mean subsidence was 2.78±2.35 mm, and the severe subsidence rate was 34%. Thus, our subsidence results are like those associated with anterior cervical corpectomy with a plate.
Nowadays we have made several modifications to reduce subsidence. The ends of the cage are bent outward almost horizontally to increase the contact surface. Due to the cervical lordosis and body alignment, the empty space after corpectomy is trapezoid shape, not square which is narrower at the posterior side. Recently, we trim the cage into a trapezoidal shape so that exactly fit into the corpectomy gap. Applying these two modifications, we are expecting the contact area of the cage will be increase and physical pressure will be more evenly distributed and subsidence will be reduced as well [8] (Fig. 6).
The radiological result supported that cervical reconstruction using the flanged TMC instead of an anterior plate has satisfactory mechanical stability and ability to obtain solid fusion. The overall fusion rate was 98% and no pseudoarthrosis. This result is equivalent or superior to the results reported in reconstruction with anterior plate [7,10,17,22]. The subsidence rate was equivalent to reconstruction with anterior plate.
Some authors have suggested that severe subsidence is associated with poor neurological outcomes [4,20,21], whereas others have reported that cage subsidence is not associated with clinical outcome [10,11,22]. In the present study, cage subsidence and clinical outcome were not statistically relevant, but the mean “poor” subsidence was significantly high. Only two patients had poor outcomes and four patients had fair outcomes. This might have become significant with a larger number of patients. We attempted to identify factors affecting subsidence, such as age, follow-up period, and level of corpectomy, but none of the factors was significant.
Complications associated with anterior cervical corpectomy and reconstruction have been well described in the literature, although their reported incidence varies widely among published series [14,17,23]. CSF leakage, hoarseness, and dysphagia are the most common complications [5,18]. CSF leakage is usually treated with a lumbar drain [13]. In the present study, we prescribed bed rest for patients with a CSF leak and achieved successful results. Several complications related to anterior plate were reported from mechanical failure to clinical symptoms [15,18]. Although controversial, some authors suggested implying anterior plate increase chance of dysphasia [18]. In our study, three patients (6%) experienced dysphasia but this resolved spontaneously. Our reconstruction can avoid complication associated with the anterior plate.
C5 palsy is a well-documented complication of cervical spinal surgery. The incidence of this complication is 0% to 30%, depending on the type of procedure and approach [3,17,19]. Various treatments have been suggested for C5 palsy, such as conservative treatment, physical therapy, and a surgical procedure [19]. In the present study, two patients experienced C5 palsy and were classified as “poor” based on Odom’s criteria. A 48-year-old man suffered from right arm pain for 3 years and was diagnosed with OPLL at C4-C5. He underwent a C5 corpectomy, and his symptoms improved. Five months later, he complained of right C5 palsy symptoms, and took a cervical MRI, which showed right C4/5 foramen stenosis. We performed a right C4/5 and C5/6 anterior foraminotomy. The palsy improved after revision surgery. In the other case, a 63-year-old man had right arm pain for 1 month and was diagnosed with CSM at C4-C5. He underwent C5 corpectomy, and his right arm pain improved but the left arm developed weakness. A follow-up cervical MRI and left C4/5 and C5/6 foraminotomy were performed. Right arm weakness occurred 1 month later, and we performed a right C4/5 and C5/6 foraminotomy with an anterior plate. The weakness in both arms improved after surgery. Subsidence and a broken screw occurred in both cases. The first case improved with a foraminotomy alone, whereas the second case required an additional anterior plate. The difference between the two cases was presumed to be osteoporosis. The bone mineral density score of the 63-year-old man was -2.9 T, and fragile bones were observed during surgery. Therefore, we applied an anterior plate to reinforce the osteoporotic bone, and no additional subsidence occurred. Fusion was observed at the last follow-up on cervical X-rays.
CONCLUSION
We evaluated innovative design of flanged TMC for the anterior reconstruction of cervical corpectomy. Using a flanged TMC in anterior cervical corpectomy and reconstruction for OPLL and CSM resulted in favorable clinical outcomes, excellent fusion, and an acceptable subsidence rate. These outcomes indicate that a f langed TMC is an effective graft for cervical reconstruction. This method not only simplifies reconstruction but also helps avoid plate-related complications and could be an alternative option for cervical reconstruction.