INTRODUCTION
Acute subdural hemorrhage requires emergent neurosurgery or close observation because of its high mortality rate. It may take several weeks or months for spontaneous resolution without neurosurgical interventions. A number of cases who showed rapid resolution of acute subdural hemorrhage with neurological improvements have been reported2,6,7). Herein, we present a case who showed rapid resolution of acute subdural hemorrhage spontaneously within 2 days after severe head injury.
CASE REPORT
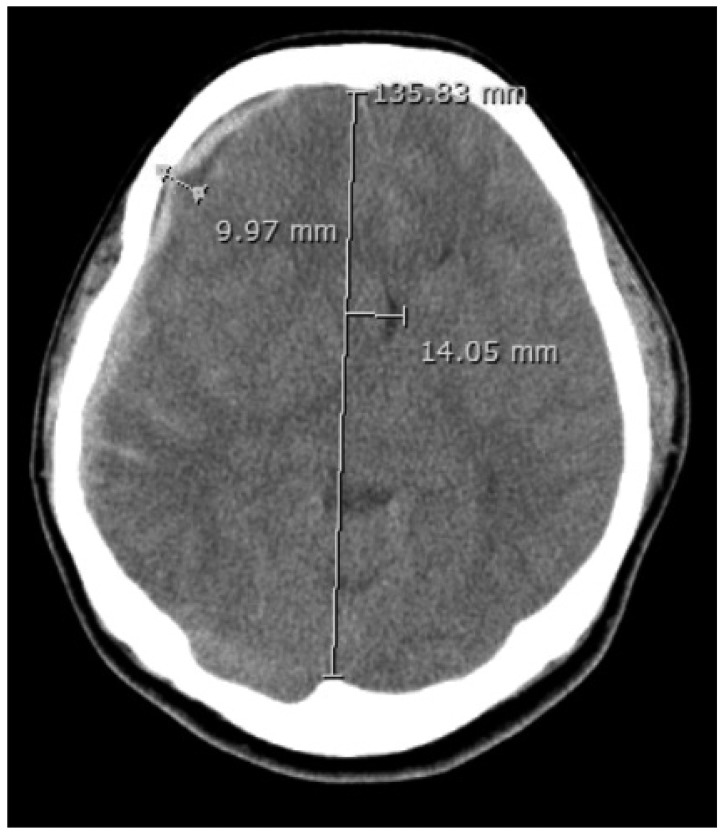
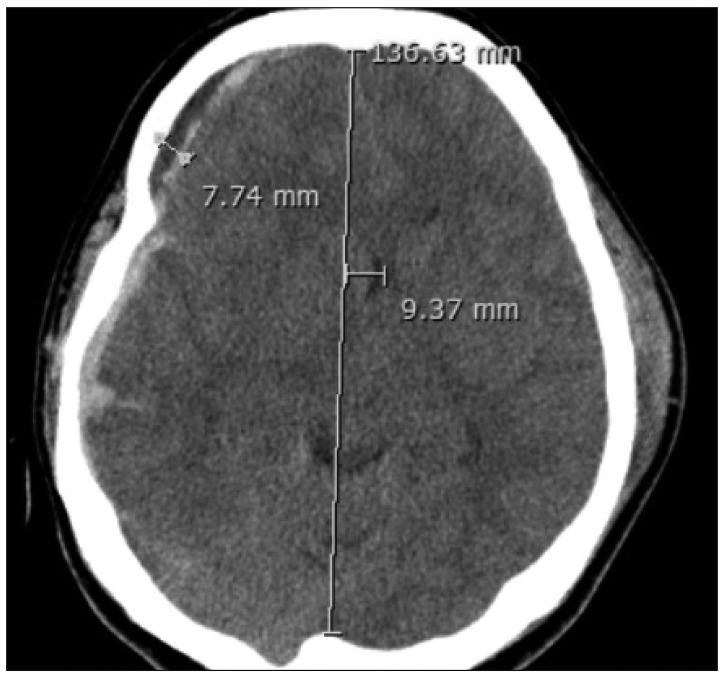
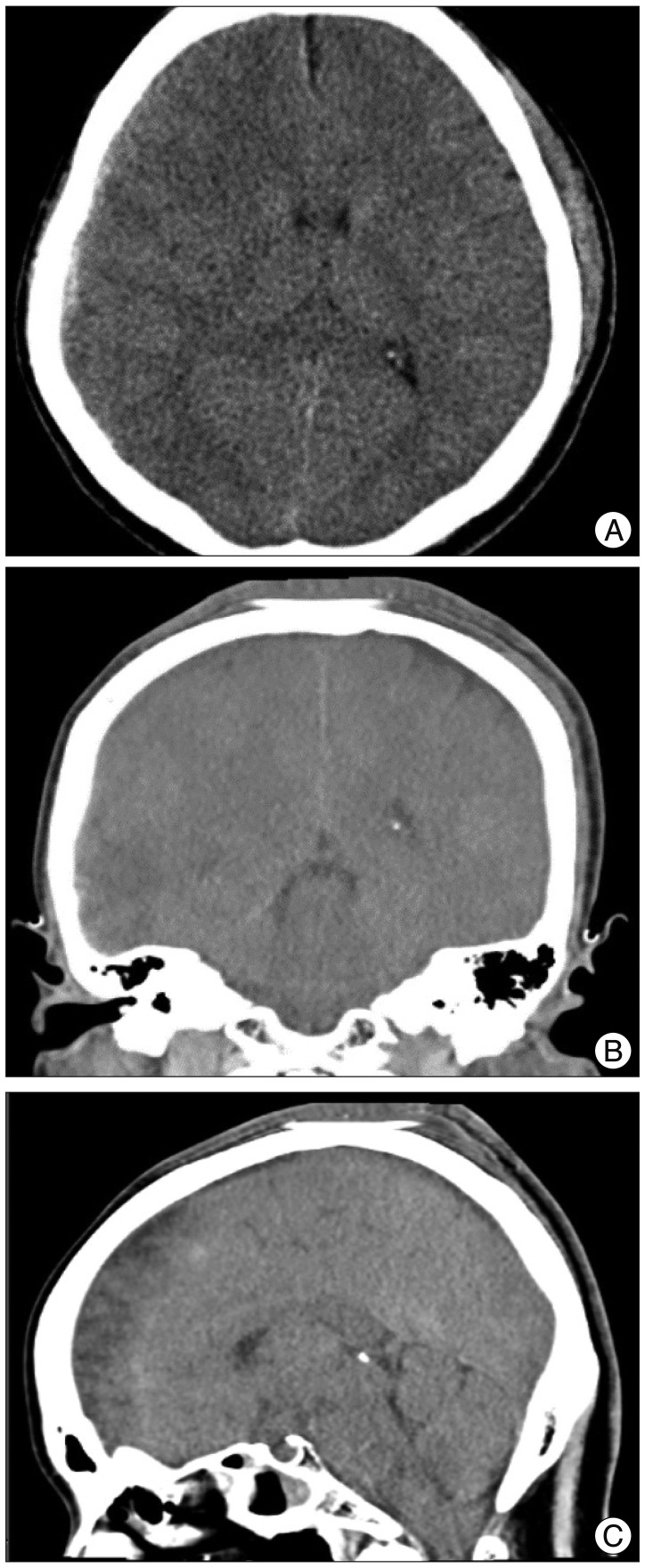
A 40-year-old female patient presented with decrease of consciousness following accident. Initially, she was stuporous and measured as glasgow coma scale (GCS) score of 6. Both pupils were dilated as 5 mm and reactive to light. Brain computed tomography (CT) revealed an acute subdural hematoma with a thickness of 10 mm in the right frontotemporoparietal region. Midline shift caused by mass effects was 15 mm (Fig. 1). Craniotomy for hematoma removal was considered during close observation. However, an unexpected neurological improvement was noted within 1 hour following the accident. The patient was obeyed and GCS score was 10 even though intubated. A follow-up brain CT showed a decrease in the thickness of hematoma and improvement of the midline shift (Fig. 2). On the third day following the accident, brain CT showed a remarkable reduction of acute subdural hematoma and mass effect. The hemorrhages of subdural space around falx, tentorium, posterior fossa, and upper cervical spinal canal were not found (Fig. 3). The patient recovered her consciousness completely without any neurosurgical interventions.
DISCUSSION
Acute subdural hemorrhage is a frequent brain insult resulting from head injury. Usually, it requires emergent neurosurgery for decompression or close observation because of the possibility of irreversible brain damages or abrupt neurological deteriorations. Rapid resolution of acute subdural hemorrhage resulting in neurological improvement is uncommon and several reports about that have been documented2,6,7). Wen et al.7) summarized some characteristics in most patients who showed rapid resolution of acute subdural hemorrhages as followings : transitory coma which last no longer than 12 hours, exclusion of cerebral contusion, widely distributed hematoma with thin width, a band of low density between the hematoma and inner table of the skull on images, a minor or moderate head trauma sustained on insults. In our present case, similar clinical findings were found except for minimal contusion of left temporal lobe. Several theories have been proposed to explain rapid resolution of acute subdural hemorrhages. Flow of cerebrospinal fluid (CSF) through the arachnoid membrane tear site and retrograde flow into the subarachnoid space may result in dilution of the hematoma5). A low density band in the subdural hematoma which is seen on the images seems to mean CSF that comes from the subarachnoid space through arachnoid membrane tear. Redistribution of the hematoma towards another subdural space or extracranial spaces through the skull fracture site can be another acceptable explanation1,4). Our present case did not show definite skull fractures or hemorrhages in another subdural space except for minimal cerebral contusion was found. So, it is thought that the dilution of acute subdural hematoma caused by CSF flow is more consistent with our case rather than redistribution of hematoma. Brain swelling caused by cerebral contusion may contribute the redistribution of hematomas resulting in rapid resolution of subdural hematomas3). However, it is more likely to obstruct CSF circulation and would mitigate the dilution and redistribution1). As seen in our case, minimal cerebral contusion dose not seem to influence the obstruction of CSF circulation. It is very difficult to predict the rapid resolution of acute subdural hematoma which may undergo prompt neurosurgical treatment. Therefore, meticulous observation and concomitant imaging should be required even though some characteristics which may develop rapid resolution of acute subdural hematoma were seen.