INTRODUCTION
Life expectancy has dramatically increased as a result of several factors including improved nutritional support, advanced quality of life, and development of medical and surgical techniques. As the population of the world is aging, the number of patients suffering from lumbar spine disease has increased considerably, especially within the Republic of Korea. In addition, newly developed imaging equipment facilitates more sensitive and wider diagnosis of various disease entities.
The pathophysiologic and anatomic changes associated with the degenerative process include thickening of the ligaments, enlargement or loosening of the facet joints, and loss of water from discs28). These changes may lead to a narrowing of the spinal canal and segmental instability with subsequent compression of the neural elements28). In addition, elderly people are more vulnerable to external forces as a result of senile or postmenopausal osteoporosis, decreased pliability, and weakness of muscle tone. For these reasons, lumbar spinal diseases are commonly observed in the elderly.
Although spinal disorders are not typically regarded as life threatening, they can lead to chronic pain and significant limitation of activity15). Therefore, symptomatic lumbar spinal disease should be treated irrespective of patient age. An accurate assessment of the potential morbidities associated with spinal procedures is necessary to guide treatment41). Conservative treatment such as medication, physical therapy, and steroid injection may relieve the symptoms in some cases48). However, surgical treatment, and even fusion surgery, is typically needed for medically refractory cases with moderate to severe lumbar spinal disease.
The majority of the elderly population has the concomitant problem of associated comorbidities. Advanced patient age, medical comorbidities, nutritional needs, life expectancy, and bone quality are important issues to consider when discussing spine surgery in the elderly. Many previous studies have emphasized the morbidity associated with surgical treatment of lumbar spinal disease in the elderly10,24) and have recommended non-surgical treatment for elderly patients22). Consequently, spine surgery in the elderly has generally been thought to be associated with an increased risk of perioperative complications. However, several authors recently claimed that surgical treatment of the elderly is both safe and efficacious because of newly developed surgical techniques and improved instruments36,45). Ragab et al.36) studied the safety and outcome of lumbar spinal surgery in patients 70 years of age or older and found that surgical treatment of lumbar spinal diseases in the elderly has a high success rate and satisfaction level, with results comparable to those in a younger population.
Many previous reports focused on outcome assessments of specific procedures or diagnoses or outcomes as a function of age distribution19,37,39,40). This study systematically analyzed previously reported risk factors in Korean patients. The aim of the study was to examine perioperative complications and assess the risk factors associated with lumbar spinal fusion, focusing on geriatric patients at least 70 years of age.
MATERIALS AND METHODS
Patient population
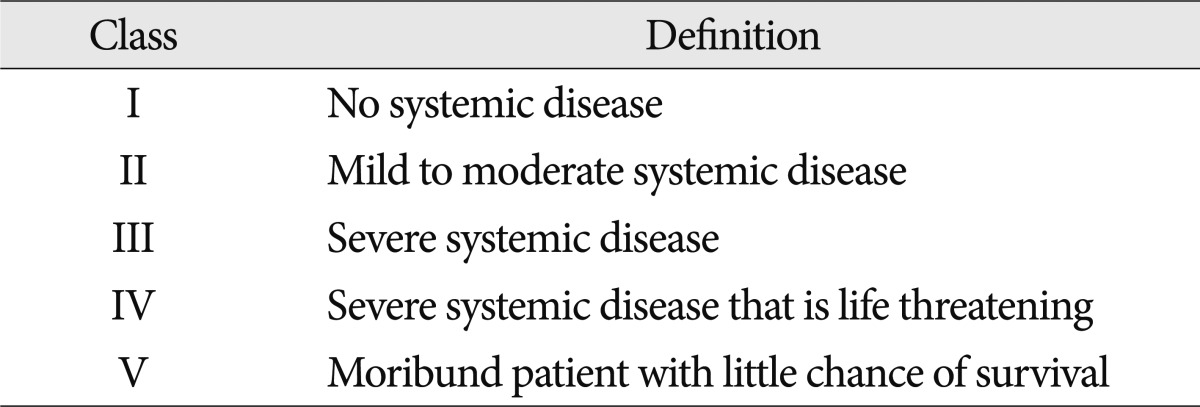
The present study included 489 patients who underwent lumbar spine fusion surgery (LSFS) from 2003 to 2007. Exclusion criteria were age between 66 and 69 years, decompression only, anterior interbody fusion, a follow-up period less than 12 months, and severe co-morbidity [American Society of Anesthesiologists (ASA) classification of physical status >III] (Table 1). LSFS was performed by one neurosurgeon at a single institute, Hanyang University Medical Center. The patients were divided according to the definition of 'geriatric' into group 1 (older than 70 years) and group 2 (younger than 65 years). We enrolled patients with various preoperative diagnoses including degenerative spine disease, spine trauma, and revision surgery after the previously mentioned diseases, and excluded patients suffering from spine tumors to avoid unexpected co-morbidities. Data related to these patients were evaluated by a single observer using the standard hospital chart, outpatient notes, electronic medical records, operative reports, and preoperative and postoperative imaging studies. The following demographic variables were evaluated : principal diagnosis, previous spine surgery, treatable or non-treatable medical co-morbidities, bone mineral density (BMD), surgical approach, and segment of fusion.
Radiological evaluation
Preoperative plain radiographs including anteroposterior (AP), lateral, both oblique, and dynamic views (flexion and extension) were obtained for all patients except those with traumatic lesions, who were evaluated with only AP and lateral views. Additionally, all enrolled patients underwent magnetic resonance imaging and computed tomography (CT) scanning of the lumbar lesion preoperatively. Plain radiographs with AP and lateral views were obtained immediately after surgery, and then at 1, 3, 6, and 12 months thereafter. Additional CT scans were performed as follow-up to evaluate perioperative complications as needed.
Co-morbidities
All patients were evaluated for co-morbidities such as cardiovascular, renal, pulmonary, and endocrine problems. Co-morbidities were subdivided as follows : cardiovascular (hypertension, coronary artery disease, and congestive heart failure), renal disease (renal cyst and acute or chronic renal failure), pulmonary (chronic obstructive pulmonary disease and asthma), endocrine (hyperthyroidism, hypothyroidism, and diabetes mellitus), liver disease (fatty liver, liver cyst, hepatitis, liver cirrhosis), rheumatoid arthritis, peptic ulcer disease, and others.
Surgical treatment
We performed several types of fusion surgery according to the patient's lumbar spine disease. In general, surgery was performed in degenerative cases when conservative treatment over three months failed to improve the patient's symptoms. We used three different surgical approaches: trans-pedicular screw fixation (TPSF), posterior lumbar interbody fusion (PLIF), and a combined approach. In the present study, all techniques were used interchangeably by the two neurosurgeons. In patients who only underwent TPSF, postero-lateral fusion was simultaneously performed at the intertransverse process space with autologous lamina bone and an allograft.
Postoperative care
Patients were ambulated from postoperative day 2 with a rigid molded plastic brace or lumbar corset. Patients were initially treated with analgesia for control of acute pain by intravenous injection, and then quickly weaned to mild oral narcotic therapy and NSAIDs that were discontinued as soon as possible.
Complications
The term "complication" is broadly and differently defined in the published literature. In this study, a complication was defined as any event requiring specific management during the perioperative period, including the intra-operative and post-operative periods. Based on a PubMed search of previous literature with the keyword "complication," we considered the following to be complications : intra-operative complications such as dura tear, and postoperative complications including infection, spondylitis, hematoma accumulation, wound dehiscence or infection, mal-position of instrumentation, and aggravated neurologic symptoms when compared with preoperative status. However, postoperative systemic complications such as pneumonia, bowel ileus, or renal failure were excluded because they could be caused by any surgery with general anesthesia. All complications were verified by retrospective chart reviews. In addition, any need for reoperation during the follow-up period was noted, and the reason was recorded.
Evaluation of outcome
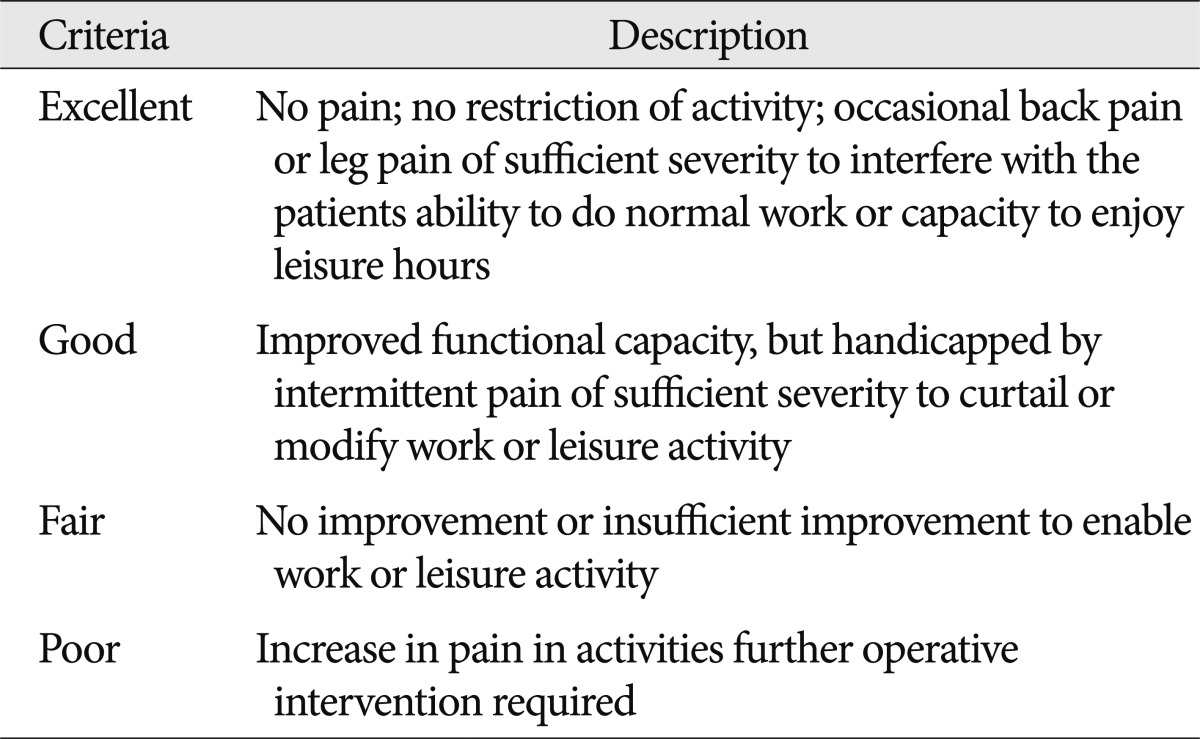
The patients enrolled in the present study were followed up for at least 12 months postoperatively. To evaluate objective neurologic improvement, we used the visual analogue scale (VAS) and MacNab's criteria (Table 2).
Statistical analysis
Several univariate statistical analyses were performed to estimate the association among various factors as follows : Student's t-test for the analysis of relationships among BMD, age, and sex; chi-square test for age and underlying disease; and logistic regression models to determine the relationship between age and other factors with the occurrence of complications. Finally, we used binomial univariate logistic regression analysis to evaluate the correlation between the occurrence of complications and age, sex, preoperative diagnosis, comorbidities, ASA class, and procedural details. p-values <0.05 were considered statistically significant.
Variables significant on univariate analysis were further tested in multivariate logistic regression models. Multivariate generalized linear models were applied to assess the statistical significance of each individual variable while adjusting for other covariates. p-values <0.05 were considered significant. Because the focus of the present study was elderly patients, age was kept in the regression model throughout regardless of its significance. For each variable, ORs and 95% CIs were calculated. A predetermined subset analysis was performed to characterize complication rates according to age and to identify specific risk factors. Descriptive and procedural information were compiled, and complication rates were calculated according to the previously described definition. Univariate and multivariate logistic regression analyses were used to identify factors associated with complications in elderly patients. All statistical analyses were performed with SPSS statistical software version 16.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient population
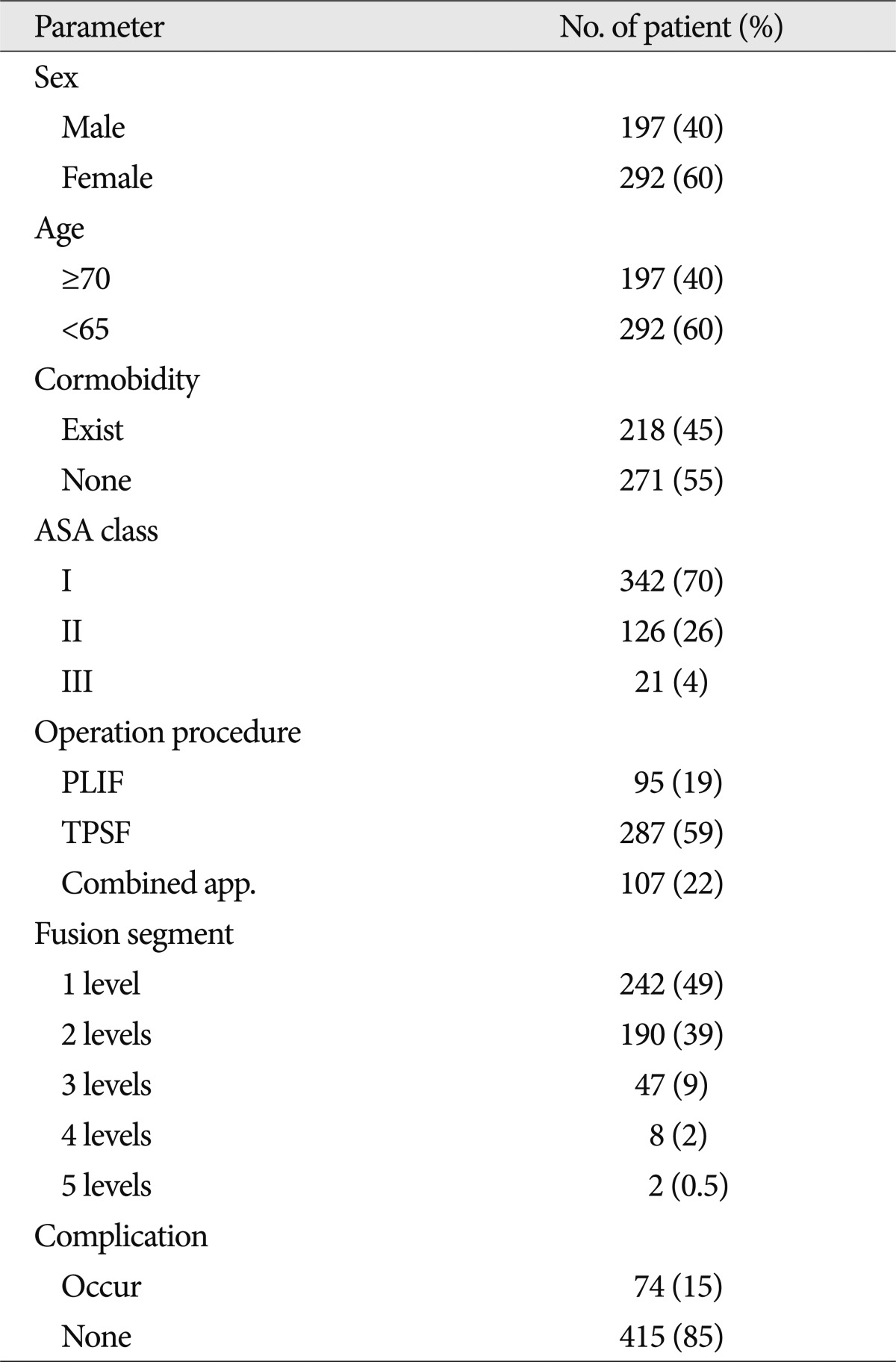
During the five-year study period, 489 patients who met the inclusion criteria underwent instrumented fusion surgery (Table 3). Of these, 197 patients (40%) were male and 292 (60%) were female, and there were 197 patients (40%) in group 1 and 292 patients (60%) in group 2. The mean age was 57.8 years (group 1, 58.27 years; group 2, 75.91 years). The general condition of most patients was ASA class I (342 patients) or II (126 patients) with a few patients in ASA class III. The distribution of surgical procedures was as follows : 287 patients (59%) with TPSF, 95 patients (19%) with PLIF, and 107 patients (22%) with combined procedure. Single-level fusion surgery was performed in 242 patients (49%) whereas the remainder underwent a multi-segment procedure. The average fusion segment length was 1.64 segments. The most commonly treated levels were L4-5 and L3-4. Additionally, 45% of patients had comorbidities, and complications were encountered in 74 patients (15%).
Comorbidities
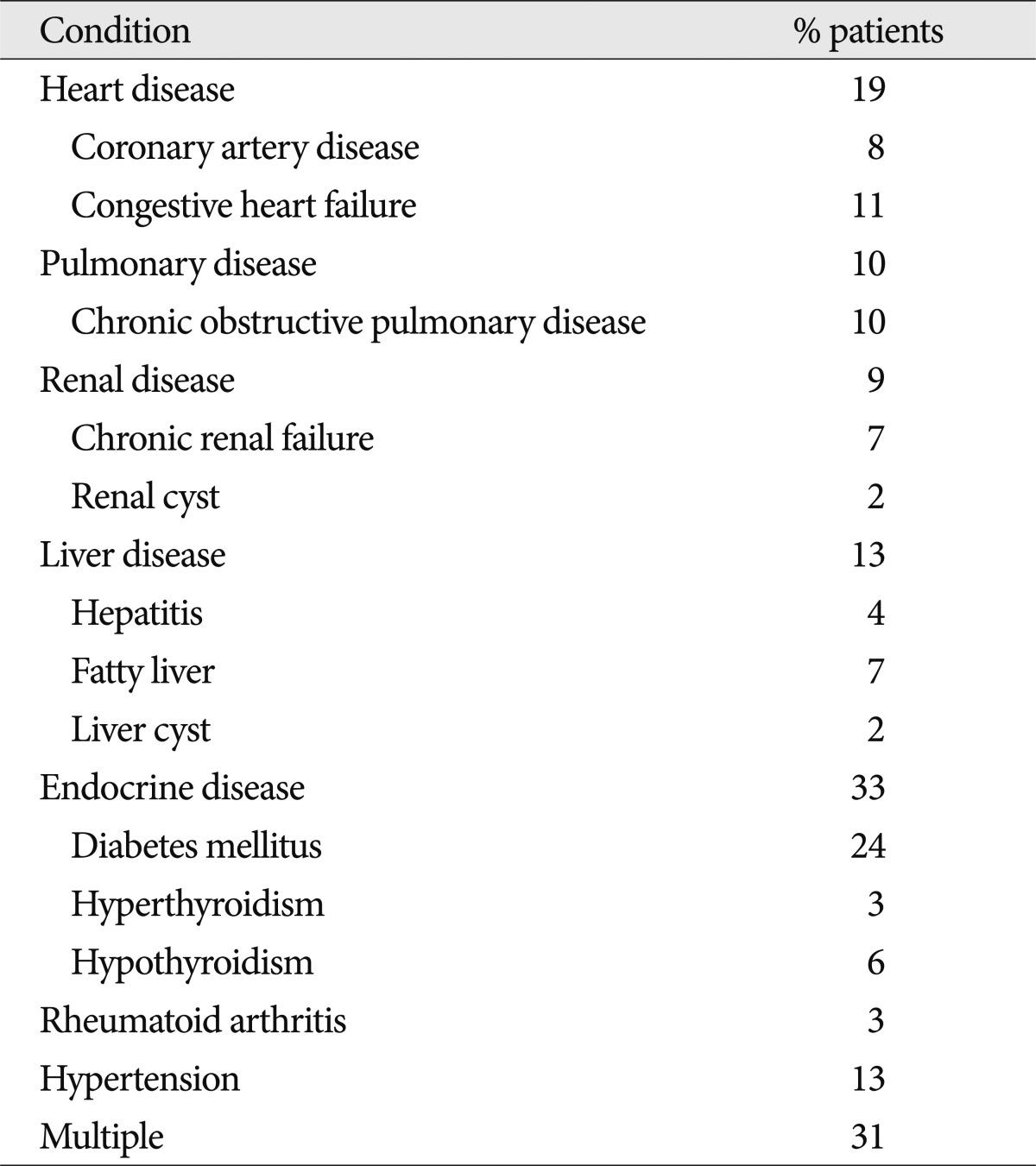
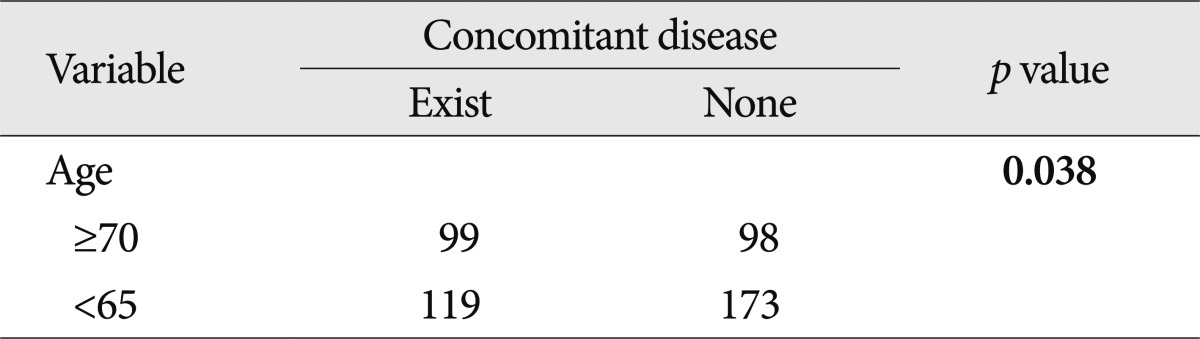
Among the observed comorbidities the most common problem was endocrine disease, which was present preoperatively in 33% of the patients. Endocrine disease was subdivided into diabetesmellitus (24%), hypothyroidism (6%), and hyperthyroidism (3%). Other comorbidities were cardiovascular disease (19%), hypertension (13%), liver disease (13%), pulmonary disease (10%), and renal disease (9%). In addition, 31% of the patients had more than one comorbidity (Table 4). We also estimated the correlation between age and underlying disease. Almost half of the geriatric patients had underlying diseases and there was a statistically significant association between age and underlying disease (p=0.038) (Table 5).
Complications
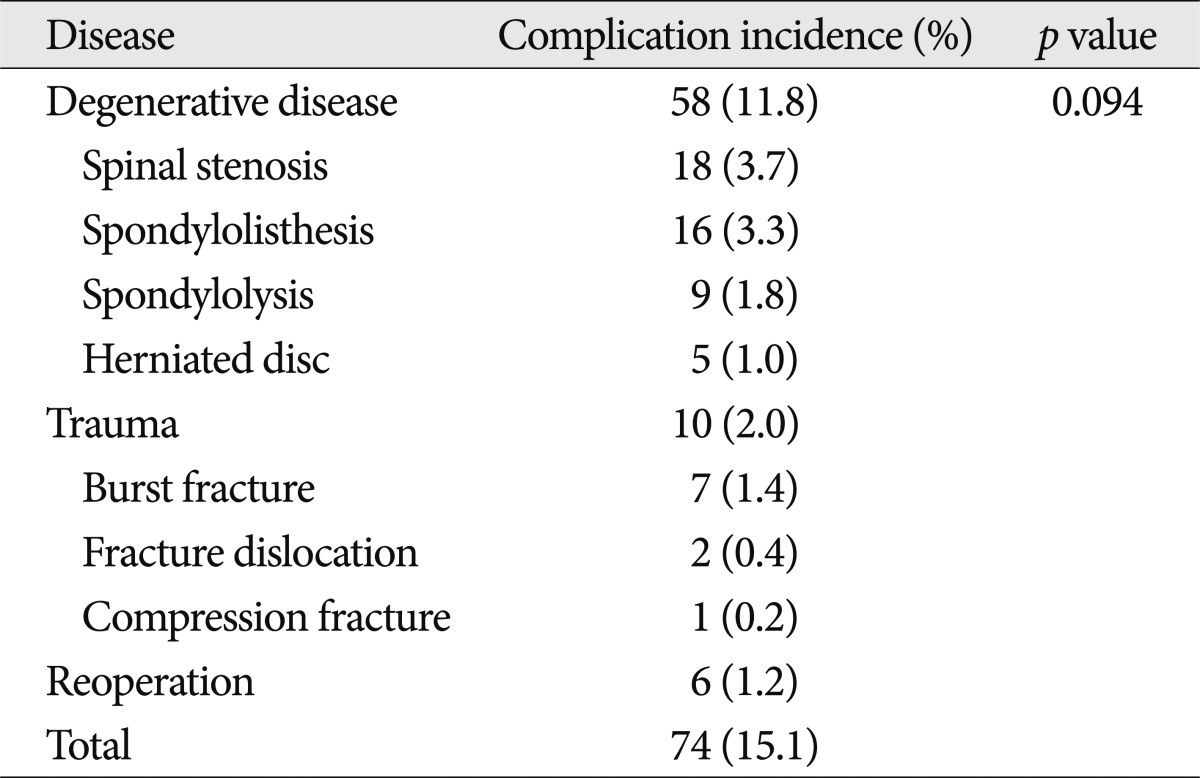
Although there was a trend toward increased incidence of complications in patients who underwent surgery for degenerative disease, there was no statistically significant correlation between diagnosis and overall complications. The overall incidence of degenerative disease, trauma, and reoperation was 11.8%, 2.0%, and 1.2%, respectively (Table 6).
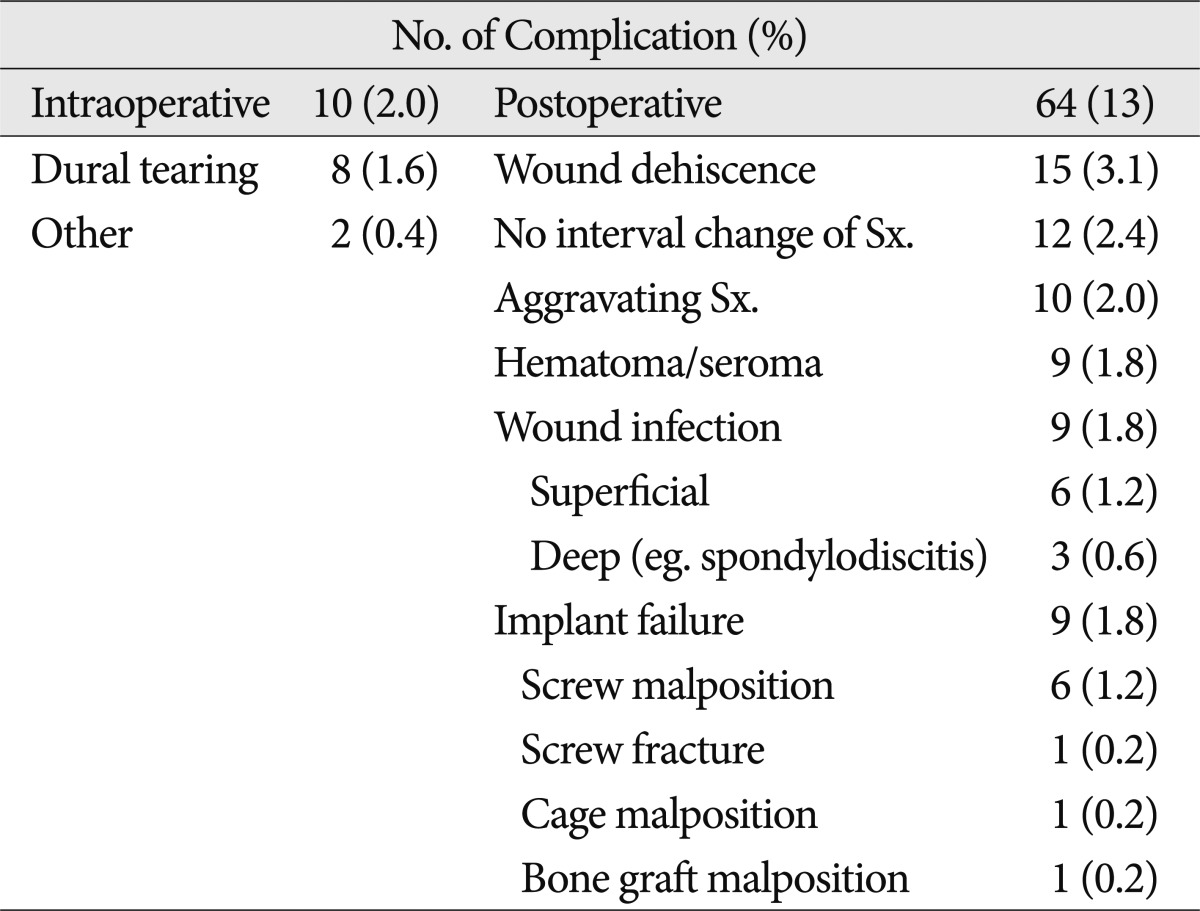
Complications arising in the 74 patients are listed in Table 7. Intraoperative dura tearing occurred in 2.0% of the patients. The total postoperative complication rate in all patients was 13%, and the overall peri-operative complication rate in patients 70 years of age or older was 9%. Among these complications, 35 cases were re-treated (6 cases of dura tearing, 12 cases of wound dehiscence, 4 cases of hematoma accumulation, 6 cases of wound infection, and 7 cases of implant failure).
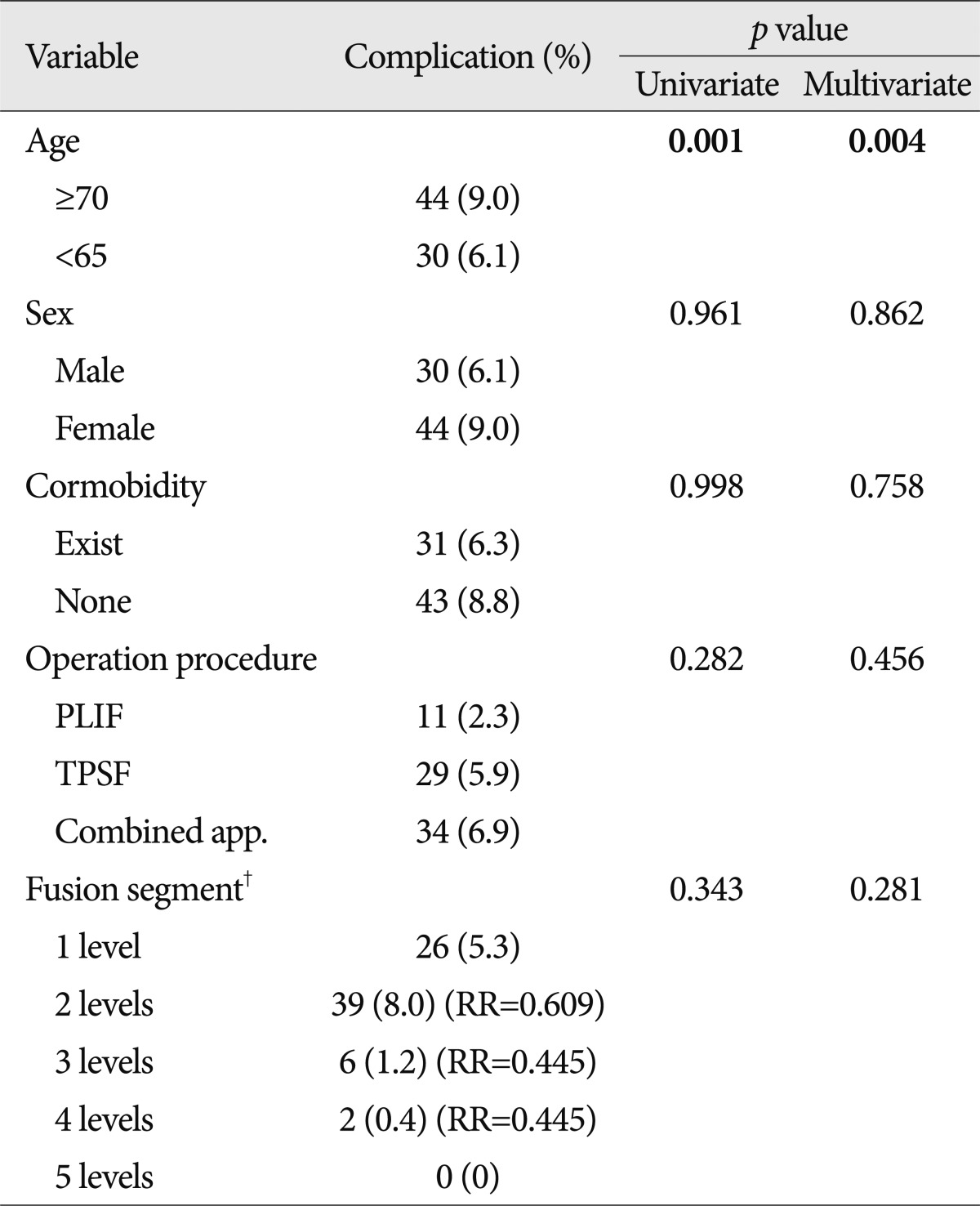
The results of the logistic regression analysis are displayed in Table 8. Age was the only statistically significantly factor in both univariate and multivariate analyses (p=0.001 and 0.004). Other factors such as sex, comorbidities, and operation procedure were not statistically significant. In addition, a greater number of fusion segments was not predictive of complications.
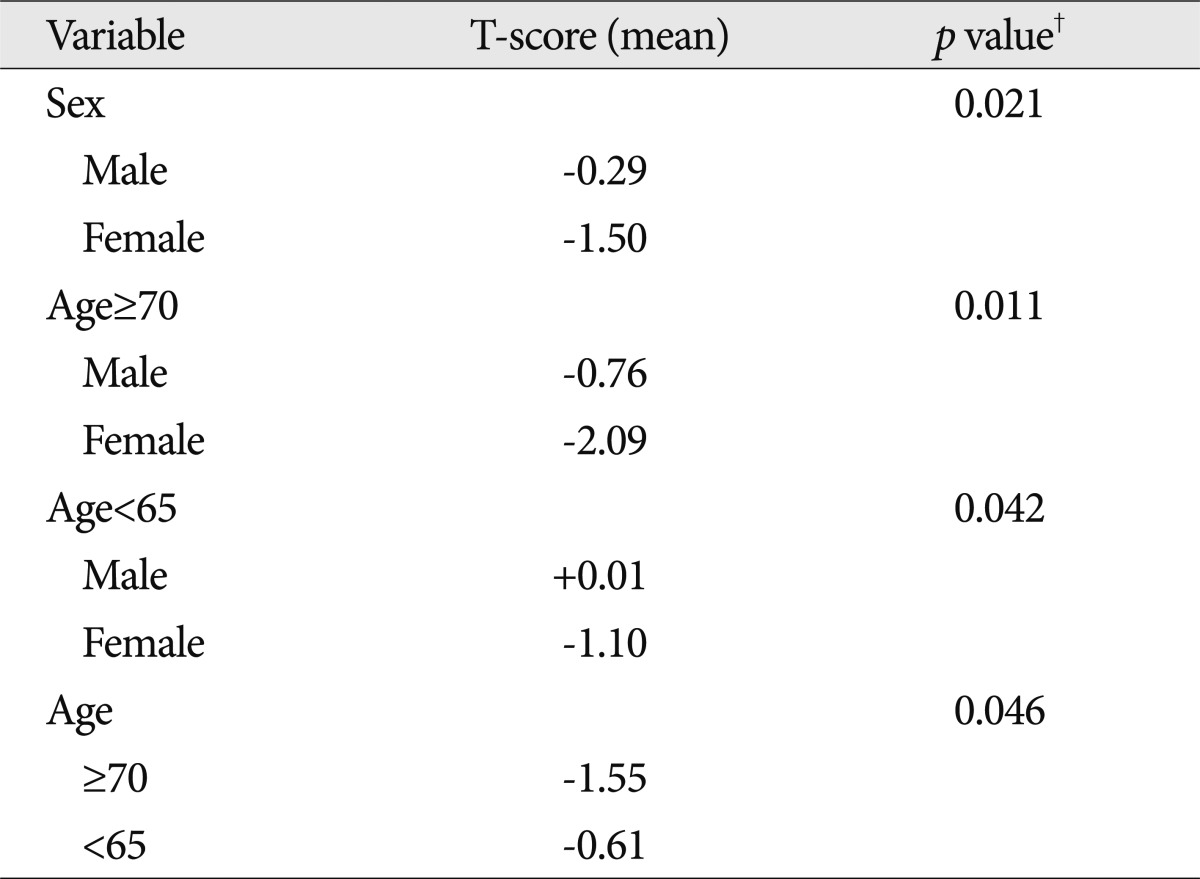
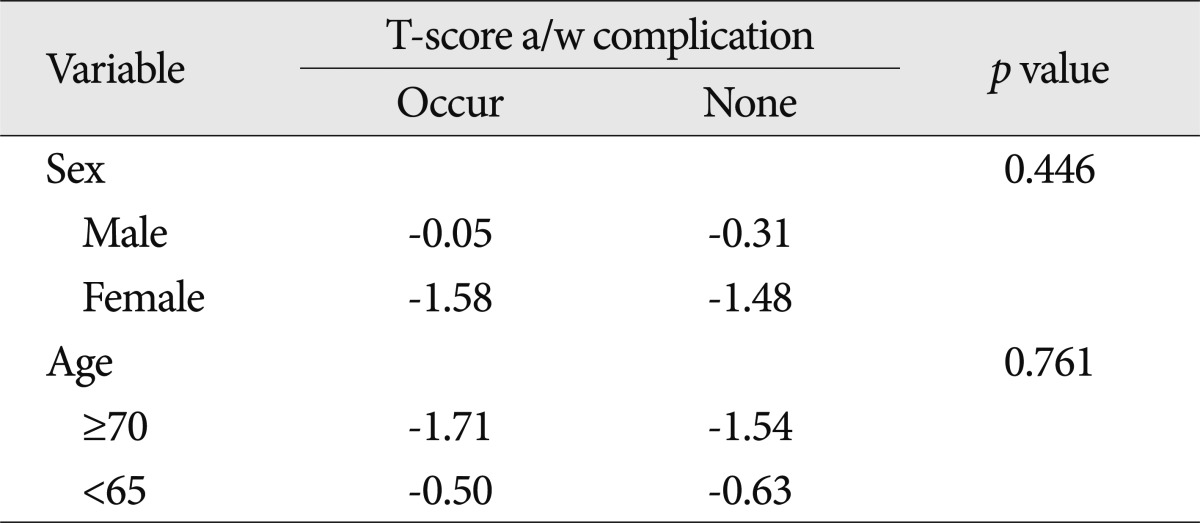
Osteoporosis
According to the present data, older patients and female patients had a lower T-score than younger patients and male patients on univariate analysis (Table 9). However, there was no statistically significant relationship between low bone mineral density and perioperative complications (p=0.446 for sex and 0.761 for age) (Table 10).
Neurologic symptoms
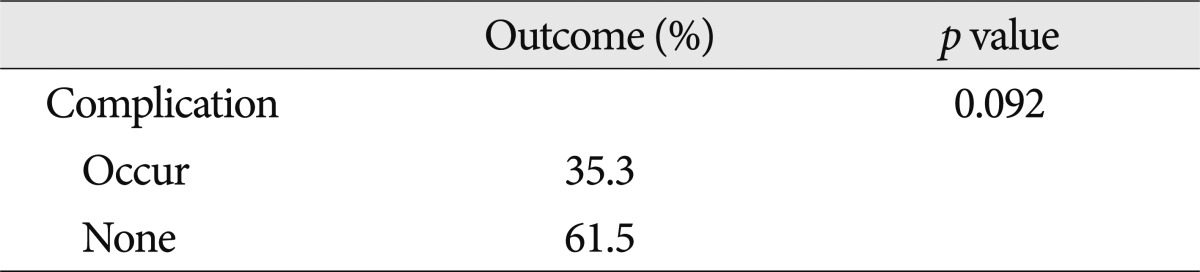
Preoperatively, the mean VAS was six points in geriatric patients and seven points in younger patients. However, the final VAS was two in older patients and one in younger patients. There was a statistically significant difference between the two groups. Based on the mean MacNab criteria, both groups had good outcomes (Table 11). Worsening or maintenance of the preoperative status during the course of the follow-up period was seen in 17 (3.4%) of the 489 patients and was generally attributed to back pain, radiating pain to the leg, or neurogenic claudication. The remaining patients had relief of approximately 57.5% of their symptoms compared with preoperative status. There was no significant correlation with age, comorbidities, operation procedure, and fusion segment. In addition, there was no statistically significant relationship between perioperative complications and neurologic outcome (p=0.092) (Table 12).
DISCUSSION
The number of elderly persons in the Republic of Korea continues to grow, with an expected 38.2% of people older than 65 years by the year 2050. This greatly exceeds the worldwide mean of 16.2%. An aging population will suffer from age-related degenerative diseases, such as disorders of the spine. Today, elderly people live longer, have more active lifestyles, and have a great desire to be pain free throughout the last decades of life. Advances in anesthesiology, spinal instrumentation, and post-operative care have made spinal procedures safer, with a decrease in morbidity and mortality and improved patient outcomes7). Additionally, they have allowed more extensive and complex procedures to be performed in at-risk populations, such as the elderly7). Identifying predictors of complications or poor outcome in the geriatric population is important for perioperative risk assessment and for implementing appropriate preventative measures.
There is no standard definition of "complication" in the spine literature37). Various classification systems have been used, often to suit the investigator, making analysis and comparison of the literature difficult8,37,39,43). In the current study, a previously validated classification of complications was not used. Most previous studies in the literature used a binary system, and included systemic complications associated with surgery38). In the present study, however, we did not choose a binary system of complications and excluded systemic complications because it was unclear whether systemic complications occurring in the perioperative period were related to spine surgery. The incidence of complications in this current analysis was 15.1%, which is a little lower than that in several previous retrospective studies2,10,33,46). In a review of 105 spine surgery articles, Nasser et al.30) reported an overall pooled complication incidence of 16.4%. The most common perioperative complication observed in this study was wound dehiscence, at a rate of 2.6%, while laceration of the dura was the most common intraoperative complication (1.6%). Reoperation after spinal fusion surgery may be considered a failure of the initial surgery by the patient and surgeon and represents an additional procedure in patients who are already at significant risk for complication7). Mok et al.27) recently evaluated the need for revision surgery in patients undergoing adult spine surgery, finding a cumulative rate of 25.8%, while Cloyd et al.7) reported a reoperation rate of 27.4% in patients at least 65 years old who presented with a wide range of spine pathologies. In this study, the rate of revision surgery due to complications was approximately 47%, but age was not associated with the need for reoperation.
Cloyd et al.7) found that age is a risk factor for major postoperative complications with an OR of 1.04 (p=0.039). A ten-year increase in age is associated with a 48% greater risk for a major postoperative complication. An alarming 24.2% of elderly patients incur a major postoperative complication and 53.2% experienced at least one in-hospital complication. The rates of complications for spinal arthrodesis in elderly patients are highly variable, ranging from 14 to 80%4,5,26,31,35). Okuda et al.31) found that patients older than 70 years who had undergone posterior lumbar interbody fusion for spondylolisthesis had a complication rate of 16%, which was not significantly different from that in younger patients; however, these authors admittedly excluded minor complications from their analysis. Kilinçer et al.26) also found that age did not affect the complication rates of posterior lumbar interbody fusion, but they did not report a complication rate separately for older patients. Vitaz et al.45) found that elderly patients with lumbar spinal disease can be surgically treated in a similar fashion to younger patients. On the other hand, Deyo et al.10) retrospectively analyzed a statewide hospital discharge registry and compiled data on more than 18000 hospitalizations over a two-year period. Patients with nondegenerative pathologies were excluded from the analysis. These authors reported an overall complication rate of only 10.3% for the surgical treatment of degenerative lumbar spine disease, although the rate for patients older than 75 years was higher (18%). Our data also showed a difference between the older and younger groups; the complication rate of the older group was 9%, while that of the younger group was 6%. There was a statistically significant association between age and perioperative complications (univariate analysis, p=0.001; multivariate analysis, p=0.004).
The relationship between comorbidities and surgical outcome has historically been controversial. Early studies investigating the effect of age on decompression with fusion for lumbar stenosis found that the presence of multiple comorbidities was associated with perioperative complications24,32,43). Katz et al.24) found that greater cardiovascular, musculoskeletal, and overall comorbidities led to poorer scores in most of the outcome measurements. However, for lumbar spinal fusion in the elderly, several recent studies have found the opposite to be true1,2,4,5,26). Although Daubs et al.9) did not find an association between comorbidities and complications, it is unclear whether they only studied the effect of individual diseases or the total number of comorbidities. The results of our study indicate that for lumbar fusions in the elderly, the number of comorbidities is not associated with perioperative complications (univariate analysis, p=0.998; multivariate analysis, p=0.758).
Sanjay et al.47) found no correlation between diagnosis and overall incidence of complications (p=0.08), although a trend toward increased complications in patients undergoing surgery for neoplastic or infectious pathology was observed. In this subset of the patient population, patients with preoperative diagnoses of infection and neoplasm were more often affected by isolated and multiple complications (p=0.05 and p=0.02, respectively). Patil et al.33) reviewed 26233 admissions for patients with surgically managed spine metastases from the National Inpatient Sample, a public database maintained by the Agency for Healthcare Research and Quality and found a higher complication rate in elderly patients. In this series, however, there was no statistically significant association between primary diagnosis and the rate of complication (p=0.094). Previous studies have suggested a higher incidence of complications with revision surgery compared with primary surgery2,18,43), possibly because scar tissue from the previous surgery may deform anatomy and increase the risk of injury to vascular structures, soft tissues, or visceral organs8). It may also affect wound healing and increase the risk of surgical site infections. Sidhu et al.43) found that the complication rate of revision lumbar surgery was three to five times higher than the reported rates for primary surgery. In that study, the overall complication rate for revision surgery at the same operative level was 42%. However, in the current study, the complication rate of 1.2% for reoperation was lower than that for primary surgery (14%).
Several studies have shown increased rates of complication with fusion versus non-fusion procedures6,16,23). Fusion and instrumentation surgeries are generally more complex than non-fusion surgeries and the potential for injury and infection may be greater41). However, the indications for lumbar fusion in the treatment of spine segment instability due to various causes remain controversial11). Our indications for lumbar spinal fusions have included severe low back pain25,49), mechanical or iatrogenic spinal instability3,14,18), degenerative spondylolisthesis12,13,29,34,44), and traumatic lumbar spinal injury. In our practice the decision to perform spinal fusion with instrumentation is based on the individual patient. Part of this consideration includes the patient's overall health status and ability to withstand a longer operation. Some authors believe that pedicle screw or rod fixation-type fusion procedures have become the gold standard for arthrodesis11). These procedures obviate the extensile exposure required for intertransverse fusion procedures and require less bone graft material, thereby minimizing donor-site morbidity and complications. It has also been proposed that interbody fusion offers restoration of load-bearing capacity to the ventral spinal column and maintenance of interspace disc height, and that the smaller exposure results in fewer complications11). In this study, a significant association was not detected between fusion type and risk of perioperative complications in patients of all ages, including the elderly (univariate analysis, p=0.282; multivariate analysis, p=0.456).
Elderly patients who present with symptomatic spinal pathology may require single or extensive lumbar fusions to ensure adequate fusion and prevent future instrumentation-related complications7). Several studies have suggested that longer fusion lengths lead to an increased risk of complications in the elderly4,5,35). Carreon et al.4) found an OR of 2.4 for postoperative complications in older patients undergoing lumbar arthrodesis with instrumentation. Similarly, Casinelli et al.5) found that fusion of four or more segments was predictive of complications. The mean number of levels fused in these studies was 2.4 and 1.9, respectively. On the other hand, Daubs et al.9) studied patients older than 60 years who underwent spinal arthrodesis with a mean of 9.1 levels fused and found no association between the length of fusion and complication risk. Moreover, Glassman et al.17) found that extending the fusion length may actually offer improved clinical outcomes in the setting of poor sagittal balance or spinal cord compression. Elderly patients may require extensive multilevel thoracolumbar spinal fusion procedures for a variety of indications, such as to restore sagittal balance, revise failed constructs, debride infections, or resect large spinal tumors7). In our study, there was no significant association between the number of segments fused and the risk of perioperative complications in patients of all ages, including the elderly (univariate analysis, p=0.343; multivariate analysis, p=0.281). We therefore believe that the number of fusion segments may be not significantly associated with perioperative complications in lumbar spinal fusion surgery, therefore fusion extension should be determined by the surgeon as the occasion demands.
While the findings of the current study are important, there are several limitations. First, this study is a retrospective analysis, for which the limitations are well known. Retrospective studies may underestimate the actual complication incidence through the introduction of investigator recall bias21,42). A disproportionate reliance on the memory of different investigators and the accuracy of medical records may lead to falsely low reported rates of complication21). Differences in the interpretation of the patients' degree of pain and neurologic examinations may also lead to a biased result. Second, there are several other opportunities for bias in the present study. There was significant case complexity in our patient population; thus the current study population may not represent the spine surgery population as a whole. Therefore, these findings may not be generalizable to a wider group of spinal fusion surgery patients. Third, we used our own definition of spinal fusion surgery complications. This definition may not represent the views of all spine surgeons, and inclusion of adverse medical events may not be an acceptable methodology to the general spine surgery community.
CONCLUSION
The number of spinal fusion surgeries performed for lumbar spinal disease has increased due to improved surgical techniques and advances in medical treatment, including anesthesia. However, various complications are associated with fusion surgery. The incidence of complications in this series is similar to that in previously published papers. In this study, increasing age was an important risk factor for perioperative complications in patients undergoing lumbar spinal fusion surgery. There was no significant difference between the various procedures in terms of outcome. The general condition of patients with respect to a number of chronic diseases did not affect the risk of perioperative complications. An important finding of the present study is that the occurrence of complications did not affect clinical outcome. Therefore, if good clinical judgment and careful patient selection are applied, fusion surgery may be performed in geriatric patients, even in those with many concomitant diseases.